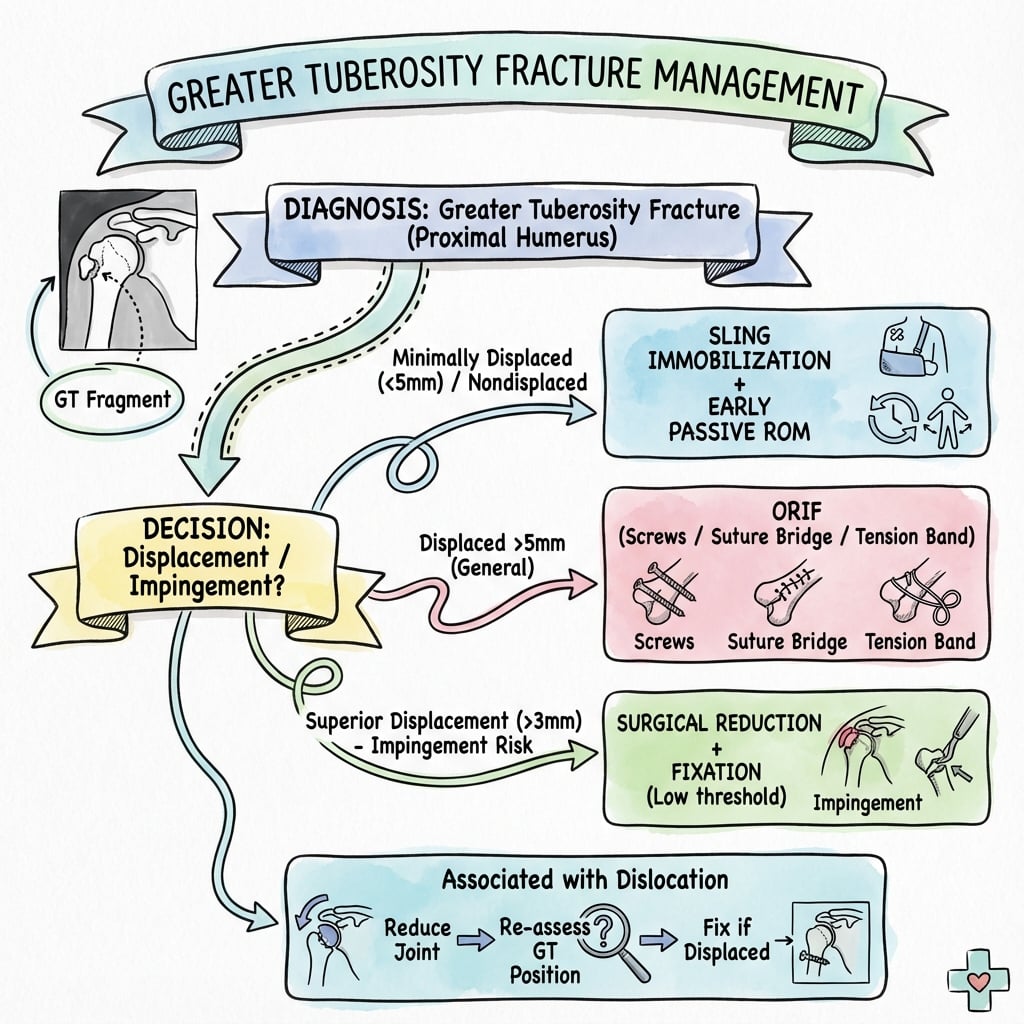
Rotator Cuff Attachment Site | Displacement Threshold 5mm | Posterior Displacement Worst
- Three cuff attachments: Supraspinatus (superior), Infraspinatus (middle), Teres minor (inferior)
- 5mm displacement is surgical threshold (3mm for overhead athletes)
- Posterior displacement worst - limits external rotation function
- Axillary view essential - shows posterior displacement (crescent sign)
- Deltoid split must stay within 5cm of acromion to protect axillary nerve
- “GT fracture with dislocation often reduces after glenohumeral reduction
- “Superior malunion causes impingement, posterior causes rotation loss
- “Screw fixation for good bone, suture anchors for osteoporotic bone
- “External rotation strength testing is key clinical assessment
5mm displacement is the standard surgical threshold. Use 3mm threshold for overhead athletes and laborers requiring full shoulder function. Posterior displacement is more functionally significant.
Three tendons attach to GT: Supraspinatus (superior facet), Infraspinatus (middle facet), Teres minor (inferior facet). The subscapularis attaches to lesser tuberosity.
Deltoid split approach must stay within 5cm of acromion. The axillary nerve courses 5-7cm distal to the lateral acromion. Document nerve function before and after any manipulation.
15-30% of anterior dislocations have associated GT fracture. Often reduces with glenohumeral reduction. Repeat imaging (especially axillary view) after reduction.
- Displacement
- Under 5mm
- Patient Factors
- Any patient
- Treatment
- Non-operative (sling, early ROM)
- Displacement
- 3-5mm
- Patient Factors
- Overhead athlete/laborer
- Treatment
- Consider surgical fixation
- Displacement
- Over 5mm
- Patient Factors
- Active patient
- Treatment
- Surgical fixation (screw/anchor)
- Displacement
- Variable
- Patient Factors
- Any patient
- Treatment
- Reduce first, reassess displacement
- Displacement
- Any
- Patient Factors
- Active patient
- Treatment
- Strong surgical indication
SITSRotator Cuff Attachments to GT
Hook:SITS muscles but only first three attach to Greater Tuberosity - subscapularis sits on lesser!
TUBERGT Fracture Assessment
Hook:The TUBER(osity) tells you what tendons attach and what displacement direction matters most!
Overview
Greater tuberosity fractures represent a clinically important subset of proximal humerus fractures due to their intimate relationship with rotator cuff function. The greater tuberosity serves as the attachment point for three of the four rotator cuff tendons - supraspinatus, infraspinatus, and teres minor.
- 15-20% of all proximal humerus fractures
- Bimodal distribution: young males (high energy), elderly females (low energy)
- 15-30% associated with anterior shoulder dislocations
- Higher rate in contact sports and falls
- Osteoporosis (elderly)
- Contact sports participation
- Seizure disorders
- Alcohol intoxication
- Fall onto lateral shoulder
- Direct blow to shoulder
- Forceful abduction with external rotation
- Avulsion by rotator cuff during dislocation
- Hyperabduction injury
- Anterior shoulder dislocation (15-30%)
- Rotator cuff tears
- Hill-Sachs lesion
- Bankart lesion
Anatomy and Pathophysiology
Anatomical Considerations
The greater tuberosity is a critical anatomic landmark that determines rotator cuff function and shoulder biomechanics.
- Superior facet: Supraspinatus insertion
- Middle facet: Infraspinatus insertion
- Inferior facet: Teres minor insertion
- Located lateral to the articular surface
- Forms the lateral margin of the bicipital groove
- Lesser tuberosity: Medial, subscapularis insertion
- Bicipital groove: Between tuberosities
- Anatomical neck: Between tuberosities and head
- Surgical neck: Below tuberosities
- Anterior humeral circumflex artery (ascending branch)
- Posterior humeral circumflex artery
- Rotator cuff tendon vessels
The greater tuberosity anatomy is crucial for understanding displacement patterns.
The "crescent sign" on axillary radiograph shows the displaced greater tuberosity fragment posterior to the humeral head, indicating significant displacement that typically requires surgical intervention.
Classification
Classification
- Fragment displaced less than 5mm
- Often associated with undisplaced surgical neck fracture
- Treated non-operatively in most patients
- Fragment displaced more than 5mm or angulated over 45°
- Significant functional deficit expected if not reduced
- Surgical indication in active patients
- Greater tuberosity fracture with anterior shoulder dislocation
- Fragment often reduces with glenohumeral reduction
- Re-evaluate displacement after reduction
Neer classification remains primary for clinical decision-making.
- Displacement
- Under 5mm
- Key Features
- Minimal displacement, stable
- Treatment
- Non-operative
- Displacement
- Over 5mm
- Key Features
- Significant displacement
- Treatment
- Surgical fixation
- Displacement
- Variable
- Key Features
- Associated dislocation
- Treatment
- Reduce first, reassess
- Displacement
- Variable
- Key Features
- Small cortical fragment
- Treatment
- Suture anchor fixation
- Displacement
- Variable
- Key Features
- Larger fragment
- Treatment
- Screw or plate fixation
Clinical Assessment
History and Physical Examination
History
- Fall onto outstretched hand or shoulder
- Direct blow to lateral shoulder
- Dislocation event (ask about reduction)
- Seizure activity
- Motor vehicle accident
- Shoulder pain (lateral predominant)
- Inability to lift arm
- Weakness with external rotation
- History of dislocation
- Numbness over deltoid (axillary nerve)
- Severe weakness (complete cuff avulsion)
- Vascular compromise
Thorough mechanism history helps predict associated injuries.
Physical Examination
- Swelling over lateral shoulder
- Ecchymosis (may extend to arm)
- Arm held in adduction and internal rotation
- Loss of normal shoulder contour
- Point tenderness over greater tuberosity
- Crepitus with gentle rotation
- Assess for associated injuries
- Active abduction limited and painful
- External rotation weak and painful
- Passive ROM may be preserved
- External rotation lag sign (indicates cuff avulsion)
- Hornblower's sign (teres minor function)
- Resisted external rotation strength
External rotation strength testing is critical and must be compared to contralateral side.
Neurovascular Assessment
- Most commonly injured nerve
- Test deltoid motor function
- Test sensation over "regimental badge" area
- Document before and after any manipulation
- Complete motor examination
- Sensory examination of upper limb
- May be injured with high-energy mechanism
- Axillary artery at risk with dislocation
- Check distal pulses
- Assess capillary refill
- Consider angiography if concern
Document complete neurovascular examination before any reduction attempts.
ALWAYS document axillary nerve function before and after shoulder reduction. The nerve courses around the surgical neck and is vulnerable during both injury and reduction maneuvers.
- Key Discriminator
- Point tenderness over GT, weak/painful external rotation, fragment on axillary view
- Investigation
- AP, scapular-Y and axillary radiographs; CT for surgical planning
- Key Discriminator
- Weakness without bony fragment; positive lag signs with normal bone
- Investigation
- Ultrasound or MRI - no cortical break
- Key Discriminator
- Squared-off shoulder, empty glenoid, arm held in slight abduction/external rotation
- Investigation
- AP and axillary radiographs showing humeral head out of joint
- Key Discriminator
- Diffuse proximal arm swelling, deformity below the tuberosities
- Investigation
- Radiographs showing fracture line distal to the tuberosities
- Key Discriminator
- Tenderness and step at the AC joint, not over the GT
- Investigation
- AP and zanca views of the AC joint
- Key Discriminator
- Atraumatic or trivial trauma, no fracture line, calcific deposit
- Investigation
- Radiograph shows calcific deposit, no cortical disruption
Investigations
Imaging Studies
- Perpendicular to scapular plane
- Shows glenohumeral joint space
- Identifies fracture and displacement
- Lateral scapula projection
- Confirms reduction status
- Shows anterior/posterior displacement
- Shows posterior displacement ("crescent sign")
- Identifies Hill-Sachs lesion
- Confirms glenohumeral reduction
- Most important view for displacement assessment
- Alternative if cannot abduct arm
- Patient leans back over cassette
- Useful in emergency setting
The axillary view is most important for assessing GT displacement.
The "crescent sign" on axillary radiograph indicates posterior displacement of the greater tuberosity fragment. This finding often indicates need for surgical intervention.



Management Algorithm
Treatment Decision Making
- Displacement under 5mm (or under 3mm in athletes)
- Elderly, low-demand patients with larger displacement
- Significant medical comorbidities
- Minimally displaced fracture-dislocation after reduction
Protocol
- Sling immobilization
- Ice, analgesia
- Gentle pendulum exercises
- Progressive passive ROM
- Active-assisted exercises
- Avoid active abduction
- Active ROM when healed
- Strengthening exercises
- Rotator cuff rehabilitation
- Full activities as tolerated
- Sport-specific training
- Return to work/sport based on function
Non-operative treatment yields excellent results in minimally displaced fractures.
The classic error in non-operative GT management is to immobilise and forget. The fracture fragment carries the rotator cuff insertion (supraspinatus superiorly, infraspinatus/teres minor posteriorly), and that deforming muscle pull can drag an initially acceptable fragment into a surgical position over the first weeks - a fracture under the operative threshold on day 1 can cross it by week 2-3.
So non-operative management is active surveillance, not neglect:
- Obtain interval radiographs (a true AP and an axillary view) at around 1-2 weeks and again at 6 weeks specifically to detect secondary displacement before the fragment malunites.
- Protect against the deforming pull in the early phase - sling, and avoid active abduction/external rotation until early union (the same logic as protecting a rotator cuff repair).
- If the fragment displaces past the threshold on a follow-up film, convert to fixation while reduction is still achievable; a late-displaced GT that malunites needs the much harder osteotomy/decompression salvage.
Exam point: a non-operatively-treated GT fracture needs early interval radiographs (incl. axillary) to catch secondary displacement from cuff pull, plus early activity restriction - do not assume an acceptable injury film means an acceptable healed position.
- Under 5mm: Non-operative
- Over 5mm: Surgical fixation
- Under 3mm: Non-operative
- Over 3mm: Consider surgery
- May accept greater displacement
- Consider comorbidities
- Functional goals important
- Repeat imaging (AP, axillary essential)
- Measure persistent displacement
- Fragment often reduces with head
- Non-operative treatment
- Early motion important
- Watch for instability
- Apply standard criteria
- Surgical fixation likely needed
- Consider associated instability repair
The familiar "operate over 5 mm" is a useful headline but an over-simplification examiners like to probe:
- Direction matters more than the absolute number: a few millimetres of superior displacement sits the tuberosity under the acromion (impingement, lost abduction), and posterior displacement blocks external rotation - so the functional consequence, not just the millimetres, drives the decision. A small superior/posterior displacement in an active or overhead patient can be more significant than a larger displacement tolerated in a low-demand elderly patient.
- Measurement is unreliable: displacement is easily under- or over-estimated on a single view; assess on a true AP plus an axillary (and CT when in doubt), accounting for the cuff's deforming pull.
- The threshold is trending down: because even modest superior displacement causes impingement, many authors now use a lower threshold (around 3 mm) for active patients and reserve the more lenient 5 mm tolerance for the elderly/low-demand.
Exam point: don't quote "5 mm" as a fixed law - say the threshold is direction-weighted and demand-dependent, measured on AP + axillary (+/- CT), with a lower (~3 mm) threshold in active/overhead patients and more tolerance in the elderly.
Surgical Technique
Operative Approaches
- Isolated greater tuberosity fracture
- Most common approach used
- Beach chair or lateral decubitus position
- Incision from anterolateral acromion edge
- Split deltoid in line with fibers
- Stay within 5cm of acromion (axillary nerve)
- Identify fracture fragment and cuff
- Direct access to fragment
- Minimizes soft tissue stripping
- Can extend if needed
- Axillary nerve injury (stay proximal)
- Deltoid origin damage
Deltoid-splitting provides excellent access while protecting axillary nerve.
The axillary nerve emerges approximately 5-7cm distal to the lateral edge of the acromion. The deltoid-splitting approach must stay within 5cm of the acromion to avoid nerve injury.
Fixation Techniques
- Reduce fragment anatomically
- Provisional K-wire fixation
- Cannulated screw over wire
- Washer if poor bone quality
- Typically 2 screws for rotation control
- Aim screws toward medial calcar
- Lag technique if bone allows
- Avoid proud screw head (impingement)
- Bury head below cortical surface
Two screws provide rotational stability and prevent toggle.
FIX GTSurgical Decision Making
Hook:FIX the GT when it meets surgical criteria!
Complications
Potential Complications
Most common complication of non-operative treatment with displacement
- Superior malunion: Subacromial impingement
- Posterior malunion: External rotation block
- Combined: Both impingement and rotation loss
- Pain with overhead activities
- Weakness of external rotation
- Catching and clicking
- Night pain
- Osteotomy and repositioning
- Arthroscopic subacromial decompression (mild cases)
- May require reverse shoulder arthroplasty in severe cases
Malunion is the primary reason to treat displaced fractures surgically.
Malunion of greater tuberosity fractures with superior displacement causes painful subacromial impingement that may require osteotomy to correct. This reinforces the importance of achieving anatomic reduction in displaced fractures.
Postoperative Care
Rehabilitation Protocol
- Protect fixation
- Control pain and swelling
- Maintain passive ROM
- Sling immobilization
- Pendulum exercises only
- Ice and analgesia
- Elbow/wrist/hand motion
- Passive forward flexion
- Passive external rotation (to neutral)
- No active abduction
- No active external rotation
- No lifting
- Sleep in sling or recliner
- Avoid reaching behind back
Protection phase focuses on healing while maintaining passive mobility.
Outcomes
Expected Results
- Union rate over 95%
- Good to excellent outcomes: 85-90%
- Return to pre-injury function: 80-85%
- Mean Constant score: 85-90
- Mean ASES score: 85-90
- Return to sport: 85%
- Pain resolution: 6-8 weeks
- ROM recovery: 8-12 weeks
- Strength recovery: 12-16 weeks
- Full activity: 3-4 months
Non-operative treatment yields excellent results in appropriately selected patients.
Guidelines, Registries & Global Practice
Global Epidemiology
Greater tuberosity fractures are best understood within the wider epidemiology of proximal humeral fractures, which are among the most common osteoporotic fractures worldwide. According to PubMed, Court-Brown et al. prospectively studied 1027 proximal humeral fractures and found a unipolar age distribution with peak age-specific incidence in women aged 80-89 years, with roughly half of all fractures minimally displaced (PMID 11580125, DOI). Isolated greater tuberosity fractures account for a minority of this group and show a more bimodal pattern - younger patients sustaining high-energy or sporting injuries (frequently as part of an anterior dislocation) and older patients with low-energy falls on osteoporotic bone (Green and Izzi, PMID 14671536, DOI). Mutch et al. reported a mean age of 58 years across 199 isolated greater tuberosity fractures, with a female predominance (PMID 24788500, DOI).
Guideline & Society Guidance
There is no single high-level (RCT-based) guideline dedicated to isolated greater tuberosity fractures; recommendations are derived from proximal humeral fracture guidance and expert reviews. The table below summarises the position of major bodies and the level of supporting evidence.
- Position on GT fractures
- No mandatory operative criterion; shared decision-making. Limited/inconclusive evidence to favour surgery over non-operative care for most proximal humeral fractures
- Evidence level
- Limited / inconclusive
- Position on GT fractures
- Displaced fragments (commonly greater than 5mm) reduced and fixed to restore cuff footprint; fixation matched to morphology (avulsion/split/depression)
- Evidence level
- Expert consensus / III
- Position on GT fractures
- Process standards for proximal humeral trauma - prompt imaging, neurovascular documentation, early senior decision and physiotherapy
- Evidence level
- Standards of care
- Position on GT fractures
- Endorse displacement-based thresholds (greater than 5mm general, greater than 3mm overhead/active) with early mobilisation
- Evidence level
- Narrative / IV-V
- Position on GT fractures
- No GT-specific criterion; emphasises non-operative care for many proximal humeral fractures and early rehabilitation
- Evidence level
- Guideline (indirect)
The defining decision threshold across all bodies is displacement-based: greater than 5mm in the general population and greater than 3mm in active or overhead patients (George, PMID 17916784). No registry or randomised trial has overturned this.
Registry & Trial Evidence
No national joint registry captures isolated greater tuberosity fracture fixation, because these are bone-and-soft-tissue procedures rather than arthroplasty; registry data (AOANJRR, NJR, AJRR) are relevant only when displaced fracture-dislocations in the elderly proceed to reverse shoulder arthroplasty, where these registries report implant survivorship and revision rates. The randomised-trial evidence base specific to greater tuberosity fractures is sparse; the strongest comparative data remain cohort studies showing better function after fixation of genuinely displaced fragments versus non-operative treatment (Platzer, PMID 18349710, DOI) and excellent non-operative outcomes for minimally displaced (1-5mm) fractures (Platzer, PMID 15963996).
Practice Variation
Practice variation is driven by patient demand and bone quality rather than geography: screw or plate fixation predominates for large split fragments in good bone, whereas suture-anchor or transosseous suture constructs (including arthroscopic suture-bridge techniques) are favoured for comminuted, avulsion-type or osteoporotic fragments (Li et al., PMID 28401278, DOI). Arthroscopic fixation is concentrated in high-volume shoulder units with the requisite expertise. Imaging and specialist access also vary by setting rather than by country: plain radiography and CT are routinely available, whereas MRI access can be more limited outside major centres but is rarely required acutely; telehealth with image transfer increasingly supports regional and rural management with specialist input. In high-income settings, structured falls-prevention programmes help reduce the low-energy osteoporotic fracture burden in the elderly.
MCQ Practice
Self-Assessment Questions
Q: A 35-year-old tennis player sustains a greater tuberosity fracture with 4mm of superior displacement. Which factor would most influence your decision toward surgical management?
- A) Patient age
- B) Occupation as an overhead athlete
- C) Superior direction of displacement
- D) Fragment size
- E) Time from injury
A: B - The patient's occupation as an overhead athlete with high functional demands is the key factor. While the standard threshold is 5mm, many surgeons advocate 3mm threshold for overhead athletes requiring full shoulder function.
Q: Which rotator cuff tendon does NOT attach to the greater tuberosity?
- A) Supraspinatus
- B) Infraspinatus
- C) Teres minor
- D) Subscapularis
- E) All attach to the greater tuberosity
A: D - The subscapularis attaches to the lesser tuberosity, not the greater tuberosity. The three rotator cuff tendons that attach to GT are supraspinatus (superior), infraspinatus (middle), and teres minor (inferior facet).
Q: What is the most important radiographic view for assessing displacement of a greater tuberosity fracture?
- A) True AP (Grashey) view
- B) Scapular Y view
- C) Axillary view
- D) Internal rotation AP view
- E) External rotation AP view
A: C - The axillary view best shows posterior displacement of the GT fragment (the "crescent sign"). Posterior displacement is often the most functionally significant and may be missed on AP views.
Q: When performing a deltoid-splitting approach, how far distal to the acromion must the surgeon stay to avoid axillary nerve injury?
- A) 2cm
- B) 3cm
- C) 5cm
- D) 7cm
- E) 10cm
A: C - The deltoid split must stay within 5cm of the acromion to avoid injury to the axillary nerve, which courses around the surgical neck 5-7cm distal to the lateral acromion.
Q: What is the most common complication following treatment of greater tuberosity fractures?
- A) Non-union
- B) Avascular necrosis
- C) Stiffness
- D) Infection
- E) Hardware failure
A: C - Stiffness is the most common complication following both operative and non-operative treatment of GT fractures. This emphasizes the importance of early motion protocols.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old rugby player sustains an anterior shoulder dislocation during a tackle. After closed reduction, X-rays show a greater tuberosity fracture with 8mm of superior displacement. How would you manage this patient?”
“An 82-year-old woman with osteoporosis falls and sustains a greater tuberosity fracture with 7mm of posterior displacement. Her pre-injury Constant score was 70 and she lives independently. What is your approach?”
“At 3 months post-operative following screw fixation of a displaced greater tuberosity fracture, your patient has persistent pain and inability to elevate the arm above 90 degrees. The fracture is united on X-ray. What is your differential and management?”
“Describe the surgical approach and fixation technique you would use for a displaced greater tuberosity fracture in a 45-year-old patient with good bone quality.”
Key Facts
- Displacement threshold: 5mm standard, 3mm for overhead athletes
- Three cuff attachments: Supraspinatus (superior), Infraspinatus (middle), Teres minor (inferior)
- Posterior displacement worst - limits external rotation
- Superior displacement causes impingement
- 15-30% of anterior dislocations have associated GT fracture
- Axillary view shows posterior displacement (crescent sign)
- Deltoid split must stay within 5cm of acromion (axillary nerve)
- Screw fixation for large fragments with good bone
- Suture anchors for osteoporotic bone or comminution
Surgical Steps
- Beach chair position, arm draped free
- Deltoid-splitting approach from anterolateral acromion
- Split deltoid in line with fibers, stay within 5cm of acromion
- Identify fracture and rotator cuff attachment
- Reduce fragment anatomically
- Provisional K-wire fixation
- Place 2 cannulated screws toward medial calcar
- Bury screw heads below cortical surface
- Check fixation with fluoroscopy
Common Pitfalls
- Missing posterior displacement on AP views alone
- Treating displaced fractures non-operatively in active patients
- Extending deltoid split beyond 5cm (axillary nerve)
- Proud hardware causing impingement
- Prolonged immobilization causing stiffness
- Missing associated instability in fracture-dislocations
- Using screw fixation in osteoporotic bone
Examiner Favorites
- Describe rotator cuff attachments to greater tuberosity
- What is the surgical threshold for displacement?
- Why is posterior displacement worse than superior?
- What approach would you use and why?
- How do you protect the axillary nerve?
- How would you fix a GT fracture in osteoporotic bone?
- Management of GT fracture with anterior dislocation
Evidence Base
Key Studies
Platzer et al. - Operative vs Non-operative for Displaced GT Fractures
- Surgical cohort of 52 patients with displaced GT fractures compared with 9 treated non-operatively
- All operatively treated fractures healed with no nonunion; 80% achieved good or excellent shoulder scores
- Operative reduction and fixation gave significantly better function than non-operative treatment of displaced fragments (p less than 0.05)
Platzer et al. - Minimally Displaced GT Fractures (1-5mm)
- 135 patients with minimally displaced (1-5mm) GT fractures treated non-operatively, mean follow-up 3.7 years
- 97% achieved good or excellent results; displacement greater than 3mm gave slightly worse but non-significant outcomes
- Worse results in the eighth and ninth decades; female patients did significantly better than male patients
Mutch et al. - Morphological Classification (Avulsion/Split/Depression)
- 199 isolated GT fractures classified as avulsion (39%), split (41%) and depression (20%)
- Inter- and intra-observer reliability (kappa 0.69-0.86) superior to both Neer and AO classifications
- Distinct morphologies carry differing implications for pathophysiology and fixation technique
George - Fractures of the Greater Tuberosity (Review)
- GT fractures occur with anterior dislocation or by impaction against the acromion/superior glenoid
- Surgical fixation recommended for greater than 5mm displacement (general population) or greater than 3mm in active overhead patients
- Associated partial-thickness cuff and labral tears may cause persistent post-healing pain
Green and Izzi - Isolated GT Fractures (Review)
- Comprehensive review of epidemiology, anatomy, classification and treatment of isolated GT fractures
- Highlighted the paucity of outcome studies specific to isolated GT fractures
- Called for more precise diagnostic criteria and treatment selection
Li et al. - Arthroscopic Suture-Bridge Fixation
- 14 displaced/comminuted GT fractures (greater than 3mm) treated arthroscopically with a modified suture-bridge
- Mean ASES 97.5 and UCLA 32 at follow-up, with 13 of 14 rated good or excellent
- Demonstrates arthroscopic fixation as a viable option for avulsion/comminuted fragments
Court-Brown et al. - Epidemiology of Proximal Humeral Fractures
- Prospective 5-year population study of 1027 proximal humeral fractures
- Unipolar age distribution with peak age-specific incidence in women aged 80-89 years
- Roughly half of fractures are minimally displaced; the AO classification captured the spectrum better than Neer