Congenital | Iatrogenic | Traumatic | Flexible vs Rigid | EHL Transfer or Arthrodesis
- Hallux varus is medial deviation of great toe at MTP joint greater than 10 degrees
- Iatrogenic (post-bunion surgery) is most common cause in adults
- Flexible vs rigid determines treatment - test passive correctability
- EHL transfer is first-line surgery for flexible deformity
- Arthrodesis is definitive treatment for rigid, arthritic deformity
- “Always assess flexibility - passive correction test differentiates flexible from rigid
- “Iatrogenic causes: excessive medial eminence resection, overtightening of medial capsule
- “EHL transfer (Johnson procedure) addresses dynamic deforming force
- “First MTP arthrodesis in neutral/slight valgus is salvage for rigid deformity
Hallux varus is medial deviation of the hallux at the MTP joint greater than 10 degrees from the longitudinal axis of the first metatarsal. Measure on weight-bearing AP radiograph. Normal is 5-15 degrees valgus.
Critical distinction: Flexible deformity corrects passively, indicating soft tissue imbalance. Rigid deformity does not correct, suggesting joint contracture or arthrosis. This determines surgical approach.
Prevent after bunion surgery: Avoid excessive medial eminence resection (leaves lateral structures unopposed), overtightening medial capsule, or fibular sesamoid excision. Maintain sesamoid balance.
Flexible: EHL transfer (Johnson), +/- reverse Akin, +/- abductor release. Rigid: First MTP arthrodesis in neutral to 5-10° valgus. Congenital: Often observation, rarely surgery.
- Flexible Hallux Varus
- Corrects to neutral or valgus
- Rigid Hallux Varus
- Does not correct passively
- Flexible Hallux Varus
- Soft tissue imbalance (EHL, abductor hallucis)
- Rigid Hallux Varus
- Joint contracture, capsular fibrosis, arthritis
- Flexible Hallux Varus
- EHL transfer (Johnson procedure)
- Rigid Hallux Varus
- First MTP arthrodesis
- Flexible Hallux Varus
- Reverse Akin osteotomy, abductor release
- Rigid Hallux Varus
- Soft tissue releases (if contracture)
- Flexible Hallux Varus
- Good with appropriate soft tissue surgery
- Rigid Hallux Varus
- Reliable with arthrodesis, loss of motion
Overview and Epidemiology
Hallux varus is defined as medial deviation of the great toe at the first metatarsophalangeal (MTP) joint, with the hallux angulated medially relative to the long axis of the first metatarsal by more than 10 degrees. [1] In contrast to hallux valgus (bunion), the normal hallux has 5-15 degrees of valgus alignment. [2]


Epidemiology:
- Iatrogenic hallux varus occurs in approximately 5-15% of patients following hallux valgus correction surgery, making it the most common cause in adults. [3]
- Congenital hallux varus is rare, often associated with metatarsus adductus or as part of polydactyly syndromes. [4]
- Traumatic hallux varus follows crush injuries, burns, or medial soft tissue trauma with subsequent contracture.
- Gender distribution: Iatrogenic cases mirror bunion surgery demographics (predominantly female), while congenital cases have equal distribution.
Hallux varus significantly impairs push-off mechanics during gait. The first MTP joint normally bears 40-60% of forefoot weight during terminal stance. Varus malalignment shifts load laterally to lesser metatarsals, causing transfer metatarsalgia and gait inefficiency. [5] The deformity is also cosmetically distressing and causes shoe wear difficulty.
Historical context: The term "hallux varus" was first described in relation to overcorrection following bunion surgery in the mid-20th century. Early bunion operations often involved aggressive medial eminence resection and medial capsulorrhaphy without balancing lateral structures, leading to high rates of iatrogenic varus deformity. Modern bunion surgery emphasizes preservation of sesamoid balance and judicious soft tissue releases. [6]
Etiology
Etiology Classification
Hallux varus can be classified by etiology into three main categories:
- Causes
- Metatarsus adductus, delta phalanx, polydactyly remnant
- Characteristics
- Present at birth, usually flexible, may spontaneously improve
- Treatment Approach
- Observation if asymptomatic, soft tissue release if rigid
- Causes
- Post-bunion surgery: excessive medial eminence resection, overtight medial capsule, fibular sesamoidectomy
- Characteristics
- Most common in adults, variable flexibility, associated with prior surgery
- Treatment Approach
- Depends on flexibility - EHL transfer vs arthrodesis
- Causes
- Crush injury, burns, lacerations with medial contracture, rupture of lateral structures
- Characteristics
- History of trauma, scarring, may have skin quality issues
- Treatment Approach
- Release contractures, address scarring, reconstruct as needed
Iatrogenic Causes (Most Common)
The most frequent cause of hallux varus in adults is overcorrection during hallux valgus surgery. [7] Specific technical errors include:
- Removing too much medial bone eliminates the medial buttress.
- The unopposed pull of the abductor hallucis and extensor hallucis longus (EHL) pulls the toe medially.
- Risk increases if resection extends beyond the sagittal sulcus of the metatarsal head.
- Aggressive medial capsulorrhaphy or plication creates excessive medial tension.
- Combined with inadequate lateral release, this imbalances soft tissue forces.
- Common in older McBride-type procedures.
- The fibular sesamoid acts as a lateral buttress.
- Its removal eliminates lateral support and allows medial deviation.
- Risk is higher if combined with other medial-sided procedures.
- Injury to the lateral capsule, lateral collateral ligament, or adductor hallucis during exposure.
- Overzealous lateral soft tissue release in an attempt to correct severe bunion.
- Excessive varus angulation with distal metatarsal osteotomy (Chevron, scarf).
- Malunion in varus after proximal osteotomy.
Key principles to prevent iatrogenic hallux varus:
- Limit medial eminence resection to within the sagittal sulcus
- Preserve the fibular sesamoid unless severely diseased
- Balance medial and lateral soft tissue releases
- Aim for slight overcorrection to 10-15° valgus, not neutral
- Assess intraoperative sesamoid position - should be centered under metatarsal head
Congenital Causes
Congenital hallux varus is rare and typically presents in infancy or early childhood. [8] Causes include:
- Metatarsus adductus: The first metatarsal is deviated medially, creating relative hallux varus.
- Delta (trapezoid) phalanx: Abnormal wedge-shaped proximal phalanx drives progressive varus angulation.
- Polydactyly remnants: Incomplete resection or scarring after polydactyly excision.
- Congenital contracture: Tight abductor hallucis or medial capsular structures.
Most congenital cases are flexible and may improve with growth. Rigid cases or those with structural bone abnormalities require surgical correction.
Traumatic Causes
Post-traumatic hallux varus results from:
- Soft tissue contracture: Burns, crush injuries, or lacerations causing medial scar contracture.
- Disruption of lateral stabilizers: Rupture of lateral collateral ligament or adductor hallucis tendon.
- Malunion: Fractures of the first metatarsal or proximal phalanx healing in varus.
- Loss of fibular sesamoid: Traumatic excision or loss of sesamoid in severe injuries.
VARUSVARUS - Hallux Varus Etiology
Hook:VARUS causes - remember iatrogenic bunion surgery complications are most common
Pathophysiology
Soft Tissue Imbalance
The hallux is maintained in physiologic valgus alignment by a balance of forces:
- Abductor hallucis (inserts on medial base of proximal phalanx)
- Extensor hallucis longus (EHL) when toe is in varus position
- Medial capsule and collateral ligament
- Adductor hallucis (inserts on lateral base and fibular sesamoid)
- Flexor hallucis brevis (via both sesamoids)
- Lateral capsule and collateral ligament
- Fibular sesamoid acting as lateral buttress
In flexible hallux varus, the medial forces overpower the lateral forces, but the joint remains mobile and passively correctable. The EHL tendon, which normally runs in a straight line, now has a medial bowstring effect, acting as a dynamic deforming force. [9]
In rigid hallux varus, chronic imbalance leads to capsular contracture, adaptive shortening of medial structures, and eventual joint stiffness or arthrosis. The deformity becomes fixed and non-correctable.
Progression Warning: Flexible hallux varus, if left untreated, often progresses to rigid deformity over time as secondary adaptive changes occur. Early intervention in symptomatic flexible cases can prevent progression to arthrodesis requirement.
Clinical Presentation and Assessment
History
Key elements to elicit:
- Cosmetic concern (visible medial deviation)
- Difficulty with shoe wear (toe rubs on adjacent toe or medial shoe)
- Pain at MTP joint (especially if arthritic)
- Transfer metatarsalgia (pain under lesser metatarsal heads due to altered loading)
- Functional limitation (difficulty with push-off, sports)
- Duration of deformity (congenital vs acquired)
- Progressive vs stable
- Inciting event (surgery, trauma, or insidious onset)
- Previous treatments attempted
- Prior bunion surgery (timing, procedure type, complications)
- Revision surgeries
- Other foot procedures
- Numbness or tingling (nerve injury from prior surgery)
- Stiffness (suggests rigid deformity)
- Lesser toe pain (transfer metatarsalgia)
Physical Examination
- Standing alignment: Assess varus angle of hallux relative to first metatarsal
- Skin condition: Scarring from prior surgery or trauma, calluses on medial hallux or lateral lesser toes
- Adjacent toes: Crossover or crowding of second toe
- Hindfoot alignment: Assess for associated pes planus or cavus
- First MTP joint: Tenderness, effusion, crepitus (suggests arthritis)
- Medial eminence area: Prominence or deficiency (over-resection)
- Sesamoids: Palpate plantar aspect for tenderness, assess position
- Lesser metatarsal heads: Tenderness suggests transfer metatarsalgia
- MTP joint: Measure dorsiflexion and plantarflexion (normal 70-80° dorsiflexion, 20-30° plantarflexion)
- Interphalangeal (IP) joint: Assess flexion/extension
- Pain with motion: Crepitus or pain indicates arthritis
- Technique
- Grasp hallux and passively push laterally while stabilizing metatarsal
- Positive Finding
- Deformity corrects to neutral or valgus
- Interpretation
- FLEXIBLE deformity - soft tissue procedures feasible
- Technique
- Same maneuver
- Positive Finding
- Deformity does not correct
- Interpretation
- RIGID deformity - arthrodesis likely needed
- Technique
- Actively extend hallux IP joint against resistance
- Positive Finding
- EHL tendon visibly bowstrings medially, accentuates varus
- Interpretation
- EHL is dynamic deforming force - consider transfer
- Technique
- Palpate plantar foot for sesamoids
- Positive Finding
- Fibular sesamoid absent or displaced
- Interpretation
- Lateral buttress lost - complicates reconstruction
- Pulses (dorsalis pedis, posterior tibial)
- Sensation (distribution of deep peroneal, medial plantar, saphenous nerves)
- Motor function (EHL, FHL, intrinsics)
- Stance phase: Assess weight distribution, tendency to offload hallux
- Push-off: Observe for diminished hallux contribution, lateral forefoot loading
The passive correction test is the single most important clinical test. Firmly grasp the hallux and attempt to passively correct the varus deformity while stabilizing the first metatarsal. If the toe readily corrects past neutral into valgus, the deformity is flexible and amenable to soft tissue procedures like EHL transfer. If it does not correct, the deformity is rigid and arthrodesis is usually required.
Functional Impact
Hallux varus impairs forefoot mechanics:
- Reduced push-off power: The hallux generates up to 85% of push-off force in normal gait. [10]
- Transfer metatarsalgia: Load shifts from first to lesser metatarsal heads, causing pain and calluses.
- Gait instability: Loss of medial tripod support reduces balance.
- Shoe wear difficulty: Varus toe crowds second toe and creates abnormal pressure points.
FLEXIBLEFLEXIBLE - Assessment of Flexible Deformity
Hook:FLEXIBLE deformities are correctable and have better outcomes with soft tissue procedures
Investigations and Imaging
Radiographic Assessment
Standard radiographs are essential for diagnosis and surgical planning:
- Hallux varus angle: Measure angle between long axis of first metatarsal and proximal phalanx. Greater than 10° medial deviation confirms hallux varus. [11]
- First metatarsal position: Assess metatarsus primus varus (increased intermetatarsal angle may predispose to recurrence).
- Sesamoid position: Normally, sesamoids are centered beneath the metatarsal head. In varus, they shift laterally. Assess for absent fibular sesamoid.
- Joint space: Narrowing, osteophytes, or subchondral sclerosis indicate degenerative joint disease.
- Previous surgery evidence: Hardware, bone resection patterns.
- First MTP joint congruency: Assess for subluxation.
- Dorsal osteophytes: May limit dorsiflexion.
- Metatarsal declination: First ray position relative to lesser metatarsals.
- Better visualization of sesamoids and first MTP joint articular surfaces.
Advanced Imaging
- Rarely indicated for routine cases.
- Useful for:
- Assessing integrity of lateral soft tissue structures (adductor hallucis, lateral collateral ligament) in traumatic cases.
- Identifying occult osteonecrosis of sesamoids or metatarsal head.
- Pre-operative planning for complex revisions.
- Rarely needed.
- Can assess bone stock and prior screw tracts in multiply-operated feet.
- Useful for three-dimensional planning in severe deformities.
Classification Systems
There is no universally accepted classification for hallux varus. However, categorization by etiology (congenital, iatrogenic, traumatic) and flexibility (flexible vs rigid) is clinically most useful.
- Description
- Passively correctable to neutral or valgus, no fixed contracture
- Clinical Test
- Passive correction test positive
- Treatment
- Soft tissue procedures (EHL transfer, capsular release)
- Description
- Fixed deformity, does not correct, joint space preserved
- Clinical Test
- Passive correction test negative, ROM preserved
- Treatment
- Aggressive soft tissue releases +/- osteotomy, or arthrodesis
- Description
- Fixed deformity with joint degeneration
- Clinical Test
- Crepitus, pain, radiographic arthritis
- Treatment
- First MTP arthrodesis (definitive)
To measure hallux varus angle on weight-bearing AP radiograph:
- Draw line through long axis of first metatarsal shaft
- Draw line through long axis of proximal phalanx of hallux
- Measure angle formed at intersection
- Normal: 5-15° valgus (hallux angles laterally)
- Hallux varus: Greater than 10° medial deviation (hallux angles medially)
Differential Diagnosis
Medial deviation or a "crooked" great toe has several mimics. The key discriminators are the direction of deviation, the level of deformity, and the history.
- Direction / Level
- Medial deviation at MTP joint
- Key Distinguishing Features
- Hallux angled medially over 10 degrees; often post-bunion surgery; assess flexible vs rigid
- Imaging Clue
- WB AP: hallux medial to first metatarsal axis, sesamoids shifted laterally
- Direction / Level
- Lateral deviation at MTP joint
- Key Distinguishing Features
- Opposite direction - lateral drift; bunion prominence; the deformity surgery was meant to treat
- Imaging Clue
- Increased hallux valgus and intermetatarsal angles
- Direction / Level
- Medial deviation at IP joint of phalanx
- Key Distinguishing Features
- MTP joint aligned; deformity is distal, within the proximal phalanx (delta phalanx, malunion)
- Imaging Clue
- Apex of angulation at phalangeal shaft/IP, not MTP
- Direction / Level
- MTP hyperextension, IP flexion
- Key Distinguishing Features
- Sagittal-plane deformity; may coexist with varus after EHL imbalance
- Imaging Clue
- Lateral radiograph shows dorsiflexed MTP, flexed IP
- Direction / Level
- Variable MTP malalignment
- Key Distinguishing Features
- Polyarticular, synovitis, bilateral, lesser-toe deformities, systemic features
- Imaging Clue
- Erosions, joint destruction, periarticular osteopenia
- Direction / Level
- First ray (metatarsal) medial deviation
- Key Distinguishing Features
- Bone/forefoot is adducted producing relative hallux varus; common congenital association
- Imaging Clue
- Increased intermetatarsal angle, adducted metatarsals
Management Algorithm
Non-Operative Management
- Asymptomatic or minimally symptomatic deformity
- Congenital cases in young children (high rate of spontaneous improvement)
- Medical comorbidities precluding surgery
- Patient preference
- Observation: Many congenital cases improve with growth.
- Shoe modifications: Wide toe box shoes, soft uppers, custom orthotics to accommodate deformity.
- Toe spacers: Soft silicone spacers between hallux and second toe to provide lateral corrective force (limited efficacy).
- Taping/splinting: Dynamic splinting to hold toe in corrected position (may slow progression in flexible cases).
- Activity modification: Avoid aggravating activities.
Non-operative treatment does not correct the deformity but may reduce symptoms. Flexible deformities may progress to rigid over time despite conservative measures.
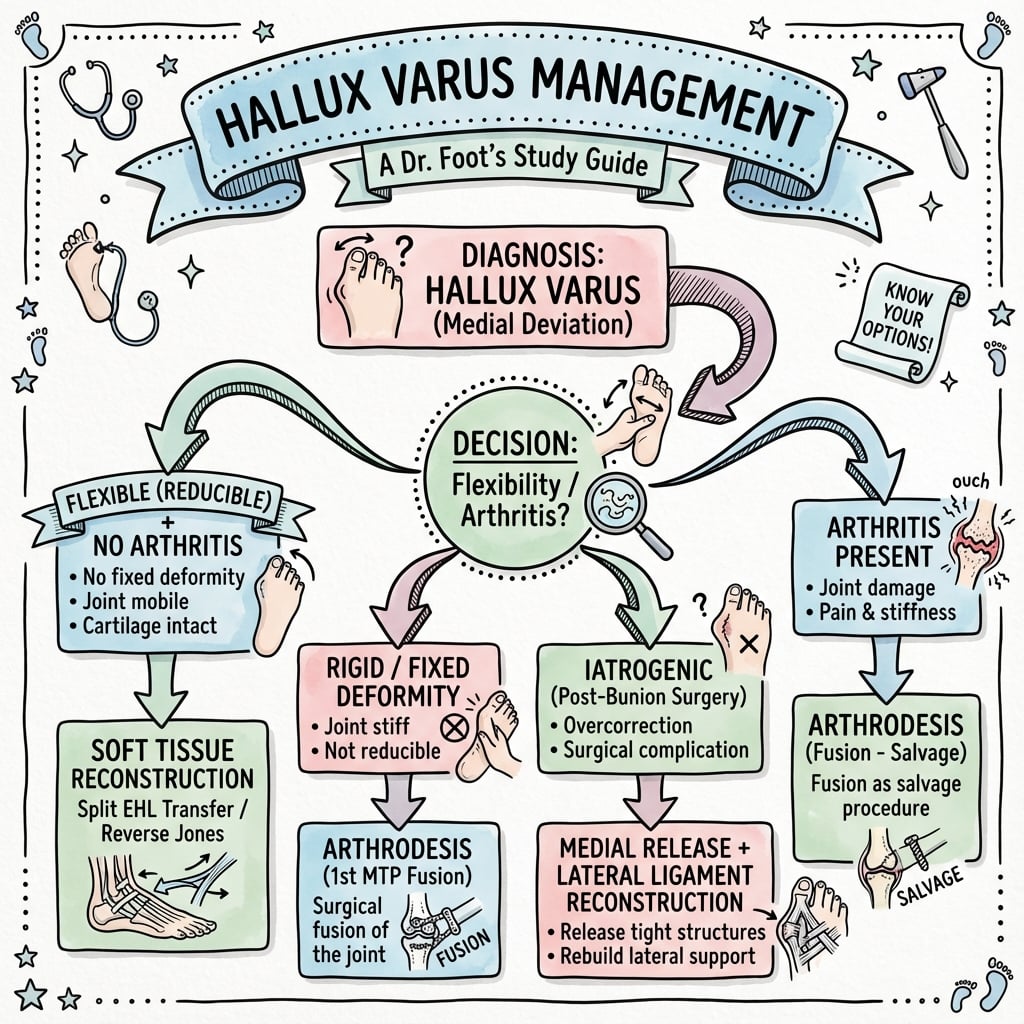
Operative Management - Decision Algorithm
Perform passive correction test under fluoroscopy if needed. Flexible = correctable. Rigid = fixed.
Review radiographs for arthritis. Arthritic joint narrows surgical options to arthrodesis.
EHL bowstringing? Abductor hallucis contracture? Capsular contracture? Bone deformity?
Flexible non-arthritic: EHL transfer +/- adjuncts. Rigid or arthritic: Arthrodesis. Bone deformity: Add osteotomy.
Surgical Options Overview
- Indication
- Flexible, non-arthritic, EHL bowstringing
- Technique Overview
- Transfer EHL to lateral capsule/proximal phalanx
- Outcomes
- 80-90% good results for flexible deformity
- Indication
- Medial soft tissue contracture
- Technique Overview
- Release abductor from medial base of proximal phalanx
- Outcomes
- Often combined with EHL transfer
- Indication
- Medial angulation of proximal phalanx
- Technique Overview
- Lateral closing wedge osteotomy of proximal phalanx
- Outcomes
- Adjunct to soft tissue procedures
- Indication
- Rigid, arthritic, salvage for failed soft tissue procedures
- Technique Overview
- Fuse MTP joint in 10-15° valgus, 20-25° dorsiflexion
- Outcomes
- Definitive correction, loss of motion, 90% satisfaction
- Indication
- Metatarsus primus varus component
- Technique Overview
- Correct metatarsal alignment (valgus-producing osteotomy)
- Outcomes
- Rarely needed as isolated procedure
Surgical Techniques
EHL Transfer (Johnson Procedure)
- Flexible hallux varus
- Non-arthritic first MTP joint
- EHL bowstringing identified as dynamic deforming force
- Failed conservative management
- Rigid deformity (does not correct passively)
- Arthritic MTP joint
- Severe bone deformity requiring osteotomy
- Poor soft tissue envelope
The EHL, when the toe is in varus, acts as a medial deforming force creating a bowstring effect. Transferring the EHL to the lateral side of the proximal phalanx eliminates the medial pull and creates a new lateral stabilizing force. [12]
- Supine on operating table
- Thigh tourniquet (or ankle tourniquet)
- Bump under ipsilateral hip for foot flat positioning
- Dorsal longitudinal incision over first MTP joint, centered over the joint line, approximately 4-5 cm long.
- Extends from midshaft of first metatarsal to midshaft of proximal phalanx.
- Incise skin and subcutaneous tissue, preserving dorsal cutaneous nerves.
- Identify EHL tendon in the center of the wound.
- Open extensor hood longitudinally over the MTP joint.
- Transect EHL tendon sharply at the level of the base of the proximal phalanx (distal to the MTP joint).
- Deliver proximal stump of EHL into wound with gentle traction.
- The EHL will retract slightly but remains accessible.
- Retract EHL tendon medially to expose lateral capsule.
- Identify lateral collateral ligament and adductor hallucis insertion.
- Create lateral capsulotomy if tight (often the capsule is attenuated in chronic varus).
- Create bone tunnel in lateral aspect of proximal phalanx base OR prepare suture anchor site.
- Bone tunnel technique: Drill 3.5-4 mm tunnel from dorsolateral to plantar-medial through proximal phalanx base.
- Pass heavy non-absorbable suture (e.g., No. 2 FiberWire) through EHL tendon using Krackow or whipstitch technique.
- Thread sutures through bone tunnel from dorsolateral to plantar-medial.
- Hold hallux in corrected position (neutral to 5-10° valgus).
- Tie sutures on plantar-medial cortex over button or post, tensioning EHL to lateral side.
- Place suture anchor in lateral base of proximal phalanx.
- Suture EHL to lateral capsule and periosteum using anchor.
- Extend incision medially or make separate medial incision.
- Release abductor hallucis from medial base of proximal phalanx.
- Release medial capsule if contracted.
- If significant proximal phalanx medial angulation persists after soft tissue correction.
- Perform lateral closing wedge osteotomy at proximal phalanx base.
- Fix with single screw or K-wire.
- Close extensor hood loosely with absorbable suture.
- Close subcutaneous layer.
- Close skin with nylon or absorbable subcuticular suture.
- Apply bulky dressing with hallux held in slight valgus with gauze between hallux and second toe.
- Week 0-2: Non-weight-bearing in posterior splint or CAM boot, hallux held in valgus with gauze spacer.
- Week 2-6: Protected weight-bearing in stiff-soled shoe or boot, continue toe spacer.
- Week 6-12: Progressive return to normal shoe wear and activities.
- IP joint ROM exercises begin at 2 weeks to prevent stiffness (EHL function to IP preserved via extensor hood).
- Success rate of 80-90% in appropriately selected flexible cases. [13]
- Complications: EHL weakness to IP joint (usually mild), recurrence if poor technique or patient selection, wound healing issues.
This completes the EHL transfer surgical technique.
Split EHL Transfer (Modified Johnson)
The controversies section and MCQ both mention a "split EHL transfer" as a modern alternative to the original Johnson procedure, and the Skalley series used it, but the modification is never explained - and it changes the post-operative reality for the patient.
- The problem with the original Johnson. The classic Johnson EHL transfer divides the whole EHL and reroutes it laterally, which removes active extension of the interphalangeal (IP) joint; to prevent the resulting cock-up/claw of the IP joint, Johnson combined it with a first IP arthrodesis (fusion). That IP fusion is the price of the original operation.
- The split modification. In a split EHL transfer only the lateral half of the EHL is detached and transferred laterally to correct the varus, while the medial half is left intact and in continuity to keep extending the IP joint. This avoids the IP arthrodesis and preserves active IP extension, at the cost of a slightly weaker corrective vector (half the tendon).
- How to choose. The split transfer is favoured when preserving IP motion matters and the deforming force is not extreme; the complete transfer (with IP fusion) is reserved for a strong dynamic deformity or when the IP joint is already stiff or arthritic, so its fusion is no loss. Either way the principle is the same - convert the EHL from a medial deformer into a lateral stabiliser.
Q: What is the split EHL transfer and how does it differ from the original Johnson procedure? A: The original Johnson transfers the whole EHL laterally and therefore adds a first IP arthrodesis to prevent an IP claw once IP extension is lost. The split EHL transfer moves only the lateral half of the tendon (the medial half stays in continuity to keep extending the IP joint), so it avoids the IP fusion and preserves IP motion, trading a little corrective power. Choose the split transfer to preserve IP motion; keep the complete transfer (with IP fusion) for a strong deformity or an already-stiff IP joint.
JOHNSONJOHNSON - EHL Transfer Procedure
Hook:JOHNSON procedure transfers EHL laterally to correct flexible hallux varus
Alternative Tendon Transfers and Static Ligamentoplasty
The evidence base (Plovanich, Schwagten) and the controversies section list a menu of tendon transfers and static reconstructions beyond the Johnson EHL transfer - abductor hallucis (Hawkins), reverse abductor hallucis, extensor hallucis brevis (EHB/Myerson) and first-dorsal-interosseous (Valtin) - but only the EHL transfer is developed.
- Abductor hallucis (Hawkins) transfer - dynamic. The abductor hallucis is itself one of the medial deforming forces; releasing it from the medial base and transferring it laterally removes a deformer and adds a lateral pull. It is an option when the EHL is not the dominant deformer, and it preserves the EHL entirely.
- Reverse abductor hallucis transfer - static ligamentoplasty. Here the abductor hallucis (or a slip of it) is used as a static lateral tether/ligamentoplasty that recreates the deficient lateral collateral/adductor buttress. It is attractive because it spares the EHL and the IP joint, but modern long-term data (Schwagten: about 69% satisfaction at a mean of 4 years) show that late loss of correction can occur, so patients must be counselled.
- Extensor hallucis brevis (EHB, Myerson) transfer - dynamic, EHL-sparing. The EHB can be transferred laterally as a dynamic corrector while leaving the EHL intact, avoiding any loss of IP or MTP extension power.
- How to choose. With no comparative trials, selection is by the dominant deforming force and the wish to spare the EHL/IP joint: an EHL-driven bowstring favours an EHL (ideally split) transfer; a supple deformity where EHL preservation is desired favours a reverse abductor ligamentoplasty or an EHB transfer; all are combined with the necessary medial release.
Q: Besides the EHL transfer, what other tendon transfers or reconstructions correct flexible hallux varus? A: The abductor hallucis (Hawkins) transfer (release the medial deformer and reroute it laterally), the reverse abductor hallucis transfer used as a static lateral ligamentoplasty (spares the EHL/IP joint but can lose correction late - Schwagten about 69% satisfaction), and the extensor hallucis brevis (Myerson) transfer (dynamic, EHL-sparing). Selection is by the dominant deforming force and whether you want to spare the EHL/IP joint; all are combined with a medial release, and no comparative trial favours one.
Complications
Complications of Hallux Varus Itself (Untreated)
- Transfer metatarsalgia: Lateral shift of weight-bearing load causes pain under second and third metatarsal heads. [17]
- Progression to rigidity: Flexible deformities become rigid over time due to capsular contracture.
- Arthritis: Abnormal joint mechanics accelerate degenerative changes.
- Shoe wear difficulty: Cosmetic and functional impairment.
- Gait dysfunction: Reduced push-off power, compensatory gait patterns.
Surgical Complications
- Infection: 1-3% with standard precautions. Higher risk in revision surgery or compromised soft tissues.
- Wound healing problems: Dorsal foot has thin skin and limited vascularity. Risk increases with multiple prior surgeries or smoking.
- Nerve injury: Dorsal cutaneous nerves at risk during incision. Causes numbness or neuroma.
- Deep vein thrombosis/pulmonary embolism: Rare in foot surgery but consider prophylaxis in high-risk patients.
- Recurrence of varus deformity: 10-20% if inadequate transfer tension, poor patient selection (rigid deformity), or failure to address all deforming forces. [18]
- Loss of IP extension strength: The EHL normally extends the IP joint. After transfer, IP extension is weaker (though extensor hood mechanism preserves some function). Usually well-tolerated.
- Overcorrection to valgus: Rare. Occurs if transfer is too tight or combined procedures create excessive valgus force.
- Tendon pull-out or failure: If fixation is inadequate. Use strong suture technique and bone tunnel or solid anchor.
- Non-union: 5-10% overall. Higher with smoking, poor bone quality, inadequate fixation, or infection. [19]
- Malunion: Fusion in incorrect position (excessive or insufficient dorsiflexion, persistent varus, rotation). Requires revision arthrodesis or osteotomy.
- Hardware complications: Prominent screws or plates causing irritation, requiring removal.
- Transfer metatarsalgia: Loss of MTP motion shifts load to lesser metatarsals. Occurs in 10-20% long-term.
- Hallux IP joint arthritis: Increased stress on IP joint over time due to loss of MTP motion.
- Shortening: Excessive bone resection during joint preparation can shorten hallux.
- Non-union: Rare in metaphyseal bone.
- Malunion: Incorrect wedge size causing under- or overcorrection.
- Fracture: Proximal phalanx fracture if osteopenic bone or trauma.
Prevention Strategies
- Limit medial eminence resection: Stay within sagittal sulcus.
- Preserve fibular sesamoid: Avoid routine sesamoidectomy.
- Balance soft tissue releases: Proportional medial and lateral releases.
- Avoid overtightening medial capsule: Plication should restore anatomy, not overcorrect.
- Assess intraoperative sesamoid position: Sesamoids should be centered under metatarsal head.
- Aim for slight valgus: Target 10-15° valgus, not neutral.
- Correct patient selection: Flexible cases for soft tissue procedures, rigid for arthrodesis.
- Address all deforming forces: EHL transfer alone may fail if medial contractures not released.
- Adequate fixation: Strong suture technique for tendon transfers, rigid fixation for osteotomies.
- Post-operative protection: Maintain correction with splinting during healing phase.
Post-operative Care and Rehabilitation
Immediate Post-operative Period (0-2 weeks)
- Bulky compressive dressing with gauze between hallux and second toe to maintain corrected position.
- Posterior splint or CAM boot for protection.
- Elevate foot above heart level to reduce swelling.
- Non-weight-bearing for soft tissue procedures (EHL transfer, releases) for first 2 weeks.
- Non-weight-bearing for arthrodesis if screw fixation; protected weight-bearing may be allowed with rigid plate fixation (surgeon preference).
- Keep dressing clean and dry.
- First dressing change at 10-14 days with suture removal.
- Multimodal analgesia: acetaminophen, NSAIDs (if not contraindicated for bone healing), opioids as needed for first few days.
Early Rehabilitation Phase (2-6 weeks)
- Week 2-6: Transition to protected weight-bearing in stiff-soled shoe or CAM boot.
- Continue toe spacer (gauze or silicone) between hallux and second toe.
- Begin gentle IP joint ROM exercises at 2 weeks to prevent stiffness (EHL still functions to IP via extensor hood).
- Avoid forceful MTP motion until 6 weeks (allow soft tissues to heal).
- Week 2-6: Protected weight-bearing in CAM boot or post-op shoe.
- No MTP joint motion (fusion is the goal).
- Radiographs at 6 weeks to assess early healing.
Late Rehabilitation Phase (6-12 weeks)
- Week 6+: Progressive return to normal shoe wear.
- Begin active MTP ROM exercises (if not arthrodesis).
- Strengthening exercises for intrinsic muscles.
- Return to athletic activities at 10-12 weeks if healing is adequate.
- Week 6-12: Continue protected weight-bearing until radiographic union (typically 8-12 weeks).
- Once fused, transition to normal shoe wear.
- Return to full activities at 12-16 weeks.
Long-term Follow-up
- Radiographs: At 6 weeks, 12 weeks, and 6 months to assess alignment, hardware, and union (for arthrodesis).
- Functional assessment: Gait analysis, shoe wear patterns, pain levels, patient satisfaction.
- Monitor for complications: Recurrence, transfer metatarsalgia, hardware prominence.
Maintaining the corrected position during the healing phase is critical. A simple gauze or silicone toe spacer between the hallux and second toe provides a gentle lateral force that helps prevent early recurrence as soft tissues heal. Continue for at least 6 weeks post-operatively.
Guidelines, Registries & Global Practice
Global epidemiology:
- Hallux varus is uncommon worldwide; the dominant aetiology in adults is iatrogenic overcorrection after hallux valgus surgery, reported across surgical series at roughly 2-13% depending on technique and definition.
- Reported cohorts are overwhelmingly female, mirroring the demographics of bunion surgery.
- Congenital cases are rare and have equal sex distribution; traumatic/burn-related cases follow injury patterns and are over-represented in lower-resource and high-burn-incidence regions.
Guidance and consensus (no dedicated single-society guideline exists):
- Position relevant to hallux varus
- Algorithm by flexibility and joint status; EHL or abductor transfer for supple non-arthritic deformity, arthrodesis for rigid/arthritic
- Position relevant to hallux varus
- Emphasise prevention during hallux valgus correction (avoid over-resection, preserve fibular sesamoid); reconstruction by foot and ankle specialists
- Position relevant to hallux varus
- First MTP arthrodesis principles: congruent surface preparation, 10-15 degrees valgus and 20-25 degrees dorsiflexion, dorsal plate +/- lag screw
- Position relevant to hallux varus
- Support both dynamic (EHL/EHB) transfers and static (reverse abductor hallucis ligamentoplasty) reconstruction for flexible iatrogenic varus
- Hallux varus is not tracked as a primary outcome in arthroplasty registries (NJR, AJRR, AOANJRR, SHAR). The relevant registry-adjacent evidence is forefoot/first-ray surgery audit data showing that varus is a recognised but infrequent complication of bunion correction, and that arthrodesis non-union rates sit around 5-10% across large series and systematic reviews.
- Well-resourced settings: weight-bearing radiographs, dorsal locking-plate arthrodesis, anchor/tendon-transfer reconstruction, and access to revision foot-and-ankle fellowship expertise.
- Limited-resource settings: greater reliance on clinical assessment, K-wire or crossed-screw fixation for fusion, and simpler soft-tissue procedures; congenital and burn-contracture varus form a larger share of the caseload.
Controversies & Areas of Uncertainty
No randomised data compare dynamic tendon transfers (Johnson EHL, abductor hallucis/Hawkins, EHB) with static ligamentoplasty (reverse abductor hallucis). Evidence is level IV-V with small, female-predominant cohorts; choice remains surgeon preference and local expertise.
The original Johnson procedure included first IP joint fusion to prevent clawing once the EHL is rerouted. Many surgeons now use split EHL transfer to preserve IP extension and avoid fusion, but comparative evidence for this modification is limited.
There is no universally accepted classification and no consensus threshold angle; values from "any medial deviation" to "over 10-15 degrees" appear in the literature. This hampers pooling of outcome data.
For the rigid but minimally arthritic joint, the role of osteotomy or arthroplasty/implant versus going straight to arthrodesis is unsettled; arthrodesis remains the most reliable but sacrifices motion.
The exact "safe" limits of medial eminence resection and lateral release are not precisely defined; recommendations (stay within the sagittal sulcus, preserve the fibular sesamoid, aim for slight valgus) are consensus-based rather than trial-proven.
Long-term data show meaningful late loss of correction with soft-tissue procedures (e.g. 31% sub-optimal satisfaction at mean 48 months for reverse abductor transfer), so durability and the true recurrence rate over a decade remain uncertain.
MCQ Practice Points
Q: What is the most common cause of hallux varus?
A: Iatrogenic following hallux valgus surgery - most commonly after excessive medial capsular plication, over-resection of medial eminence, over-correction of IMA, or lateral release with fibular sesamoid excision. Disruption of lateral stabilizers (adductor hallucis, lateral capsule, sesamoid complex) leads to medial deviation.
Q: What are the components of the deformity in hallux varus?
A: Medial deviation of proximal phalanx at MTP joint, supination of hallux (rotation), often combined with IPJ flexion (cock-up deformity). May be flexible (correctable passively) or rigid (fixed). Flexible deformity amenable to soft tissue procedures; rigid deformity requires bony procedures or fusion.
Q: What are the surgical options for flexible hallux varus?
A: Soft tissue procedures: EHL transfer (split or complete) to lateral proximal phalanx base, abductor hallucis release, reverse McBride (medial release, lateral repair). Johnson procedure: EHL transfer through P1 base tunnel. For rigid deformity: MTP fusion in 15° valgus, or corrective osteotomy.
Q: What is the reverse McBride procedure for hallux varus?
A: Medial soft tissue release (medial capsulotomy, abductor hallucis release) combined with lateral soft tissue reconstruction (adductor hallucis repair, lateral capsular plication). Essentially reverse of McBride bunionectomy. Effective for mild flexible deformity without MTP arthritis. Often combined with EHL transfer for better correction.
Q: What is the position of MTP fusion for hallux varus?
A: 15° valgus relative to first metatarsal, 10-15° dorsiflexion relative to floor (simulating toe-off), neutral rotation. Same fusion position as for hallux rigidus or severe hallux valgus. Preferred treatment for rigid hallux varus with MTP arthritis. Provides pain relief and stable push-off. High union rates with modern fixation.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old woman presents 18 months after hallux valgus correction surgery. She complains of medial deviation of her great toe, difficulty with shoe wear, and pain at the first MTP joint. On examination, the hallux is deviated medially approximately 15 degrees. When you grasp the toe and push it laterally, it easily corrects past neutral into slight valgus. Radiographs show no arthritis but the fibular sesamoid appears absent. What is your diagnosis and management plan?”
“A 60-year-old man presents with painful hallux varus that has been progressive over 5 years. He has no history of prior surgery. On examination, the hallux is deviated medially about 20 degrees and when you attempt passive correction, the toe does not move - it is rigid. There is crepitus and pain with attempted MTP joint motion. Radiographs show narrowing of the first MTP joint space with subchondral sclerosis and osteophytes. What is your management?”
“The parents of a 3-year-old boy bring him to clinic concerned about the appearance of his right great toe, which points inward. He was born with this and it has not changed. He is walking well and has no pain. On examination, the right hallux is in about 15 degrees of varus. When you push the toe laterally, it easily corrects to neutral and beyond. There is no skin tightness or scarring. Radiographs show no bone abnormality, normal joint spaces, and the metatarsus is slightly adducted. What do you advise the parents?”
Definition
- Medial deviation of hallux at MTP joint greater than 10° (normal is 5-15° valgus)
- Measure on weight-bearing AP radiograph
- Normal hallux has slight valgus alignment
Etiology (3 Types)
- 1. Congenital: Present at birth, often with metatarsus adductus, usually flexible
- 2. Iatrogenic (MOST COMMON in adults): Post-bunion surgery 5-15% incidence
- - Excessive medial eminence resection (beyond sagittal sulcus)
- - Overtightening medial capsule
- - Fibular sesamoidectomy (loss of lateral buttress)
- - Disruption of lateral structures (LCL, adductor hallucis)
- 3. Traumatic: Burns, crush, medial soft tissue contracture
Classification (Clinical)
- FLEXIBLE: Passively corrects to neutral/valgus - soft tissue imbalance (EHL, abductor)
- RIGID: Does not correct - joint contracture/capsular fibrosis/arthritis
- Flexibility determines treatment approach - TEST PASSIVELY
Clinical Assessment
- History: Prior bunion surgery? Congenital? Trauma? Progressive?
- Exam: Varus angle, PASSIVE CORRECTION TEST (key), EHL bowstringing
- Palpate sesamoids (fibular sesamoid absent?), assess MTP ROM, crepitus
- Radiographs: Weight-bearing AP (measure angle), assess joint space, sesamoid position
Treatment Algorithm
- Conservative: Observation (congenital), shoe mods, toe spacers, splinting
- FLEXIBLE: EHL transfer (Johnson procedure) +/- abductor release +/- reverse Akin
- RIGID: First MTP arthrodesis (10-15° valgus, 20-25° dorsiflexion)
- Arthritis: Arthrodesis is definitive
EHL Transfer (Johnson)
- Indication: Flexible hallux varus, EHL bowstringing, non-arthritic joint
- Technique: Divide EHL at proximal phalanx base, transfer to lateral capsule/bone
- Fixation: Bone tunnel or suture anchor, hold in corrected position
- Outcome: 80-90% success in flexible cases
- Complication: IP extension weakness (mild), 10-20% recurrence
First MTP Arthrodesis
- Indication: Rigid, arthritic, salvage for failed soft tissue procedures
- Position: 10-15° valgus, 20-25° dorsiflexion relative to ground
- Fixation: Dorsal plate (preferred) or crossed screws
- Fusion rate: 90-95% with plate
- Outcome: 85-90% satisfaction, loss of MTP motion
Prevention (During Bunion Surgery)
- Limit medial eminence resection within sagittal sulcus
- Preserve fibular sesamoid (avoid routine sesamoidectomy)
- Balance soft tissue releases (medial and lateral proportional)
- Avoid overtightening medial capsule
- Target 10-15° valgus, NOT neutral
- Check intraop sesamoid position (should be centered)
Exam Pearls
- Passive correction test = THE key clinical maneuver (flexible vs rigid)
- Iatrogenic is most common cause in adults (5-15% after bunion surgery)
- Congenital cases usually improve with growth - observation first
- EHL transfer for flexible, arthrodesis for rigid - simple algorithm
- Fusion position critical: 20-25° dorsiflexion (too much = heel walk, too little = no heel rise)
Evidence Base
Iatrogenic Hallux Varus - Cause, Prevention, Correction (Classic)
- Foundational paper describing acquired hallux varus as a complication of bunion surgery
- Excessive medial eminence resection, fibular sesamoidectomy and overtight medial capsulorrhaphy identified as causes
- Loss of the fibular sesamoid removes the lateral buttress and predisposes to medial drift
- Hawkins abductor hallucis tendon transfer first described as a correction technique
EHL Transfer for Hallux Varus - Original Description (Johnson)
- Original description of the Johnson EHL transfer for dynamic hallux varus
- Fifteen affected great toes treated; deformity attributed to dynamic tendon imbalance after McBride-type surgery
- EHL routed beneath the intermetatarsal ligament into the base of the proximal phalanx, with first IP joint arthrodesis
- Overall satisfactory correction of the varus deformity reported in the series
First MTP Arthrodesis with Plate Fixation - Outcomes
- 47 patients (58 feet) underwent first MTP fusion with a Vitallium dorsal plate
- 98% (57 of 58 feet) successfully fused; 93% reported good or excellent results
- Cone- or cup-shaped reamers used to create congruous, broadly apposed surfaces
- Plate removal required in only 7%; one nonunion with plate breakage and one delayed union
Congenital Hallux Varus (Classic Description)
- Classic surgical description of congenital hallux varus and its anatomy
- Deformity associated with short, broad first metatarsal, accessory bones and medial soft-tissue tethering
- Surgical correction addresses the medial tether and any duplicated/abnormal osseous structures
- Provides the historical basis for distinguishing congenital from acquired hallux varus
Operative Treatment of Acquired Hallux Varus - Algorithm
- 42 patients (45 feet) with acquired hallux varus; 36 followed prior hallux valgus surgery
- Procedure selection driven by aetiology, age/activity, and the site of primary deformity
- Treatments ranged from soft-tissue release with tendon transfer (17) to arthrodesis (17) and resection arthroplasty (7)
- Pain, shoe-wear difficulty and MTP instability improved across all treatment groups; treatment algorithm proposed
Soft-Tissue Release with Tendon Transfer for Flexible Hallux Varus
- Systematic review of 8 studies, 52 patients (all female), 68 feet treated for flexible iatrogenic hallux varus
- Tendon transfers: Johnson EHL with IP arthrodesis (41 feet), Hawkins abductor (9), reverse Hawkins (7), Valtin (7), Myerson EHB (4)
- Overall complication rate 16.2% (11/68); recurrent varus in only 4.4% (3 feet), all after Johnson EHL transfer
- Sustainable correction achievable with capsular release plus a variety of tendon transfers
Reverse Abductor Hallucis Transfer - Long-Term Results
- Prospective observational study, 16 female patients, 100% follow-up (mean 48 months, range 10-101)
- Success satisfaction rate of 69% (11/16); satisfaction correlated strongly with maintained alignment (r=0.77)
- Coronal/sagittal malalignment were the most disabling complications
- Effective for supple iatrogenic varus but patients must be counselled that late loss of correction can occur
References
-
Mann RA, Coughlin MJ. Hallux varus. In: Mann RA, Coughlin MJ, editors. Surgery of the Foot and Ankle. 6th ed. St. Louis: Mosby; 1993. p. 321-334.
-
Coughlin MJ, Saltzman CL, Anderson RB. Mann's Surgery of the Foot and Ankle. 9th ed. Philadelphia: Elsevier; 2014.
-
Edelman RD. Iatrogenic hallux varus. Foot Ankle Surg. 2015;21(4):223-227. doi:10.1016/j.fas.2015.07.003
-
Farmer AW. Congenital hallux varus. Am J Surg. 1958;95(2):274-278. doi:10.1016/0002-9610(58)90515-4
-
Hutton WC, Dhanendran M. The mechanics of normal and hallux valgus feet: a quantitative study. Clin Orthop Relat Res. 1981;(157):7-13.
-
Hawkins FB. Acquired hallux varus: cause, prevention and correction. Clin Orthop Relat Res. 1971;76:169-176.
-
Skalley TC, Myerson MS. The operative treatment of acquired hallux varus. Clin Orthop Relat Res. 1994;(306):183-191.
-
McElvenny RT. Hallux varus. Q Bull Northwest Univ Med Sch. 1941;15:277-280.
-
Johnson KA, Spiegl PV. Extensor hallucis longus transfer for hallux varus deformity. J Bone Joint Surg Am. 1984;66(5):681-686.
-
Shereff MJ, Bejjani FJ, Kummer FJ. Kinematics of the first metatarsophalangeal joint. J Bone Joint Surg Am. 1986;68(3):392-398.
-
Coughlin MJ, Roger A. Mann Award. Juvenile hallux valgus: etiology and treatment. Foot Ankle Int. 1995;16(11):682-697.
-
Johnson KA, Spiegl PV. Extensor hallucis longus transfer for hallux varus deformity. J Bone Joint Surg Am. 1984;66(5):681-686.
-
Chacon YP, Lam T. Extensor hallucis longus transfer for correction of hallux varus: long-term follow-up. J Foot Ankle Surg. 2012;51(6):687-691. doi:10.1053/j.jfas.2012.07.008
-
Coughlin MJ, Abdo RV. Arthrodesis of the first metatarsophalangeal joint with Vitallium plate fixation. Foot Ankle Int. 1994;15(1):18-28. doi:10.1177/107110079401500105
-
Roukis TS. Nonunion after arthrodesis of the first metatarsophalangeal joint: a systematic review. J Foot Ankle Surg. 2011;50(6):710-713. doi:10.1053/j.jfas.2011.06.010
-
Akin OF. The treatment of hallux valgus: a new operative procedure and its results. Med Sentinel. 1925;33:678-683.
-
Vandeputte G, Dereymaeker G, Steenwerckx A, Peeraer L, Broos P. The Weil osteotomy of the lesser metatarsals: a clinical and pedobarographic follow-up study. Foot Ankle Int. 2000;21(5):370-374. doi:10.1177/107110070002100502
-
Leemrijse T, Hoang B, Maldague P, Docquier PL, Valtin B. A new surgical procedure for iatrogenic hallux varus: reverse transfer of the abductor hallucis tendon. A report of 7 cases. Acta Orthop Belg. 2008;74(2):227-234.
-
Politi J, John H, Njus G, Bennett GL, Kay DB. First metatarsal-phalangeal joint arthrodesis: a biomechanical assessment of stability. Foot Ankle Int. 2003;24(4):332-337. doi:10.1177/107110070302400408