Piriformis Anatomy
Anatomical Variations.
- In up to 15-20% of cases, the Sciatic nerve (or Common Peroneal division) passes THROUGH or ABOVE the muscle.
- Risk: Blind dissection or retractor placement can injure the aberrant nerve.
- Mitigation: Identify the nerve early, especially if anatomy looks "abnormal".
Retraction Hazard.
- The artery exits the notch just superior to the Piriformis.
- Risk: Vigorous retraction or blind placement of a 'Charnley' retractor pin into the ilium can lacerate the vessel.
- Consequence: Massive hemorrhage within the pelvis (the artery retracts into the pelvis).
- Nerves
- Superior Gluteal
- Vessels
- Superior Gluteal
- Other
- -
- Nerves
- Sciatic, Inf Gluteal, Pudendal, Post Cutaneous Thigh, N to OI/QF
- Vessels
- Inferior Gluteal, Internal Pudendal
- Other
- Pudendal N goes to Alcock's canal
P-GO-GO-QLateral Rotators
Hook:The order of the short external rotators from Superior to Inferior.
POPS IQInfra-piriform Contents
Hook:Everything that comes out BELOW the Piriformis.
Overview
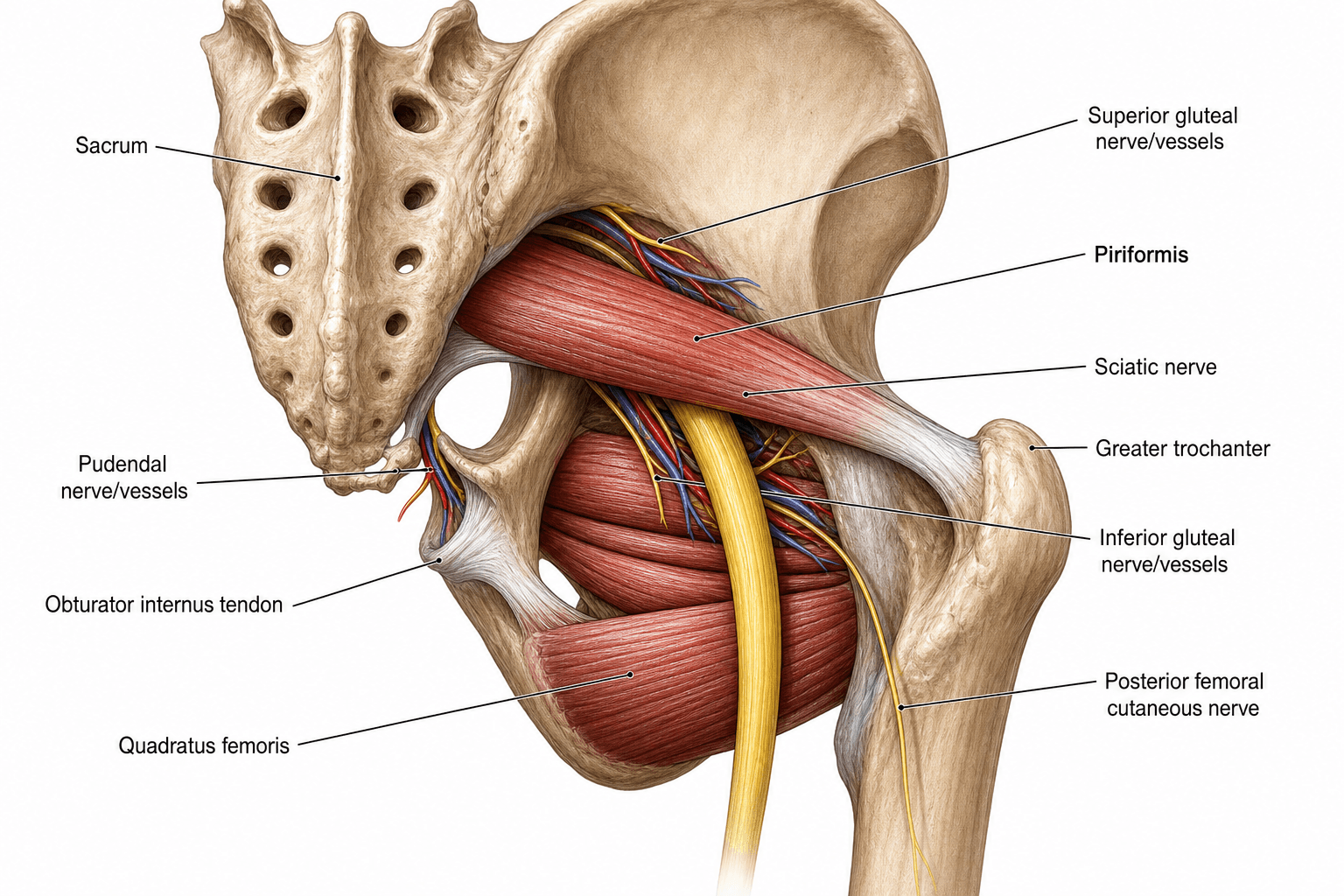
The Piriformis is a flat, pyramidal muscle located in the posterior gluteal region. It is the crucial anatomical landmark that organizes the neurovascular structures exiting the pelvis. Almost all significant structures leave the pelvis via the Greater Sciatic Foramen, related either superiorly or inferiorly to this muscle.
Neurovascular
Origin
- Anterior Sacrum: From the front of the sacrum, involving segments S2, S3, and S4 (between the anterior sacral foramina).
- Gluteal Surface of Ilium: Near the PIIS (Posterior Inferior Iliac Spine).
- Sacrotuberous Ligament: A minor origin contribution.
Course
- Leaves the pelvis through the Greater Sciatic Foramen.
- Fills the foramen almost completely, leaving small gaps above and below.
Insertion
- Greater Trochanter: Specifically the superior border and medial aspect of the apex.
- The tendon often blends with the tendons of the Obturator Internus and Gemelli.
Surface Anatomy
Piriformis Line
- Draw a line from the PSIS (Posterior Superior Iliac Spine) to the Greater Trochanter.
- The superior border of the Piriformis roughly corresponds to this line.
Palpation
- Palpation: Deep palpation in the mid-buttock, midway between the PSIS and Greater Trochanter, may elicit tenderness in Piriformis syndrome.
- Difficulty: Direct palpation is difficult due to the overlying Gluteus Maximus.
- Seated Palpation: Palpating while the patient is seated (flexed hip) may make the muscle more accessible as it emerges from under the gluteus maximus.
Tenderness at the greater sciatic notch is a sensitive sign for deep gluteal pathology.
Beyond the syndrome, the piriformis fossa is a classic landmark for antegrade femoral nailing, and examiners probe both the entry choice and a naming catch:
- The two antegrade start points are the piriformis fossa (the depression just medial to the tip of the greater trochanter, collinear with the femoral canal/shaft axis — suited to a straight nail) and the greater-trochanter tip (suited to a trochanteric-entry nail with a proximal bend).
- A piriformis-fossa start point that is too medial or too posterior endangers the medial femoral circumflex artery and the femoral-head blood supply — a recognised cause of avascular necrosis, which is why piriformis-entry antegrade nailing is avoided in children and adolescents (a trochanteric or more lateral entry is preferred to protect the still-vulnerable supply). The start point also lies close to the abductors and the superior gluteal nerve.
- Nomenclature trap: the piriformis tendon actually inserts on the greater trochanter, so the "piriformis fossa" entry (the trochanteric/digital fossa medial to the tip) is a slight misnomer — a favourite exam catch.
Pathology: Piriformis Syndrome
Etiology
- Primary: Anatomic anomaly (Beaton Type B). (less than 15%)
- Secondary: Macro-trauma (fall on buttock), Micro-trauma (wallet neuritis, overuse), or Hypertrophy.
- Mechanism: Compression of the Sciatic nerve (Usually the peroneal division) by the muscle belly or tendon.
The peroneal division is more lateral and susceptible to compression against the ischium.
S1-S2Piriformis Roots
Hook:Piriformis is primarily S1/S2.
Classification Systems
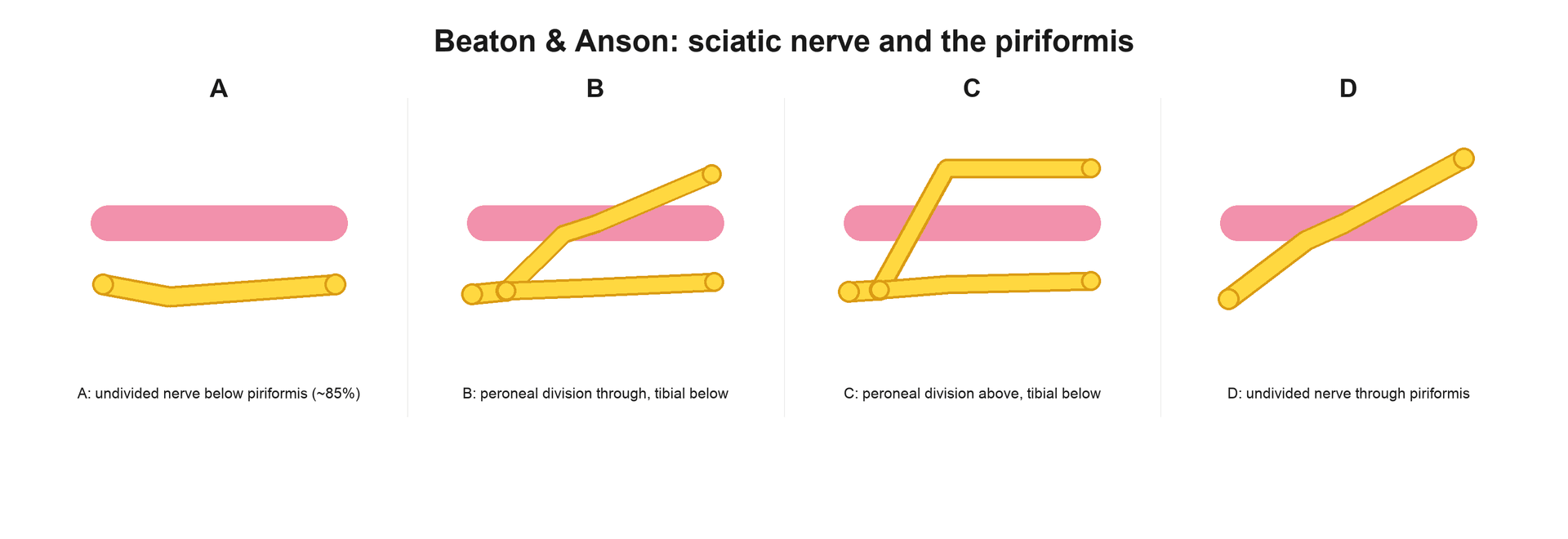
Beaton & Anson: Sciatic Nerve Relationship
Describes the relationship between the Piriformis and the Sciatic Nerve (SN).
- Type A (Unsplit): Normal (85-90%). SN passes undivided below Piriformis.
- Type B (Split): Common Peroneal Nerve (CPN) pierces Piriformis; Tibial Nerve (TN) passes below.
- Type C (Split): CPN passes ABOVE (superior); TN passes below.
- Type D (Unsplit): Entire SN pierces muscle (Rare).
- Type E (Split): CPN passes ABOVE; TN pierces muscle (Very Rare).
- Type F (Unsplit): Entire SN passes ABOVE muscle (Extremely Rare).
Significance: Type B is the most common variant and predisposes to entrapment (Piriformis Syndrome).
Clinical Assessment
Provocative Tests.
- FAIR Test: Flexion, Adduction, Internal Rotation. Stretches the Piriformis and compresses the Sciatic Nerve. Pain = Positive.
- Pace's Sign: Pain and weakness on resisted abduction and external rotation of the thigh in a sitting position.
- Freiberg's Sign: Pain on passive internal rotation of the extended hip.
Differential Diagnosis.
- Piriformis Syndrome is a subset of Deep Gluteal Syndrome (DGS).
- Other causes: Gemelli-Obturator Internus syndrome, Ischiofemoral impingement, Proximal Hamstring tendinopathy.
- Differentiation: Point of maximal tenderness and exact provocation maneuvers help distinguish.
Differential Diagnosis of Deep Buttock / Extra-spinal Sciatica
- Distinguishing feature
- Buttock pain, sitting intolerance, notch tenderness; foot usually spared
- Key test / finding
- FAIR test; relief after image-guided block
- Distinguishing feature
- Dermatomal pain often to foot; back pain; positive neural tension
- Key test / finding
- Positive SLR; MRI lumbar spine; EMG paraspinal changes
- Distinguishing feature
- Pain in the ischiofemoral space; long-stride pain
- Key test / finding
- Narrowed ischiofemoral and quadratus femoris space on MRI; quadratus femoris oedema
- Distinguishing feature
- Ischial tuberosity pain on sitting and loading
- Key test / finding
- Tenderness at ischium; MRI tendinopathy or avulsion
- Distinguishing feature
- Deep gluteal pain; part of deep gluteal syndrome spectrum
- Key test / finding
- Tenderness more inferolateral; endoscopic findings
- Distinguishing feature
- Pain over the SIJ, rarely below knee
- Key test / finding
- Cluster of provocation tests; diagnostic SIJ block
Investigations
MRI Neurography
- Gold Standard.
- Can show Piriformis hypertrophy, asymmetry, or anomalous course of the nerve.
- T2 Sequence: Increased signal in the sciatic nerve indicates neuritis.
Diagnostic Injection
- CT or Ultrasound-guided local anesthetic into the muscle belly.
- Positive Test: Immediate relief of sciatic symptoms confirms the diagnosis.
This is often considered the most definitive confirmation of the diagnosis.


Surgical Technique
Piriformis Release
- Indication: Failure of conservative management and positive diagnostic block.
- Approach: Posterior (Kocher-Langenbeck) or Endoscopic.
- Technique:
- Identify Sciatic Nerve distally.
- Trace proximally to inferior border of Piriformis.
- Identify any bands or split nerve (Type B).
- Tenotomize the Piriformis at the reflected tendon (insertion).
- Observe decompression of the nerve.
- Caution: Protect the Superior Gluteal vessels superiorly!
Endoscopic release is becoming increasingly common due to lower morbidity.
A point the posterior approach makes critical: the deep branch of the medial femoral circumflex artery (MFCA) is the dominant blood supply to the adult femoral head (it continues as the lateral epiphyseal/retinacular vessels). Its constant relationship to the short external rotators is examinable:
- The deep branch runs along the inferior border of obturator internus and the gemelli, then crosses deep (anterior) to the obturator externus tendon before piercing the capsule near the superior border of the gemelli.
- Releasing the piriformis and the conjoint tendon (obturator internus plus gemelli) is safe, but the obturator externus tendon must be preserved — it shields the MFCA, which is why the Ganz surgical hip dislocation is built around keeping obturator externus intact.
- The danger zone is aggressive dissection at the quadratus femoris / lesser-trochanter region (and dividing obturator externus), which can injure the MFCA and cause avascular necrosis of the femoral head.
Complications
- Sciatic Nerve Injury: Direct trauma or traction.
- Bleeding: Inferior Gluteal vessels are often adherent to the deep surface.
- Incomplete Release: Failure to identify anomalous bands.
- Instability: Following total hip replacement, failure of repair increases posterior dislocation risk.
Rehabilitation Protocol
- Release: Immediate weight bearing. Avoid deep flexion/stretch for 2 weeks.
- Stretching: Gentle neural gliding exercises starts at week 2.
- Strengthening: Gluteus Maximus and Medius strengthening to correct pelvic mechanics.
Prognosis
- Conservative: Variable. Stretching works for mild cases.
- Injection: Good short term relief. Predicts surgical success.
- Surgery: 80-90% success in properly selected patients (Positive block).
Clinical Relevance
Treatment by Stage
- Treatment
- Rest, NSAIDs, Stretching
- Evidence
- First line. 70% success.
- Treatment
- Physiotherapy (gluteal strengthening)
- Evidence
- Address biomechanics.
- Treatment
- Injection (Steroid/Botox)
- Evidence
- Diagnostic and Therapeutic.
- Treatment
- Surgical Release
- Evidence
- Last resort.
- Botox: Paralyses the muscle, inducing atrophy and relieving compression. Effects last 3-6 months.
Surgical release should only be considered after a failure of at least 6 months of conservative therapy.
Guidelines, Registries & Global Practice
Global epidemiology. Piriformis syndrome is cited as a cause in roughly 5-6% of patients presenting with sciatica, though this figure is contested because the diagnosis lacks an accepted reference standard. A piriformis-sciatic nerve anatomical anomaly is present in about 17% of cadavers worldwide (Smoll meta-analysis) but is not over-represented in symptomatic patients. Female predominance is reported in most series, often quoted around 2:1 to 6:1.
Society Positions on Diagnosis and Management
- Diagnostic stance
- Diagnosis of exclusion; image-guided diagnostic block central
- Management emphasis
- Conservative first; ultrasound-guided injection; endoscopic release in refractory deep gluteal syndrome
- Diagnostic stance
- Sciatica pathway prioritises excluding lumbar disc/stenosis; piriformis labelled when spine is normal
- Management emphasis
- Physiotherapy and activity advice first-line; injection and surgery reserved for failures
- Diagnostic stance
- Subset of deep gluteal syndrome; favours MR neurography where available
- Management emphasis
- Stepwise: physiotherapy, image-guided injection (steroid or botulinum toxin), then endoscopic decompression
- Diagnostic stance
- Piriformis is the key landmark in the Kocher-Langenbeck and posterior hip approaches
- Management emphasis
- Identify and protect sciatic nerve at the inferior border; repair short external rotators to lower posterior dislocation risk
Registry and Outcome Notes
- Arthroplasty registries (NJR-UK, AJRR-USA, AOANJRR-Australia, SHAR-Sweden): do not track piriformis pathology directly, but record nerve-injury and dislocation outcomes relevant to the posterior approach where the piriformis is released and repaired. Sciatic/peroneal palsy after primary THA is consistently rare (around 0.1-1%).
- Posterior approach: remains the most common worldwide workhorse exposure; soft-tissue (capsule and short external rotator) repair is associated with reduced posterior dislocation in registry and cohort data.
High- vs Limited-Resource Practice Variation
- High-resource settings: MR neurography, ultrasound-guided injection, and endoscopic deep gluteal decompression are available; diagnosis is refined with dynamic imaging.
- Limited-resource settings: diagnosis is clinical (symptom quartet plus provocative tests); landmark or fluoroscopic injection and open release predominate, with greater reliance on physiotherapy and activity modification.
Controversies & Areas of Uncertainty
Some authors argue piriformis syndrome is over-diagnosed and that most "extra-spinal sciatica" is better captured by the broader term deep gluteal syndrome. The anatomical anomaly is not more common in symptomatic patients (Smoll), undermining a purely structural explanation.
There is no accepted reference standard. FAIR, Pace and Freiberg signs have limited and poorly quantified accuracy. Response to an image-guided diagnostic block is the most relied-upon confirmation but is not formally validated.
MR neurography can show piriformis asymmetry, sciatic nerve hyperintensity and anomalous course, but findings overlap with asymptomatic individuals, so imaging supports rather than establishes the diagnosis.
Randomised data (Fishman) favour botulinum toxin A over steroid, but trials are small and heterogeneous; optimal dose, target (belly vs tendon) and guidance modality remain debated.
MCQ Practice Points
Q: Which structure exits the Greater Sciatic Foramen SUPERIOR to the Piriformis? A: Superior Gluteal Nerve and Vessels. Everything else is inferior.
Q: What is the action of the Piriformis when the hip is flexed to 90 degrees? A: Abduction. In extension, it is an External Rotator.
Q: The Nerve to Piriformis is derived from which segments? A: S1 and S2. (Anterior rami).
Q: In the Beaton Type B anomaly, which component of the sciatic nerve pierces the muscle? A: Common Peroneal Nerve. The Tibial nerve passes inferiorly.
Q: Where does the Piriformis originate? A: Anterior surface of the Sacrum.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“You are performing a posterior approach for a THR. You see the short external rotators. How do you identify the Piriformis?”
“45F with 6 months of buttock and posterior leg pain. MRI Lumbar Spine is normal. What is your differential?”
“During a sciatic nerve exploration, you find the Common Peroneal Nerve passing THROUGH the piriformis. What type of anomaly is this?”
Anatomy
- Origin: Anterior Sacrum
- Insert: Superior GT
- Nerve: N to Piriformis (S1-2)
- Passes: Greater Sciatic Foramen
Relationships
- Superior: Sup Gluteal N/A
- Inferior: Sciatic N, Inf Gluteal
- Anterior: Sacral Plexus
- Posterior: Gluteus Maximus
Clinical
- Action: ER (Ext), Abd (Flex)
- Test: FAIR Test
- Syndrome: Sciatica + Normal MRI
- Variant: CPN pierces (Type B)
Evidence Base
Every citation below has been checked against its source record in PubMed. The key conceptual point comes from Smoll's meta-analysis — the piriformis-sciatic anomaly is common (~17%) but NOT more frequent in symptomatic patients, so the anomaly alone does not explain the syndrome. The remaining studies anchor diagnosis (Hopayian's four features), injection accuracy (Finnoff — ultrasound far better than fluoroscopy), treatment (Fishman botulinum toxin; Kay deep-gluteal decompression), and the THA nerve-palsy risk that makes the piriformis landmark surgically important (Farrell).
Botulinum Toxin A and Physical Therapy
- Double-blind placebo-controlled trial using electrophysiologic (FAIR-test H-reflex) selection
- Botulinum toxin A gave more pain relief than lidocaine-plus-steroid (P less than 0.05) and than placebo (P = 0.001) on the visual analog scale
- H-reflex prolongation over 1.86 msec (3 SD) in the FAIR position was a clinical indicator of piriformis syndrome
Piriformis and Sciatic Nerve Variation Meta-analysis
- Systematic review and meta-analysis pooling 18 studies and 6,062 cadavers
- Pooled prevalence of a piriformis-sciatic nerve anomaly was 16.9% (95% CI 16.0-17.9%)
- Anomaly prevalence in piriformis-syndrome surgical series (16.2%) did not differ significantly from cadavers (P = 0.824)
Surgical Management of Deep Gluteal Syndrome
- Systematic review of 28 studies (481 patients) on surgery for sciatic nerve entrapment in deep gluteal syndrome
- Commonest causes: iatrogenic (30%), piriformis syndrome (26%), trauma (15%), non-piriformis muscle pathology (14%)
- Improvement in pain at final follow-up reported in all 28 studies; endoscopic procedures had major complications in 0% and minor in fewer than 1%