The Largest Nerve in the Body
- Strictly speaking, it is two nerves (Tibial + Common Peroneal) wrapped in one sheath
- Exits pelvis below the Piriformis muscle (in 85% of people)
- Supplies all hamstring muscles and all muscles below the knee
- Common Peroneal division is lateral and more vulnerable to stretch injury
- Injection Safe Zone: Upper Outer Quadrant of the buttock
- “The component to the Short Head of Biceps is the first branch of the Common Peroneal division
- “Sensory supply is entire foot/leg EXCEPT medial calf (Saphenous - Femoral)
- “Foot Drop is the classic sign of high Sciatic injury (Peroneal fibers are lateral)
- “Surgical approach: Posterior approach to hip puts it at risk (External Rotators protect it)
Foot Drop is not always at the knee.
- A high Sciatic lesion often presents as an isolated Foot Drop because the Common Peroneal fibers are lateral and superficial.
- Differentiate: Check Hamstrings (Short Head Biceps) and Gluteals. If Glutes affected → Plexus/Root.
Upper Outer Quadrant.
- Any other quadrant risks the Sciatic (Lower Medial/Lateral) or Superior Gluteal (Upper Inner/Middle).
- In thin patients, the nerve is surprisingly superficial.
- Component
- Tibial
- Action
- Knee Flex / Hip Ext
- Innervation
- L5, S1, S2
- Component
- Tibial
- Action
- Knee Flex / Hip Ext
- Innervation
- L5, S1, S2
- Component
- Tibial
- Action
- Knee Flex / Hip Ext
- Innervation
- S1, S2, S3
- Component
- Com Peroneal
- Action
- Knee Flexion
- Innervation
- L5, S1, S2
- Component
- Tibial
- Action
- Hip Extension
- Innervation
- L4, L5, S1
P-I-N- P-I-N-SGreater Sciatic Foramen Contents
Hook:PIN the PINS in the Foramen.
P-G-O-G-QDeep Rotators (Relations)
Hook:Sciatic nerve lies ON these muscles (The Bed).
HAM-LEGSciatic Supply
Hook:Sciatic supplies the HAM and the LEG (mostly).
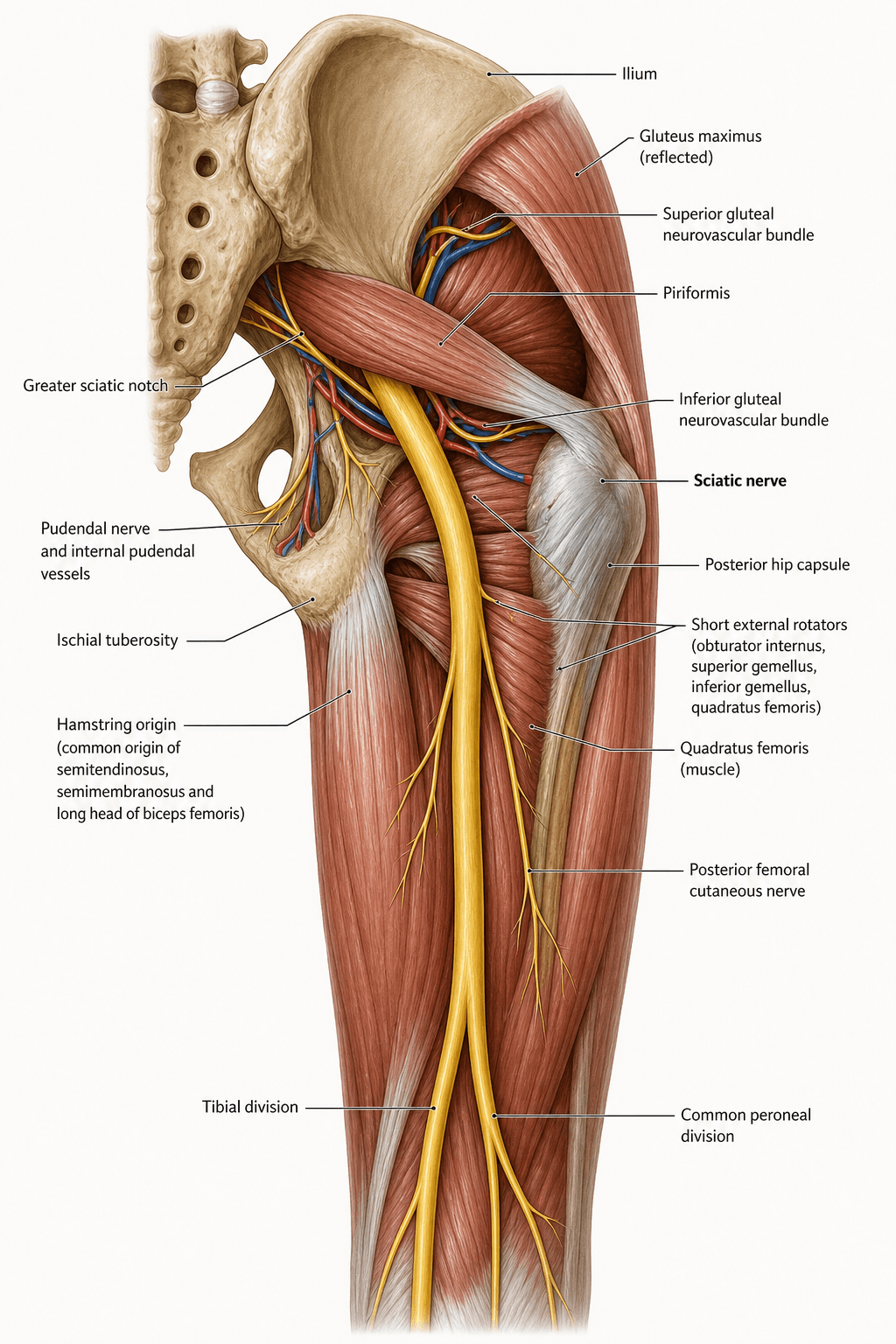
Overview
The Sciatic Nerve is the largest nerve in the body (roughly the width of an adult thumb, around 2 cm at its origin), derived from the ventral rami of L4-S3 via the sacral plexus. It serves as the primary conduit for motor and sensory signals to the lower limb.
Functionally it is best understood as two nerves in one sheath: a medial tibial division (ventral rami) and a lateral common peroneal (fibular) division (dorsal rami). These two components are bound by a common epineurium but remain anatomically and clinically distinct from origin to the popliteal fossa, where they formally separate. This duality explains nearly every examination point on the topic: the peroneal division, being lateral, smaller, with fewer/larger fascicles, less protective connective tissue and tethered at the fibular neck, is selectively vulnerable to stretch, compression and ischaemia, so a "sciatic" injury often masquerades as an isolated foot drop.
Its relations in the gluteal region (resting on the bed of short external rotators, exiting beneath piriformis in most people) are critical for the posterior approach to the hip, acetabular fracture surgery and intramuscular injection safety. Its long course and the great distance from a proximal lesion to the foot muscles also dominate prognosis after laceration.
Neurovascular
Pelvic & Gluteal Course
- Origin: Sacral Plexus (Anterior surface of Piriformis).
- Exit: Leaves pelvis via Greater Sciatic Foramen, usually inferior to the Piriformis muscle.
- Gluteal Region: Descends deep to Gluteus Maximus, resting on the "Bed" of deep external rotators (Gemelli, Obturator Internus, Quadratus Femoris).
- Thigh: Enters posterior thigh deep to the Long Head of Biceps.
- Termination: Divides into Tibial and Common Peroneal nerves at the apex of the Popliteal Fossa (variable).
Structure
- The two components (Tibial and Common Peroneal) are physically separate within the epineurium from the origin.
- Medial: Tibial (Ventral divisions L4-S3).
The sciatic nerve is the terminal continuation of the sacral plexus, which lies on the anterior surface of piriformis on the pelvic side wall:
- Lumbosacral trunk: the descending L4 and L5 ventral rami unite to form the lumbosacral trunk, which crosses the pelvic brim to join the S1-S3 (and part of S4) ventral rami and build the plexus — so the sciatic carries L4-S3.
- Anterior (ventral) vs posterior (dorsal) divisions: within the plexus the ventral divisions coalesce into the tibial component and the dorsal divisions into the common peroneal component — bound in one sheath but already separate, the anatomical basis of the two-nerves-in-one rule.
- Plexus neighbours (which explain combined deficits in a plexopathy): the superior gluteal nerve (L4-S1) above piriformis, the inferior gluteal nerve (L5-S2) below it, the pudendal nerve (S2-S4) and the posterior cutaneous nerve of the thigh (S1-S3).
- Clinical corollary: because the glutei are supplied by the gluteal nerves before the sciatic forms, gluteal weakness localises the lesion to the plexus or roots, not the sciatic nerve — the single most useful localising rule.
Surface Anatomy
Gluteal Region
- PSIS: Posterior Superior Iliac Spine.
- Ischial Tuberosity: Medial landmark (nerve is lateral).
- Greater Trochanter: Lateral landmark (nerve is medial).
The Sciatic Nerve emerges at the midpoint of a line connecting the Ischial Tuberosity to the Greater Trochanter.
Classification Systems
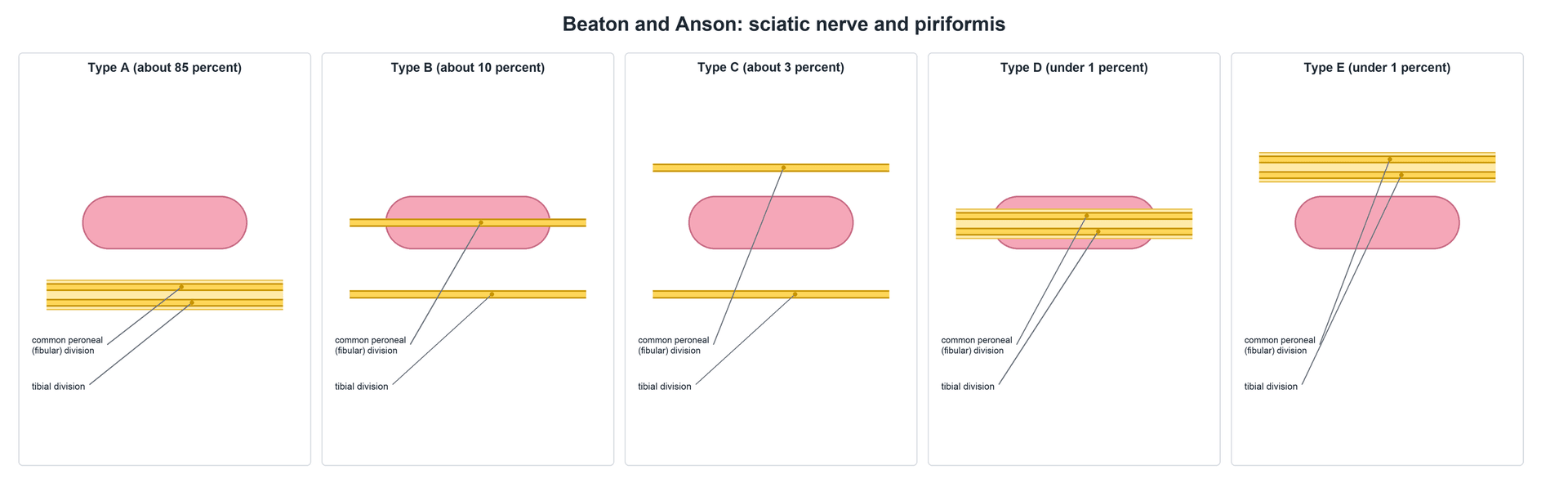
Beaton & Anson Classification
This classification describes the relationship between the Sciatic Nerve and the Piriformis muscle.
- Type A (85%): Undivided nerve passes below Piriformis.
- Type B (10%): Common Peroneal division passes through Piriformis; Tibial passes below.
- Type C (3%): Common Peroneal passes above Piriformis; Tibial below.
- Type D (less than 1%): Entire nerve passes through Piriformis.
- Type E (less than 1%): Entire nerve passes above Piriformis.
- Type F (less than 1%): Undivided nerve passes below, but there is an accessory piriformis.
Type B is the most clinically significant variant as it predisposes to Piriformis Syndrome (compression of the Common Peroneal division).
Clinical Assessment
Lasègue's Sign.
- Passive elevation of leg with knee extended.
- Positive: Radicular pain (L5/S1) below knee at 30-70 degrees.
- Bragard's: Dorsiflexion increases pain.
- Sensitizing: Internal rotation stretches the nerve.
- Ankle Jerk (S1): Lost in Tibial/Sciatic lesions.
- Knee Jerk (L3/4): Preserved (Femoral nerve).
- Hamstring Reflex: Often diminished.
Differentiating High vs Low Lesion
- High Sciatic
- Weak/Paralyzed
- Common Peroneal (Knee)
- Normal
- High Sciatic
- Normal (Plexus intact)
- Common Peroneal (Knee)
- Normal
- High Sciatic
- Weak
- Common Peroneal (Knee)
- Weak
- High Sciatic
- Weak
- Common Peroneal (Knee)
- Normal
To confirm radicular origin:
- Flex the knee to relieve pain (Bowstring relaxed).
- Apply firm pressure in the popliteal fossa over the nerve.
- Positive: Pain returns (Confirming nerve tension/irritation).
Differential Diagnosis of "Sciatica" / Foot Drop
The clinical syndrome of buttock-to-leg pain or foot drop has several causes that must be separated, because management differs completely. The single most useful discriminators are the short head of biceps femoris (peroneal-division marker), the glutei (plexus/root marker) and the paraspinals (root marker).
- Distinguishing Feature
- Paraspinals involved; SLR positive; dermatomal
- Key Test
- MRI lumbar spine; H-reflex / EMG
- Distinguishing Feature
- Glutei AND sciatic muscles weak
- Key Test
- EMG (paraspinals spared); pelvic MRI
- Distinguishing Feature
- Glutei spared; short head biceps weak
- Key Test
- EMG; MR neurography
- Distinguishing Feature
- Short head biceps & hamstrings normal
- Key Test
- EMG localises block at fibular head
- Distinguishing Feature
- Deep buttock pain; normal spine MRI
- Key Test
- FAIR test; diagnostic block; MR neurography
- Distinguishing Feature
- Knee extension weak; ankle jerk preserved
- Key Test
- EMG; quadriceps wasting pattern
Investigations
MRI
- MRI Lumbar Spine: Mandatory to rule out radiculopathy (disc herniation/stenosis) which is the most common cause of "Sciatica".
- MRI Pelvis: To assess the course of the nerve through the sciatic notch. Look for:
- Mass lesions (Hematoma, Tumor).
- Piriformis hypertrophy or asymmetry.
- Signal change (T2 hyperintensity) within the nerve indicative of neuritis or compression.
MR Neurography
- Specialized fluid-sensitive sequences to track the nerve fascicles.
- Highly sensitive for extraspinal sciatica.
This modality is particularly useful for identifying non-compressive etiologies like neuritis.


Surgical Technique
Posterior Exposure (Thigh)
- Incision: Midline posterior thigh.
- Deep Flexia: Split Gluteus Maximus proximally.
- Identification: Find nerve deep to Long Head of Biceps (guides you to it).
- Neurolysis: Release adhesions from hamstring origin or quadratus femoris.
Always identify the nerve in normal tissue (distally or proximally) before dissecting the scarred zone.
The stretch-injury, positioning and THA-lengthening points throughout this topic all reduce to the strain tolerance of peripheral nerve:
- A nerve tolerates only modest elongation: intraneural blood flow falls and conduction is impaired at around 6 to 8 percent strain, with structural (fascicular) failure at roughly 15 percent. Beyond the ischaemic threshold, sustained tension causes a stretch/traction palsy even without laceration.
- Why position helps: keeping the hip extended and the knee flexed slackens the sciatic nerve across both joints — the protective position during reduction and retraction.
- THA lengthening: restoring length loads the nerve; a commonly quoted ceiling is about 4 cm, but it is nerve tension, not an absolute number, that matters — palsy occurs at lower lengthening in dysplasia, where the nerve is already short and scarred.
- Why the peroneal division fails first: it is laterally placed, has fewer and larger fascicles with less cushioning epineurium, and is tethered at the sciatic notch and the fibular neck, so a given limb elongation concentrates more strain on it — hence the foot-drop-predominant picture.
Complications
- Foot Drop: Most common manifestation of injury. Requires AFO (Ankle Foot Orthosis).
- Neuropathic Pain: Often severe (Type II CRPS).
- Pressure Sores: Insensate foot/heel.
- Contracture: Equinus deformity if not splinted.
Rehabilitation Protocol
- Splinting: Anti-drop foot splint (AFO) immediately.
- ROM: Passive ankle dorsiflexion to prevent contracture.
- Strengthening: Hamstrings and Glutes.
- Nerve Glides: Sciatic sliders flossing techniques.
- Return to Sport: Dependent on motor recovery (Variable).
Prognosis
- Stretch Injury: Good prognosis (neuropraxia).
- Injection Injury: Poor prognosis (chemical neurolysis).
- Laceration: Guarded. Rate of regeneration is 1mm/day, but the distance to the foot is distinctively long (causes motor endplate death before nerve arrives).
- Common Peroneal: Paradoxically worse prognosis than Tibial division (less vascular, more tethered).
Clinical Relevance
Sciatica and Palsy
- Management
- NSAIDS, Physio, Time
- Indication for Surgery
- Cauda Equina / Motor Deficit
- Management
- Reduction, splint in ext
- Indication for Surgery
- Nerve entrapment in joint
- Management
- Stretch, Injection
- Indication for Surgery
- Failure of conservative
- Management
- Observe, EMG
- Indication for Surgery
- Pain/No recovery over 3m
- Reduction: In hip dislocation, prompt reduction is the primary treatment for the nerve (ischemia).
- Neurolysis: Indicated for tethering or persistent compression (e.g., scarring after trauma).
Neurolysis should be performed with magnification to avoid disrupting the epineural blood supply.
Injection Injury Protocol
- Immediate: Stop injection. Document drug and volume.
- Acute Phase: Analgesia (Neuropathic agents). MRI to look for hematoma (compressive).
- Chronic Phase: Serial EMG. If no recovery at 3-6 months, consider exploration and neurolysis (poor prognosis if intrafascicular injection occurred).
Guidelines, Registries & Global Practice
Global Epidemiology
- Traumatic hip dislocation: Sciatic nerve injury complicates roughly 10% of adult posterior hip dislocations/fracture-dislocations and about 5% of paediatric cases worldwide, the peroneal division being most often affected (Cornwall & Radomisli, 2000).
- Total hip arthroplasty (THA): Pooled prevalence of nerve palsy is approximately 1%, rising to 3-5% in revision and developmental dysplasia of the hip (DDH) (Schmalzried 1991, 1997).
- Injection injury: Iatrogenic sciatic neuritis from dorsogluteal intramuscular injection remains a global problem, disproportionately affecting children and limited-resource/rural settings where ventrogluteal technique is under-used.
- Anatomical variant: A piriformis–sciatic anatomical anomaly is present in approximately 17% of the population (Smoll, 2010).
Side-by-Side Society Guidance
- Domain
- Hip / acetabular surgery
- Key Recommendation
- Protect nerve via short-rotator cuff; hip extended + knee flexed; retractors on bone
- Domain
- THA / DDH
- Key Recommendation
- Identify lengthening and palsy risk; avoid overlengthening; document pre-op neurology
- Domain
- Open fractures / trauma
- Key Recommendation
- Document distal neurovascular status before and after every reduction
- Domain
- IM injection
- Key Recommendation
- Prefer ventrogluteal over dorsogluteal site to avoid the nerve
Registry Evidence
- Arthroplasty registries (NJR England & Wales, AJRR USA, AOANJRR Australia, Swedish SHAR) do not record nerve palsy as a primary endpoint, but capture the DDH and revision case-mix that drives higher palsy rates, and track leg-length restoration, the principal modifiable risk factor.
- Registry-level rises in revision and complex primary volume translate into a higher absolute burden of nerve injury even when the per-case rate is stable.
High- vs Limited-Resource Practice Variation
- High-resource: MR neurography, intra-operative neuromonitoring, and early EMG are available; ventrogluteal injection and ultrasound-guided blocks are standard.
- Limited-resource: Diagnosis rests on clinical examination; dorsogluteal injection persists and is a leading preventable cause of paediatric foot drop. Prevention (correct injection site, prompt reduction of dislocations) carries the greatest yield where reconstructive nerve surgery is scarce.
Controversies & Areas of Uncertainty
- Does piriformis syndrome exist as a distinct entity? The variant anatomy is no commoner in symptomatic patients (Smoll 2010), and many authorities prefer the broader term deep gluteal syndrome. It remains a diagnosis of exclusion with no universally accepted diagnostic criterion.
- Timing and role of exploration after injection injury. There is no high-level evidence that early surgical washout or neurolysis changes outcome; most chemical injuries are established at the moment of injection. Management is therefore largely supportive, with exploration reserved for a compressive haematoma or non-recovery on serial EMG.
- Acute exploration after THA palsy. Whether to re-operate for an immediate post-operative palsy is debated; most are observed unless imaging shows a correctable compressive cause (haematoma) or gross overlengthening. Return of any motor function within two weeks predicts good recovery (Schmalzried 1997).
- Maximum "safe" lengthening in THA. A figure of around 4 cm is widely quoted, but the threshold is patient-specific; nerve tension, not an absolute number, is the determinant, and palsy occurs at lower lengthening in dysplasia.
- Tendon transfer vs orthotic for established foot drop. Choice between a permanent AFO and reconstructive transfer (e.g. tibialis posterior) depends on prognosis for spontaneous recovery, which is itself uncertain for high lesions.
MCQ Practice Points
Q: Where is the safe zone for intragluteal injection? A: Upper Outer Quadrant. This avoids the Sciatic Nerve (Lower Medial/Lateral) and Superior Gluteal Nerve (Upper Medial).
Q: Why is the Common Peroneal division more susceptible to injury? A: It is lateral, more superficial, and has fewer fascicles with less connective tissue. It is also tethered at the fibular head, reducing its ability to glide during stretch.
Q: Which hamstring muscle is NOT supplied by the Tibial division? A: Short Head of Biceps Femoris. It is supplied by the Common Peroneal division. This is a key differentiator for high vs low lesions.
Q: What is the innervation of the 'Hamstring portion' of Adductor Magnus? A: Tibial Division of Sciatic Nerve. The adductor portion is supplied by the Obturator Nerve.
Q: What are the root values of the Sciatic Nerve? A: L4, L5, S1, S2, S3. It is the largest branch of the sacral plexus.
Q: Which sensory branch of the sciatic system is the standard nerve autograft donor, and what is the donor deficit? A: The sural nerve (tibial division + peroneal communicating branch). It yields ≈30-40 cm of graft with only a small, well-tolerated patch of lateral foot/heel numbness — the workhorse for bridging peripheral nerve gaps.
Q: The sciatic nerve supplies the skin of the posterior thigh — true or false? A: False. The sciatic gives no cutaneous branch in the thigh; posterior thigh skin is the posterior cutaneous nerve of the thigh (S1-S3), a separate sacral-plexus branch.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“You perform a posterior approach THR. In recovery, the patient has a foot drop. Take me through your management.”
“A nurse calls you. A patient complained of immediate burning pain down the leg during an IM injection. What do you do?”
“A cyclist complains of deep buttock pain and sciatica. MRI spine is normal. How do you assess for Piriformis Syndrome?”
Anatomy
- Roots: L4-S3
- Exit: Greater Sciatic Foramen
- Relation: Inf to Piriformis
- Divisions: Tibial (Med), CP (Lat)
Clinical
- Sign: SLR (Lasègue)
- Motor: Hamstrings + All below knee
- Reflex: Ankle (S1), Hamstring
- Safe Zone: Upper Outer Quadrant
Pathology
- Hip Dislocation: 10% Palsy
- THR: Traction/Retractor injury
- Injection: Chemical neuritis
- Piriformis: Compression
Evidence Base
Nerve Injury in Traumatic Hip Dislocation
- Sciatic nerve injury complicates approximately 10% of adult hip dislocations and 5% in children
- The peroneal branch is the division most often involved
- At least partial recovery occurs in 60-70% of patients
- No clear correlation between recovery and injury type or treatment chosen
MR Neurography & Surgery for Piriformis Syndrome
- 239 consecutive patients with sciatica refractory to standard treatment
- Piriformis syndrome was the rediagnosis in 67.8% once MR neurography was applied
- Piriformis asymmetry plus sciatic hyperintensity at the notch: 93% specificity, 64% sensitivity
- Piriformis surgery gave excellent or good outcome in over 80% of selected cases
Piriformis–Sciatic Variation: Meta-Analysis
- Meta-analysis of 18 studies pooling 6,062 cadavers
- Anomalous piriformis–sciatic relationship present in 16.9% (95% CI 16.0-17.9%)
- Prevalence in piriformis-syndrome surgical series (16.2%) was not significantly different from the general population
- Suggests the anatomical variant is not the dominant driver of piriformis syndrome
Beaton & Anson Variants in 294 Limbs
- 147 cadavers (294 limbs) dissected and classified by Beaton & Anson
- Typical pattern (undivided nerve below piriformis) in 93.6% of limbs
- Common peroneal through a doubled piriformis with tibial below in 4.1% (Beaton type B)
- All other variants (type C, D, E) each occurred in only 0.3% of limbs
Nerve Palsy After THA: Risk Factors & Prognosis
- 53 of 3,126 hip replacements (1.7% overall, 1.3% of primaries) developed neuropathy
- Prevalence rose to 5.2% in dysplasia/congenital dislocation and 3.2% in revisions (both significant risk factors)
- The sciatic nerve was involved in all but five extremities
- Cause was unclear in 57%; prognosis tracked the degree of nerve damage and all full recoveries occurred by 21 months
Update on Nerve Palsy After THA (Prognosis)
- Overall prevalence of nerve palsy after THA approximately 1%
- Sciatic nerve (usually the peroneal division) involved in nearly 80% of cases
- Complete/near-complete recovery in approximately 41%, mild residual deficit in 44%, poor outcome in approximately 15%
- Some motor function within 2 weeks predicts good recovery; female sex, dysplasia and revision increase risk
AO Foundation / Surgical Exposure Principles
- In the posterior (Kocher–Langenbeck / Moore) approach the short external rotators are mobilised to protect the sciatic nerve
- Keep the hip extended and the knee flexed during reduction to minimise nerve tension
- Retractors must be seated on bone (acetabular rim), never blindly in the posterior soft tissues
- The nerve should be identified and palpated when posterior fixation or release is planned