ALTR | Pseudotumor | Metal Ion Toxicity | Surveillance and Revision
- Cobalt greater than 7 ppb = concerning, warrants further investigation and surveillance
- Cup inclination greater than 55 degrees = edge loading, accelerated wear and ion release
- MARS MRI = Metal Artifact Reduction Sequence for soft tissue assessment
- ALTR = Adverse Local Tissue Reaction (umbrella term for all MoM soft tissue problems)
- ASR recalled 2010 = DePuy ASR hip resurfacing and XL Acetabular System
- “Pseudotumor does not mean malignancy - it is a sterile inflammatory mass
- “Small head MoM THAs have higher failure rates than resurfacing
- “Metal ions can remain elevated for years after revision
- “Revision for ALTR has poorer outcomes than revision for other causes
Cobalt greater than 7 ppb is the concerning threshold (MHRA guidelines). Levels greater than 10 ppb require urgent investigation. Chromium follows similar pattern but cobalt is more clinically relevant. Test whole blood, not serum. Annual monitoring mandatory for all MoM hips.
Inclination greater than 55 degrees causes edge loading with metal-on-metal contact outside the bearing surface. Combined anteversion matters - aim for inclination 40-45 degrees and anteversion 15-20 degrees. Malposition is the strongest predictor of failure.
Metal Artifact Reduction Sequence MRI allows soft tissue visualization around metal implants. Essential for detecting ALTR, pseudotumor, and muscle atrophy. Ultrasound is alternative but operator-dependent. CT less useful for soft tissue but shows osteolysis.
Pseudotumor = benign inflammatory mass, not malignancy. Caused by hypersensitivity reaction to metal debris (Type IV). Histology shows ALVAL (Aseptic Lymphocyte-dominated Vasculitis-Associated Lesion). Can cause extensive soft tissue destruction including abductor damage.
- Metal Ion Level
- Cobalt less than 4 ppb
- Imaging Findings
- No abnormality on imaging
- Management
- Annual surveillance with bloods
- Metal Ion Level
- Cobalt 4-7 ppb
- Imaging Findings
- Small fluid collection
- Management
- 6-monthly surveillance, optimize activity
- Metal Ion Level
- Cobalt 7-10 ppb
- Imaging Findings
- ALTR present on MARS MRI
- Management
- Consider revision, close monitoring
- Metal Ion Level
- Cobalt greater than 10 ppb
- Imaging Findings
- Large pseudotumor or tissue destruction
- Management
- Revision surgery recommended
SMALLRisk Factors for ALTR
Hook:SMALL things cause big problems - pay attention to these risk factors!
Overview and Epidemiology
Metal-on-metal (MoM) hip bearings were introduced as an alternative to metal-on-polyethylene to reduce wear-related osteolysis and improve longevity, particularly in younger active patients. However, concerns about adverse local tissue reactions (ALTR), elevated metal ion levels, and pseudotumor formation have led to a significant decline in their use and multiple product recalls.
The DePuy ASR Hip Resurfacing System and ASR XL Acetabular System were voluntarily recalled in August 2010 due to higher than expected revision rates. The Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) data showing 6.4% revision rate at 5 years was instrumental in identifying the problem.
- Peak usage: 2005-2010 before concerns emerged
- Current use: Near zero for primary THA, very limited resurfacing
- Affected population: Estimated 500,000+ patients with MoM hips worldwide
- ASR failure rate: 12-13% at 5 years (recalled devices)
- Well-positioned resurfacing: 95%+ survival at 10 years in experienced hands
- Pseudotumor incidence: 1-4% symptomatic, up to 60% asymptomatic on MRI
- Revision burden: Significant healthcare cost and patient morbidity
- Systemic toxicity: Rare but documented cardiac, neurological, thyroid effects
- Legal implications: Major class action settlements globally
- Ongoing surveillance: Lifetime monitoring required for all MoM patients
Pathophysiology and Mechanisms
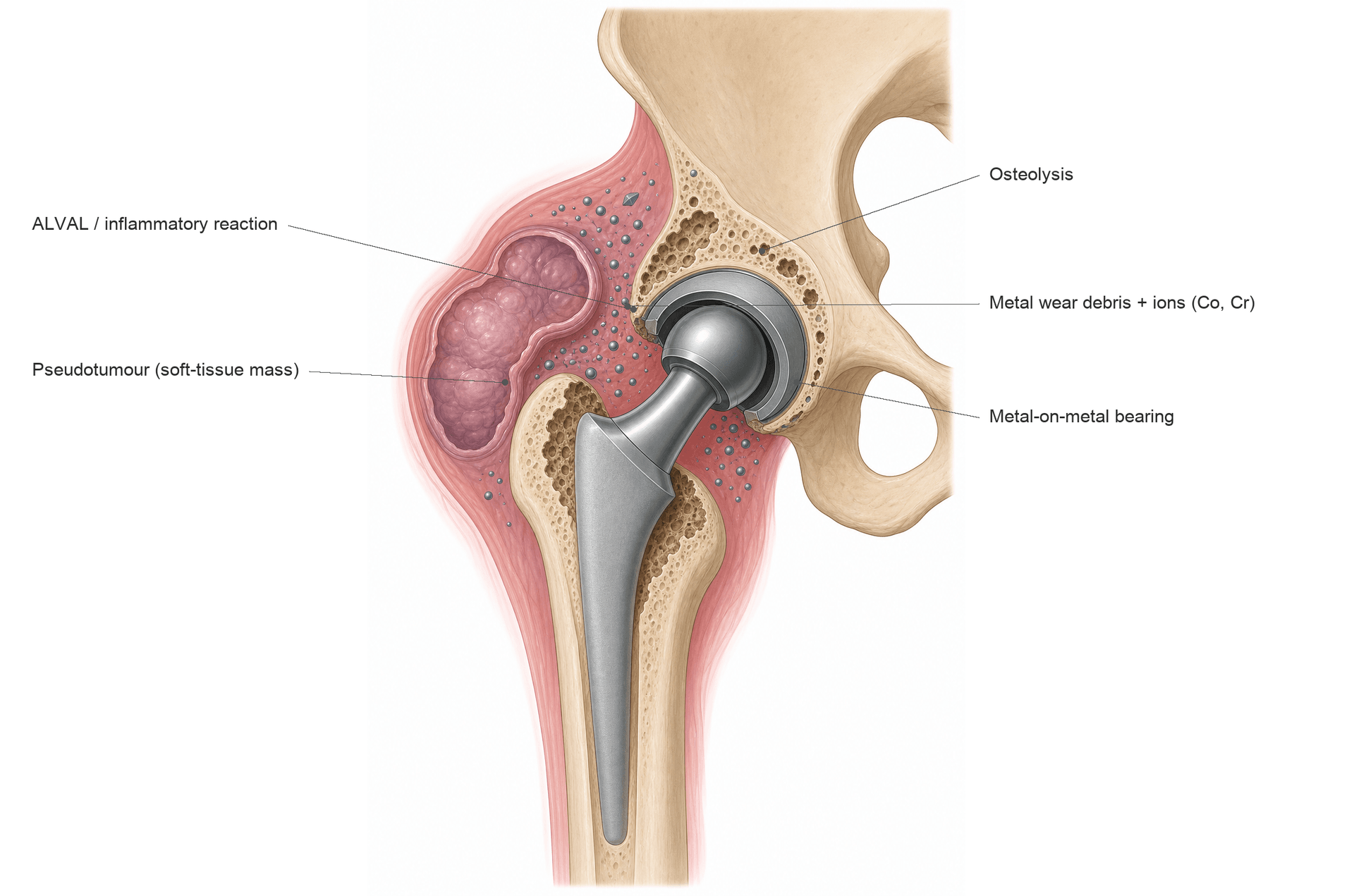
ALTR is caused by a combination of wear-generated metal debris and corrosion products from the bearing surface and modular junctions. This triggers a Type IV hypersensitivity reaction in susceptible individuals, leading to soft tissue destruction, osteolysis, and potentially systemic toxicity.
Tribological Failure
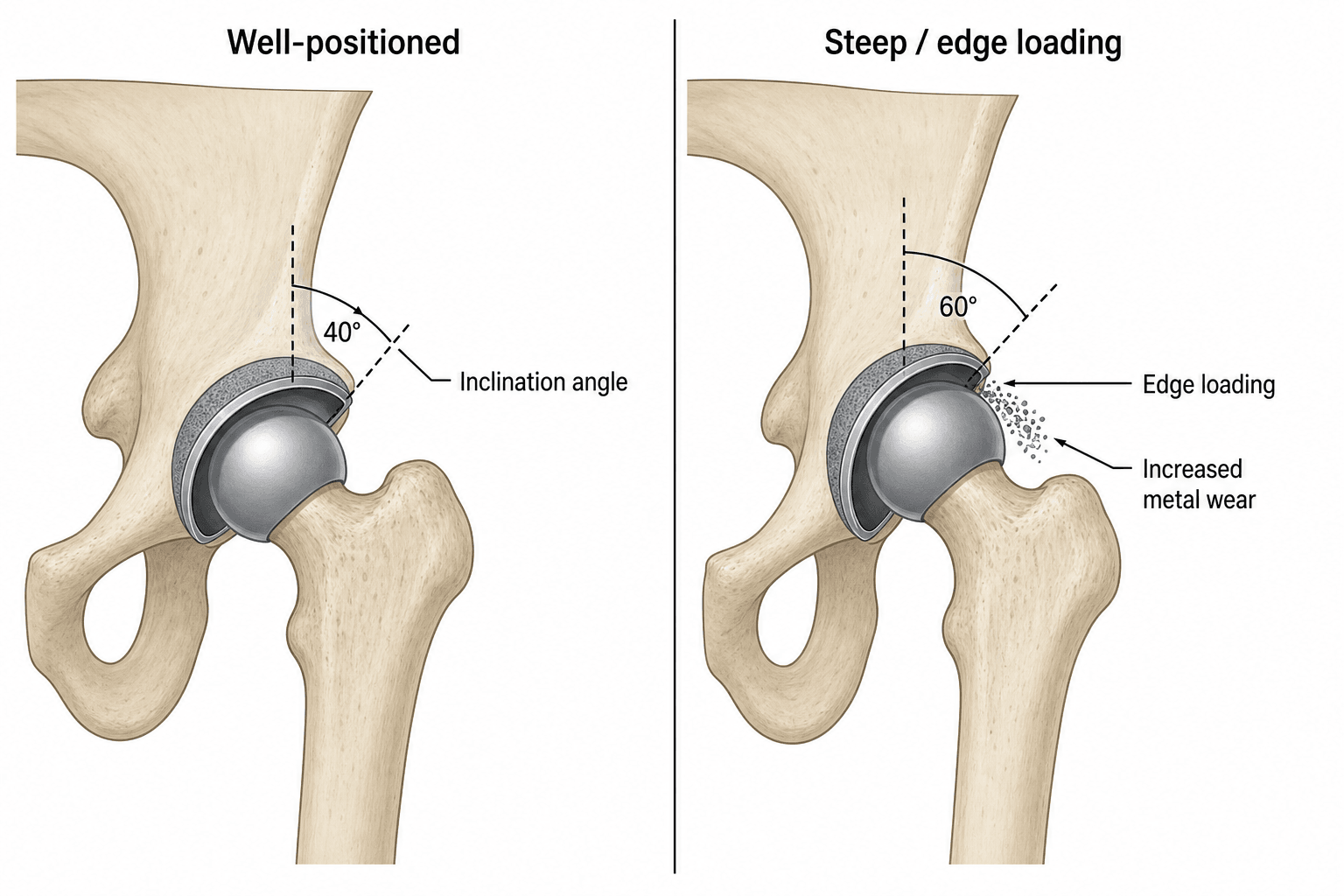
Metal-on-metal bearings rely on fluid film lubrication to separate the articulating surfaces. When this lubrication fails (due to edge loading, malposition, or high activity), metal-on-metal contact occurs, generating wear debris.
- Cause
- Cup inclination greater than 55 degrees or low coverage
- Result
- Contact at rim, not center
- Clinical Significance
- 10-100x increased wear rate
- Cause
- High range of motion, microseparation
- Result
- Linear wear pattern on head
- Clinical Significance
- Visible on explanted components
- Cause
- Modular junction corrosion
- Result
- Metal release from taper
- Clinical Significance
- More common with large heads, long necks
- Cause
- Well-positioned, matched components
- Result
- Minimal wear
- Clinical Significance
- Low ion levels, good outcomes
Biological Response
- ALVAL: Aseptic Lymphocyte-dominated Vasculitis-Associated Lesion
- Pseudotumor: Solid or cystic inflammatory mass
- Metallosis: Black staining from metal debris deposition
- Soft tissue necrosis: Destruction of capsule, abductors
- Osteolysis: Bone resorption around implants
- Neurological: Cognitive changes, peripheral neuropathy (rare)
- Cardiac: Cardiomyopathy reported at very high levels
- Thyroid: Hypothyroidism in some case reports
- Renal: Metal deposition, uncertain clinical significance
- Hematological: Cobalt affects erythropoiesis
ALVAL (Aseptic Lymphocyte-dominated Vasculitis-Associated Lesion) is the characteristic histological finding. It shows perivascular lymphocytic infiltrates, endothelial swelling, and tissue necrosis. This pattern distinguishes hypersensitivity from simple wear debris reaction and is associated with worse soft tissue destruction.
METALCauses of Metal-on-Metal Failure
Hook:METAL fails when the METAL bearing goes wrong - position, loading, and biological reaction!
Classification Systems
Hart MRI Classification of ALTR
Based on MARS MRI appearances of periprosthetic soft tissue abnormalities.
- Description
- Fluid only
- MRI Appearance
- Simple effusion, no wall thickening
- Management
- Surveillance, consider aspiration
- Description
- Fluid with synovitis
- MRI Appearance
- Wall thickening, enhancing synovium
- Management
- Close monitoring, consider revision
- Description
- Solid pseudotumor
- MRI Appearance
- Mass lesion, solid component
- Management
- Revision recommended
- Description
- Mixed/destructive
- MRI Appearance
- Complex tissue destruction, muscle atrophy
- Management
- Urgent revision, expect bone/muscle loss
Type 2b and Type 3 lesions have the worst outcomes after revision. Early detection and intervention before extensive tissue destruction improves revision outcomes significantly. Size of pseudotumor correlates with abductor damage.
Clinical Assessment
- Pain: Groin, lateral hip, thigh - often different from arthritic pain
- Swelling: Visible or palpable mass (large pseudotumor)
- Functional decline: Worse than expected after arthroplasty
- Implant details: Date of surgery, implant type (critical)
- Clicking or clunking: May indicate subluxation or impingement
- Neurological symptoms: Numbness, weakness (nerve compression)
- Gait: Trendelenburg sign (abductor damage)
- Mass: Palpable swelling anterolaterally
- ROM: May be preserved despite significant ALTR
- Leg length: Assess for subsidence or dislocation
- Neurological: Sciatic or femoral nerve involvement
- Skin changes: Rarely, sinus or discoloration
Up to 60% of patients with MoM hips may have asymptomatic ALTR on imaging. Symptoms do not correlate well with severity of soft tissue damage. This is why systematic surveillance with imaging is essential regardless of symptoms.
Differential Diagnosis
- Distinguishing Features
- Elevated metal ions, characteristic MRI findings
- Investigations
- Metal ions, MARS MRI
- Distinguishing Features
- Raised inflammatory markers, positive culture
- Investigations
- CRP, ESR, aspiration and culture
- Distinguishing Features
- Pain with activity, progressive radiolucencies
- Investigations
- Sequential X-rays, CT
- Distinguishing Features
- Anterior groin pain, pain with hip flexion
- Investigations
- Injection test, CT for cup position
- Distinguishing Features
- Lateral pain, point tenderness
- Investigations
- Clinical diagnosis, ultrasound
Investigations
Investigation Protocol for MoM Hip Surveillance
Whole blood cobalt and chromium - not serum (serum underestimates levels). Cobalt less than 7 ppb generally acceptable. Cobalt greater than 7 ppb requires further investigation. Cobalt greater than 10 ppb is high risk. Annual monitoring mandatory for all MoM hips.
AP pelvis and lateral hip - assess component position (inclination, anteversion), loosening signs, osteolysis. Cup inclination greater than 55 degrees is concerning for edge loading. Compare with previous films.
Metal Artifact Reduction Sequence MRI - gold standard for soft tissue assessment. Detects fluid collections, pseudotumors, muscle atrophy, osteolysis. Classification guides management. Should be performed if ions elevated or symptoms present.
Alternative to MRI when unavailable or contraindicated. Operator-dependent but can detect fluid and masses. Less sensitive for muscle atrophy and bone changes. Useful for guided aspiration.
Rule out infection before revision. Send for microbiology culture (extended incubation), cell count, and differential. Synovial fluid alpha-defensin if available. Essential in all painful MoM hips.
The topic repeatedly says "exclude infection," but the examinable nuance is why that is hard in a MoM hip: metallosis and ALTR mimic and confound the standard PJI tests, so the usual thresholds can mislead.
- Aspirate appearance: ALTR/metallosis produces a cloudy, grey or "metallic"/creamy aspirate that can look like pus.
- Synovial cell count: metal/corrosion particles are miscounted as leucocytes by automated analysers, giving a falsely elevated synovial white-cell count and neutrophil percentage - a manual count is needed, and a falsely high automated count must not be taken as proof of infection.
- Alpha-defensin: can be falsely positive in metallosis/ALTR, reducing its specificity in this setting.
- Serum CRP/ESR: ALTR itself can mildly raise inflammatory markers, so modest elevations are non-specific.
Practical consequence: a painful MoM hip can have biochemistry and an aspirate that look infected when the problem is ALTR - and, conversely, true infection can coexist. Use manual synovial cell counts, multiple culture samples with extended incubation, and the overall picture (ions, MARS MRI, implant) rather than a single automated count, and apply infection criteria (e.g. MSIS/EBJIS) with awareness of these MoM-specific false positives.
Exam point: in a painful MoM hip you must exclude infection, but metal debris falsely elevates the automated synovial cell count and alpha-defensin - request a manual cell count and interpret PJI tests cautiously, because ALTR and infection can look identical and can coexist.
CIMMSALTR Investigation Protocol
Hook:CIMMS investigation - Complete the picture before deciding on revision!
Metal Ion Interpretation
- Interpretation
- Normal/optimal
- Action Required
- Annual surveillance
- Interpretation
- Acceptable
- Action Required
- Annual surveillance
- Interpretation
- Borderline elevated
- Action Required
- Increased surveillance, consider imaging
- Interpretation
- Elevated - concerning
- Action Required
- MARS MRI required, 6-monthly review
- Interpretation
- High - significant risk
- Action Required
- Urgent imaging, consider revision
- Interpretation
- Very high - systemic risk
- Action Required
- Revision recommended, systemic assessment
- Whole blood, not serum - serum underestimates by 50%
- Cobalt more clinically relevant than chromium for ALTR
- Cobalt:chromium ratio - a disproportionately high cobalt (cobalt-dominant, high Co:Cr ratio) suggests taper/trunnion corrosion, whereas bearing-surface wear tends to raise both metals together
- Unilateral MoM - compare to population norms
- Bilateral MoM - interpret with caution, levels additive
A common refinement the topic otherwise glosses over is using the pattern of ion elevation to localise the source, and recognising that adverse reaction to metal debris (ARMD) is not confined to metal-on-metal bearings:
- Bearing-surface (articular) wear of a MoM bearing releases both cobalt and chromium, classically in a roughly balanced ratio (chromium is partly retained locally as chromium orthophosphate, but both rise in blood).
- Mechanically-assisted crevice corrosion at the head-neck taper (trunnionosis) preferentially releases cobalt, producing a markedly elevated cobalt with relatively normal chromium - a high cobalt:chromium ratio. So a cobalt-dominant pattern points to a taper/modular-junction problem rather than the bearing.
- ARMD/ALTR also occurs in metal-on-polyethylene THA with a cobalt-chrome head on a corroding taper (especially large-diameter heads and certain modular-neck stems) - an identical pseudotumour/ALVAL reaction driven by taper corrosion, not the bearing. A painful MoP THA with a rising isolated cobalt should prompt the same ARMD workup (ions, MARS MRI, infection exclusion).
Exam point: read the ions as a pattern - balanced Co/Cr rise = bearing wear; cobalt-dominant rise = taper corrosion/trunnionosis - and remember ARMD can occur in a non-MoM (MoP) hip through head-neck taper corrosion, so "it isn't a MoM bearing" does not exclude an adverse metal reaction.
Management Algorithm
Lifetime Surveillance for MoM Hips
All patients with MoM hip implants require lifelong surveillance regardless of symptoms.
Surveillance Schedule
Clinical assessment, metal ion levels (Co and Cr), plain radiographs if any concerns. Document symptoms, examination findings, implant function.
Many centers recommend baseline MARS MRI for all MoM patients to establish soft tissue status. Repeat if symptoms develop or ions rise.
6-monthly review if Cobalt greater than 7 ppb, new symptoms, or abnormal imaging. More frequent if rapidly rising ions or progressive symptoms.
Progressive ALTR on imaging, Cobalt greater than 10 ppb with symptoms, functional decline, neurological compromise, or component failure.
Metal ions can rise years after implantation. ALTR can develop in previously asymptomatic patients. There is no "safe" time to stop monitoring. Document surveillance in writing to patients.
Surgical Management
Key Surgical Principles for MoM Revision
- Review all imaging including MARS MRI
- Map pseudotumor location and extent
- Assess bone stock on CT if osteolysis suspected
- Rule out infection with aspiration
- Counsel patient regarding expected outcomes
- Extended approach - may need extensile exposure for pseudotumor excision
- Complete debridement - remove all necrotic tissue and metallosis
- Pseudotumor excision - thorough removal of reactive tissue
- Tissue sampling - multiple samples for microbiology and histology
- Bone grafting - address osteolytic defects
- Bearing change - ceramic-on-polyethylene preferred
- Stability assessment - anticipate instability from tissue loss
- Ceramic-on-polyethylene: Preferred for revision
- Ceramic-on-ceramic: Alternative but squeaking risk
- Avoid MoM: Never use MoM for revision
- Dual mobility: Consider if instability risk high
- Standard: If soft tissues preserved
- Dual mobility: Abductor weakness or tissue loss
- Constrained liner: Severe instability risk
- Assess intraoperatively: Trial stability before final
Complications
The complications of a MoM bearing arise from chronic metal-ion and particulate release. They are best grouped as local (the great majority), regional/mechanical, and systemic (rare).
- Pseudotumour / ALTR: cystic or solid inflammatory mass
- ALVAL: lymphocyte-dominated hypersensitivity reaction
- Metallosis: black staining of capsule and soft tissues
- Soft-tissue necrosis: destruction of capsule and abductors
- Fluid collections / recurrent effusions
- Osteolysis around the components
- Aseptic loosening of cup or stem
- Trunnionosis (taper corrosion) in stemmed MoM
- Femoral neck fracture / narrowing in resurfacing
- Instability / dislocation from abductor and capsule loss
- Nerve compression (sciatic or femoral) from a large pseudotumour
- Vascular compression by an expanding mass (rare)
- Trochanteric bursitis and gait disturbance (Trendelenburg)
- Cardiomyopathy (most serious, very high cobalt)
- Neuro-ocular toxicity: neuropathy, hearing and visual loss
- Hypothyroidism
- Polycythaemia (cobalt-driven erythropoiesis)
Local complications frequently progress without proportionate symptoms, and systemic effects appear late. This is the rationale for lifelong surveillance and a low threshold for cross-sectional imaging. Complications specific to revision surgery (instability, infection, persistent ions, nerve injury, re-revision) are detailed in the Surgical Management section.
Guidelines, Registries & Global Practice
Global Epidemiology:
An estimated one million MoM bearings were implanted worldwide during the peak period of roughly 2003 to 2010, the majority in younger, more active patients. Use has since collapsed to near zero for primary arthroplasty. Large national registries were decisive in exposing the problem before manufacturer surveillance, and remain the backbone of outcome data.
Registry Evidence (Side by Side):
- Region
- United Kingdom
- Key MoM Signal
- Resurfacing worse than THR in women at every head size; stemmed large-head MoM high revision rates
- Region
- Australia
- Key MoM Signal
- Early ASR signal (around 6 to 7% revision at 5 years) that contributed to the 2010 recall; small-head MoM THA worse than resurfacing
- Region
- United States
- Key MoM Signal
- Documents sharp decline in MoM use and ongoing revision burden from prior implants
- Region
- Sweden / Scandinavia
- Key MoM Signal
- Confirmed inferior survivorship of large-head MoM versus conventional bearings
Guidelines Compared (Side by Side):
- Surveillance Trigger for Imaging
- Symptoms or whole-blood cobalt/chromium above 7 ppb (about 119 nmol/L)
- Headline Position
- Annual review for all MoM hips; cross-sectional imaging and closer follow-up if symptomatic or ions raised; higher scrutiny for large-head stemmed MoM and ASR
- Surveillance Trigger for Imaging
- Symptoms or rising/elevated metal ions (no single mandated cut-off)
- Headline Position
- Routine ion testing not advised in asymptomatic, well-functioning patients; image and test symptomatic patients; individualised follow-up
- Surveillance Trigger for Imaging
- Symptoms, abnormal exam, rising ions, or suspicious imaging
- Headline Position
- Risk-stratified, symptom-led surveillance; metal ions and MARS MRI reserved for at-risk or symptomatic patients
- Surveillance Trigger for Imaging
- Symptoms or ions above the 7 ppb consensus threshold
- Headline Position
- Aligns broadly with MHRA; emphasises implant-specific risk and lifelong follow-up of high-risk designs
The UK/European approach is more proactive (population surveillance with a 7 ppb action level) whereas the US/AAOS approach is more symptom-led, reflecting differences in registry infrastructure and the absence of a universally agreed ion cut-off. All agree that symptomatic patients and high-risk designs (ASR, large-head stemmed MoM) need metal ions plus MARS MRI, and that monitoring is lifelong.
- DePuy ASR (recalled 2010): ASR Hip Resurfacing System and ASR XL Acetabular System
- DePuy Pinnacle MoM liner option: progressively withdrawn
- Multiple large-head stemmed MoM and other resurfacing systems voluntarily withdrawn worldwide
- Well-resourced settings: structured recall registries, routine whole-blood ICP-MS metal-ion assays, and ready MARS MRI access enable proactive surveillance and earlier revision.
- Limited-resource settings: ion assays and MARS MRI may be unavailable, so practice relies more on symptoms, plain radiographs, and ultrasound; patient tracing after recalls is harder. The principle remains identical - any symptomatic MoM hip warrants infection exclusion and cross-sectional imaging where obtainable, and lifelong follow-up.
Whatever the health system, document surveillance, counselling, and informed consent in writing, and give patients a written surveillance plan - MoM hips require lifelong monitoring with no defined endpoint.
Controversies and Areas of Uncertainty
MoM management remains an area of genuine debate. Examiners reward candidates who can articulate the uncertainty rather than quoting cut-offs as absolutes.
The 7 ppb cobalt/chromium action level is a pragmatic regulatory threshold, not a biological cliff. Up to half of patients revised for ALTR have ions below 7 ppb (Hart 2012), and many with high ions never develop tissue damage. Ion level is one input, never the sole determinant.
Whether ALTR is driven mainly by high-wear particulate toxicity or by a Type IV hypersensitivity (ALVAL) to a normal debris load remains unresolved. The two likely coexist on a spectrum, which is why low-wear, well-positioned implants can still fail in susceptible patients.
UK/European guidance favours scheduled ion surveillance; US/FDA guidance discourages routine testing in asymptomatic, well-functioning hips. There is no randomised evidence that any specific surveillance interval changes outcomes.
Many cystic ALTRs in asymptomatic patients are stable or regress over time (Goldstein 2016), so imaging an abnormality does not mandate revision. Distinguishing lesions that will progress from those that will not is still imperfect.
Not every pseudotumour needs revision, and not every elevated ion level needs surgery. Revision for ALTR carries worse outcomes than primary THA. The decision must integrate symptoms, ion trend, imaging type/size, abductor status, and implant design - never a single number.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old man presents with progressive groin and lateral hip pain 6 years after a metal-on-metal hip resurfacing. He was previously very active but has noticed increasing difficulty with walking. Examination shows Trendelenburg gait and limited internal rotation. Investigations show Cobalt 15 ppb and Chromium 12 ppb. Plain films show a well-fixed implant with cup inclination of 52 degrees. What is your diagnosis and management plan?”
“A 48-year-old woman with bilateral ASR hip resurfacings performed in 2008 attends for routine surveillance. She is asymptomatic with excellent function. Metal ions show Cobalt 5 ppb and Chromium 4 ppb. X-rays show cup inclination of 48 degrees on right and 58 degrees on left. How do you manage this patient?”
“A 65-year-old man with a MoM THA from 2009 presents with progressive hearing loss, visual disturbance, cognitive decline, and peripheral neuropathy. Cardiology has found a new cardiomyopathy. Metal ions show Cobalt 180 ppb. What is your diagnosis and emergency management?”
Metal Ion Thresholds
- Cobalt less than 2 ppb = optimal
- Cobalt 2-7 ppb = acceptable, annual surveillance
- Cobalt 7-10 ppb = concerning, MARS MRI
- Cobalt greater than 10 ppb = high risk, consider revision
- Cobalt greater than 20 ppb = systemic risk, revise
Cup Position Risk
- Inclination greater than 55 degrees = edge loading
- Optimal inclination 40-45 degrees
- Optimal anteversion 15-20 degrees
- Malposition strongest predictor of failure
ALTR Classification (Hart)
- Type 1: Fluid only - surveillance
- Type 2a: Synovitis - consider revision
- Type 2b: Solid pseudotumor - revise
- Type 3: Destructive - urgent revision
Investigation Protocol
- Whole blood (not serum) metal ions
- Plain X-rays for position/loosening
- MARS MRI for soft tissue
- Aspiration to rule out infection
- Annual surveillance lifelong
Revision Principles
- Early revision preserves soft tissue
- Complete pseudotumor excision
- Ceramic-on-polyethylene bearing
- Consider dual mobility for instability
- Never MoM for revision
Key Facts
- ASR recalled August 2010
- AOANJRR data key to identifying problem
- Pseudotumor = benign inflammatory mass
- ALVAL = histological pattern
- Small head MoM worse than resurfacing
Evidence Base and Key Studies
Original Description of MoM Pseudotumours
- Case series of 20 hips (17 patients, all women) with soft-tissue masses termed pseudotumours after MoM resurfacing
- Common histology: extensive necrosis and lymphocytic infiltration
- 13 of 20 hips required revision to conventional THA
- Estimated approximately 1% of MoM resurfacing patients develop a pseudotumour within 5 years
ASR Early Failure - Excess Wear and Component Position
- Series of 660 MoM resurfacings/large-bearing THRs; all 17 adverse-reaction revisions (3.4%) were ASR bearings
- Failed hips had significantly smaller components and higher acetabular anteversion
- Significantly higher whole-blood and joint chromium and cobalt levels than asymptomatic patients (all p less than 0.001)
- Explants showed greater surface wear; adverse reaction usually implies high component wear in well-positioned implants
Why MoM Hips Fail - Metal Ions and Cup Inclination (AAOS Exhibit)
- 55 patients revised for failed Birmingham Hip Resurfacing compared with well-functioning controls
- Revised hips had significantly higher cup inclination, smaller head diameter, and higher whole-blood cobalt and chromium (all p less than 0.01)
- Nearly 50% of revised patients had blood metal ions below the 7 ppb threshold and low wear
- Unexplained pain drove 69% of revisions, suggesting patient-specific (hypersensitivity) factors
MRI Classification of Pseudotumours
- MRI classification of periprosthetic masses: Type I thin-walled cyst, Type II thick-walled cyst, Type III predominantly solid
- 33 hips in 25 patients reviewed over 4 years
- Type III solid masses were significantly larger and more often located anterior to the hip
- Symptom severity and revision rates were lowest for Type I and highest for Type III
Evidence Base - Registry, Revision and Toxicity
Registry Failure Rates of MoM Resurfacing (NJR)
- 434,560 primary THRs in the NJR for England and Wales (31,932 resurfacings)
- In women, resurfacing had worse implant survival than conventional THR at every head size
- Predicted 5-year revision in a 55-year-old woman: 8.3% (42mm resurfacing) vs 1.5% (28mm cemented MoP THR)
- Resurfacing matched other options only in men with large femoral heads
Re-revision After ALTR Revision (NJR)
- 2,535 MoM hips revised for adverse reaction to metal debris (ARMD) in the NJR, 2008-2014
- Re-revision in 7.6% of hips; cumulative 5-year implant survival 89.5%
- Predictors of re-revision: high BMI, modular-only revision, ceramic-on-ceramic bearing, and acetabular bone grafting
- Short-term re-revision risk comparable to all-cause non-MoM revision
Systemic Cobalt Toxicity From Metal Hip Prostheses
- Systematic review identifying 18 individual cases of systemic toxicity from metal hip implants
- Reported features: neuro-ocular toxicity (14 cases), cardiotoxicity (11), thyroid toxicity (9)
- Greatest risk was a cobalt-containing revision of a failed ceramic bearing (median blood cobalt 506 ug/L), not primary MoM failure (median 34.5 ug/L)
- Removal of the prosthesis usually lowered cobalt and improved some features, but not always fully
Natural History of Asymptomatic ALTR
- 83 asymptomatic modular MoM THA patients had metal ions and MARS MRI; cystic ALTR found in 26 (31%)
- On repeat MRI a year later, 15 of 19 lesions (79%) decreased in size
- 3 patients became symptomatic and were revised
- All patients had cobalt and chromium below the 7 ppb threshold