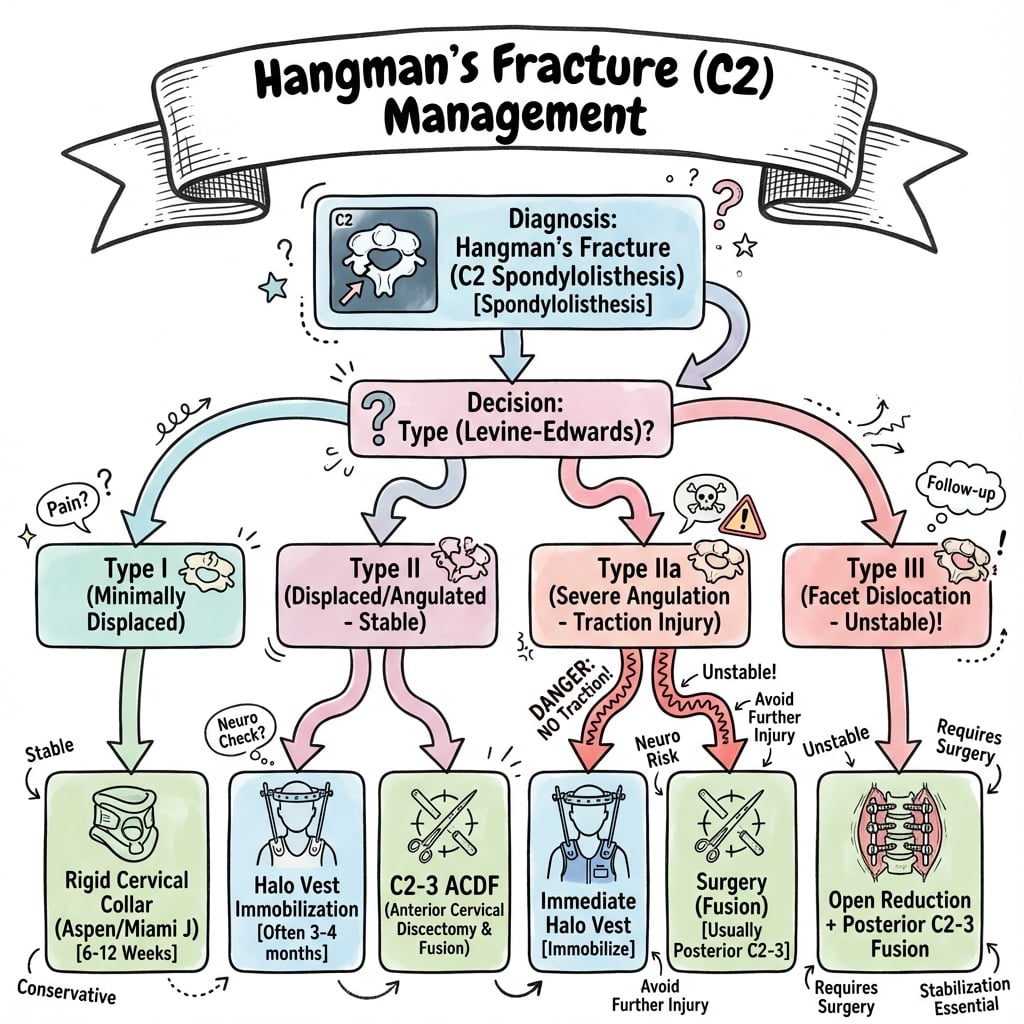
Bilateral Pars Fracture | Levine-Edwards Classification | Type IIA - No Traction
- Type IIA: Traction is CONTRAINDICATED - flexion-distraction injury
- Auto-decompression explains low neurological injury rate (canal expands)
- Measure translation AND angulation on lateral radiograph
- Type IIA: angulation out of proportion to translation (greater than 11 degrees, less than 3mm)
- Most treated non-operatively (collar or halo) - surgery for Type III or failed conservative
- “Type IIA recognition: angulation greater than translation (greater than 11 degrees, less than 3mm)
- “All types can have severe injury but neurological deficit rare (canal expands)
- “Associated head/facial trauma common (forehead impact mechanism)
Orthopaedic examiners test the Levine-Edwards classification and specific management for each type. The most commonly tested pitfall is Type IIA - recognizing that traction is CONTRAINDICATED because it will worsen the flexion-distraction injury. Type IIA has minimal translation but marked angulation.
Overview and Clinical Significance

The C2 Pars Fracture
Hangman's fracture (traumatic spondylolisthesis of C2) is a bilateral fracture through the pars interarticularis of the axis. The term derives from the similar fracture pattern caused by judicial hanging, though modern cases are typically from motor vehicle accidents.
- 4-7% of all cervical fractures
- Most common C2 fracture (excluding odontoid)
- Peak: young adults (MVA), elderly (falls)
- Male predominance
- Neurological injury only 6%
- Hyperextension + axial load (most common)
- Motor vehicle accident (forehead strike)
- Falls from height
- Diving accidents
- Type IIA: flexion-distraction
- Bilateral pars fracture creates "auto-decompression"
- Posterior ring separates from anterior elements
- Canal diameter increases with injury
- Contrast with burst fractures that narrow canal
- "Jefferson expands, Hangman's translates but opens"
Historical Context
Sir Geoffrey Jefferson first described the mechanism in 1927, relating it to judicial hanging. In judicial hanging:
- Drop causes hyperextension and distraction
- Bilateral pars fractures occur
- Spinal cord transection at C2 level
- Death from respiratory arrest (phrenic nerve C3-5)
Modern Hangman's fractures differ - lower energy, variable mechanisms, rarely cause death.
The low neurological injury rate (approximately 6%) in Hangman's fractures is explained by the "auto-decompression" effect - the bilateral pars fractures allow the spinal canal to expand rather than compress. This is in contrast to burst fractures where bone retropulses into the canal.
Pathophysiology and Mechanisms

C2 Vertebral Anatomy
The axis (C2) has unique anatomy:
- Description
- Superior projection articulating with C1
- Clinical Relevance
- Fractures classified separately (Anderson-D'Alonzo)
- Description
- Connects superior and inferior articular processes
- Clinical Relevance
- Site of Hangman's fracture - thin isthmus
- Description
- Large, flat, face superolateral
- Clinical Relevance
- Articulate with C1 lateral masses
- Description
- Face anteroinferior
- Clinical Relevance
- Articulate with C3 - can dislocate in Type III
- Description
- Courses through transverse foramen
- Clinical Relevance
- At risk with displaced fractures
- Description
- Large, bears weight from above
- Clinical Relevance
- Translates forward with bilateral pars fracture
Biomechanics of Injury
Classic Mechanism (Types I, II, III) - Hyperextension + Axial Load:
- Forehead strikes dashboard or object
- Neck forced into hyperextension
- Axial load transmitted through cervical spine
- Pars interarticularis fractures bilaterally (weakest point)
- Variable translation of C2 body on C3
Type IIA Mechanism - Flexion-Distraction:
- Different mechanism - flexion injury
- Distraction forces rather than compression
- Minimal translation but severe angulation
- Disc disruption between C2-C3
- CRITICAL: Traction contraindicated
Classification Systems
Levine-Edwards Classification
The most widely used classification system, based on mechanism and radiographic parameters:
- Translation
- Less than 3mm
- Angulation
- Minimal
- Mechanism
- Axial load + extension
- C2-C3 Disc
- Intact
- Translation
- Greater than 3mm
- Angulation
- Significant
- Mechanism
- Axial load + extension then flexion
- C2-C3 Disc
- Disrupted
- Translation
- Minimal (less than 3mm)
- Angulation
- Severe (greater than 11 degrees)
- Mechanism
- Flexion-distraction
- C2-C3 Disc
- Disrupted
- Translation
- Variable
- Angulation
- Variable
- Mechanism
- Flexion-compression
- C2-C3 Disc
- Disrupted + facet dislocation
- Less than 3mm translation
- Minimal angulation
- C2-C3 disc intact
- Stable fracture pattern
- Posterior longitudinal ligament intact
- Rigid cervical collar (Philadelphia, Miami J)
- 8-12 weeks immobilization
- Near 100% union rate
- Excellent prognosis
- No need for halo
Type IIA recognition: Look for "angulation out of proportion to translation" - if you see greater than 11 degrees angulation with less than 3mm translation, this is Type IIA. The mechanism is flexion-distraction, and traction will make it worse by further opening the posterior disc.
Radiographic Examples

Clinical Assessment
History
Key mechanism features:
- MVA: Dashboard injury, forehead strike
- Fall: Onto head or face (hyperextension)
- Diving: Impact with head
- Sports: Contact sports, gymnastics
- Type IIA clue: Flexion mechanism history
Associated symptoms:
- Neck pain (posterior, radiating to occiput)
- Limited range of motion
- Headache
- Neurological symptoms (rare - 6%)
Physical Examination
Maintain cervical spine immobilization until cleared. High association with other cervical and head injuries in MVA patients. Complete ATLS primary survey before focused spine examination.
Examination findings:
- Inspection: Cervical collar in place, facial/forehead trauma
- Palpation: Posterior midline tenderness at C2 level
- Neurological: Full motor/sensory exam (usually normal)
- Associated injuries: Head trauma, facial fractures common
Red Flags for Neurological Injury
Though rare, neurological injury can occur:
- Complete cord injury from judicial hanging mechanism
- Type III with cord compression
- Associated injuries (disc herniation, facet locking)
- Vertebral artery injury
Differential Diagnosis
A C2 ring lucency on imaging is not always a classic hangman's fracture; the distinction changes management and neurological risk.
- Key Distinguishing Feature
- Bilateral pars interarticularis fracture, body translates anteriorly
- Canal Effect
- Canal widens (auto-decompression)
- Management Difference
- Levine-Edwards directed (collar/halo/surgery)
- Key Distinguishing Feature
- Fracture through posterior vertebral body with cortical/pedicle continuity
- Canal Effect
- Canal NARROWS (33% paralysis - Starr & Eismont, PMID 8272942)
- Management Difference
- Higher surgical/neurological vigilance, CTA
- Key Distinguishing Feature
- Fracture line at the dens, not the pars
- Canal Effect
- Variable
- Management Difference
- Anderson-D'Alonzo classification; often anterior screw or fusion
- Key Distinguishing Feature
- Smooth, corticated, bilateral, symmetric line in a child
- Canal Effect
- None
- Management Difference
- Normal variant - no immobilisation needed
- Key Distinguishing Feature
- Corticated, non-traumatic defect, no soft-tissue swelling
- Canal Effect
- None
- Management Difference
- Incidental; no acute treatment
- Key Distinguishing Feature
- Bilateral pars fracture PLUS dislocated C2-C3 facets
- Canal Effect
- May compress cord
- Management Difference
- Reduction and surgical fusion
A separate C2 fracture that the differential above omits, and a classic exam trap, is the extension teardrop fracture of C2:
- What it is: a hyperextension avulsion of the antero-inferior corner of the C2 body by the anterior longitudinal ligament / annulus - a small triangular "teardrop" fragment at the front of C2. It is typically seen in older patients after a hyperextension fall (often striking the chin/forehead), the opposite mechanism context to a flexion teardrop.
- Why it matters - it is usually STABLE: it is a bony ALL avulsion of the anterior column only, with the posterior elements and pars intact - so it is generally a stable injury treated in a collar, unlike a hangman's (bilateral pars) fracture or the dreaded subaxial flexion teardrop.
- Don't confuse the two teardrops: the flexion teardrop fracture (classically lower cervical, e.g. C5, from flexion-compression) is a highly unstable, three-column injury with a high rate of cord injury (anterior cord syndrome) - the polar opposite in stability and prognosis to the extension teardrop of C2.
- Clues to stability: a small avulsed fragment wider than it is tall, no/minimal C2-C3 translation, intact pars and posterior elements, and no posterior ligamentous injury on MRI point to the benign extension teardrop; significant translation, posterior injury, or a tall fragment with retropulsion should raise concern for an unstable pattern.
Exam point: an anteroinferior C2 corner avulsion in an elderly hyperextension injury is usually a stable extension teardrop (collar) - distinguish it from the bilateral-pars hangman's fracture and from the unstable subaxial flexion teardrop.
Imaging
Plain Radiographs
Lateral Cervical Radiograph:
- Critical view for Hangman's fracture diagnosis
- Measure translation of C2 on C3
- Measure angulation at C2-C3
- Assess prevertebral soft tissue swelling
- Look for associated injuries
Key Measurements:
- Translation: measure C2 body posterior margin to C3
- Angulation: angle between C2 inferior endplate and C3 superior endplate
- Type I: less than 3mm translation, minimal angulation
- Type II: greater than 3mm translation, variable angulation
- Type IIA: less than 3mm translation, greater than 11 degrees angulation
CT Imaging
- Bilateral pars fractures
- Fracture pattern and comminution
- Translation measurement (more accurate)
- Facet alignment (Type III)
- Associated fractures (C1, C3)
- Superior fracture detail
- Multiplanar reconstructions
- 3D reconstructions helpful for planning
- Detects subtle fractures missed on radiograph
- Assess vertebral artery foramina
MRI Assessment
Indications for MRI:
- Neurological deficit
- Type II, IIA, III fractures
- Planning for surgical management
- Assessing disc and ligament integrity
- Cord evaluation
- C2-C3 Disc
- Intact
- Ligaments
- PLL intact
- Cord
- Normal
- C2-C3 Disc
- Disrupted
- Ligaments
- PLL torn
- Cord
- Usually normal
- C2-C3 Disc
- Posterior disruption
- Ligaments
- Posterior ligaments torn
- Cord
- Usually normal
- C2-C3 Disc
- Complete disruption
- Ligaments
- All ligaments torn
- Cord
- May be compressed
Imaging Pitfalls
Beware of "pseudo-Hangman's" appearance in children - synchondroses at C2 can mimic fracture lines. Synchondroses have smooth, corticated edges and are bilateral and symmetric. True fractures have irregular, non-corticated edges.
Management Algorithm
Rigid Cervical Collar:
- Philadelphia, Miami J, or Aspen collar
- Duration: 8-12 weeks
- Follow-up radiographs at 2, 6, 12 weeks
- Flexion-extension views at 12 weeks to confirm stability
- Near 100% union rate
Prognosis: Excellent outcomes with full return to function expected and minimal long-term sequelae.
Special Considerations
Elderly Patients:
- Higher fall mechanism
- May have osteoporosis
- Halo complications higher (pin loosening, infection)
- Consider collar for stable patterns
- Lower threshold for surgery if unstable
Associated Injuries:
- Head trauma common (forehead impact)
- Facial fractures
- Other cervical fractures (C1 Jefferson, C3)
- Assess entire cervical spine with CT
Surgical Technique
Indication: Type III, failed non-operative management, irreducible Type II
Technique:
- Patient supine, slight neck extension
- Standard Smith-Robinson right-sided approach
- Identify C2-C3 level with fluoroscopy
- Complete discectomy and endplate preparation
- Interbody graft or cage placement (PEEK or allograft)
- Anterior plate fixation with screws into C2 and C3 bodies
- Avoid extending plate above C2-C3 (adjacent segment issues)
- Intraoperative fluoroscopy confirmation
Key Points: Direct access to disrupted disc, anterior column support, high fusion rates (greater than 90%), may need posterior supplementation for severe instability.
Anterior C2-C3 ACDF is the most common surgical approach for Hangman's fracture requiring surgery. It provides direct access to the disrupted disc, allows anterior column support, and achieves high fusion rates. Posterior fixation may be added for severe instability or Type III injuries.
The "C2 pars screw (controversial)" tab above is the direct osteosynthesis technique - worth knowing by name and rationale because it is the most motion-preserving operative option for a hangman's fracture:
- The technique (Judet, later Roy-Camille/Leconte): a lag screw is placed directly across each pars/pedicle fracture, from a posterior entry on the inferior articular process of C2 directed up the pedicle - reducing and compressing the C2 ring back together.
- Why it is attractive: it fixes only the fractured bone and fuses nothing - so it preserves both the C1-C2 (rotation) and the C2-C3 motion segments, unlike an anterior C2-C3 ACDF or a posterior C2-C3 fusion which sacrifice the C2-C3 segment. This is the key examinable advantage.
- Indications/limits: best for a reducible Type II with adequate bone stock and a fracture configuration that a screw can cross; it is not suitable for Type III (facet dislocation) or grossly comminuted/irreducible patterns, and it demands a safe pedicle (a high-riding vertebral artery or narrow C2 pedicle on CT can preclude it, exactly as for odontoid C2 screws).
- Trade-off: technically demanding with a real hardware-failure risk if reduction or bone quality is poor - hence many surgeons still default to fusion for predictable union, reserving direct osteosynthesis for the younger patient in whom preserving motion is worthwhile.
Exam point: direct C2 pars (Judet) osteosynthesis is the motion-sparing operative choice for a reducible Type II hangman's fracture - it repairs the ring without fusing C2-C3, but needs a safe pedicle (check the vertebral artery on CT) and is unsuitable for Type III.
Complications
Overview
Hangman's fractures have relatively low complication rates compared to other cervical spine injuries, primarily due to the "auto-decompression" effect. However, specific complications can occur based on fracture type and treatment method.
- Incidence
- 5-10%
- Risk Factors
- Type II/III, inadequate immobilization
- Management
- Extended immobilization or surgery
- Incidence
- Variable
- Risk Factors
- Type IIA in flexion, poor reduction
- Management
- May be asymptomatic or require surgery
- Incidence
- Rare (less than 5%)
- Risk Factors
- Displaced fracture through foramen
- Management
- CTA screening, observation
- Incidence
- Very rare (less than 2%)
- Risk Factors
- Type III, cord compression
- Management
- Urgent surgical decompression
- Incidence
- 10-30%
- Risk Factors
- Elderly, osteoporosis, poor compliance
- Management
- Pin care, early removal, convert to collar
Non-union
Incidence: 5-10% overall (higher in Type II/III, rare in Type I)
Risk Factors:
- Inadequate immobilization duration
- Poor patient compliance
- Smoking and diabetes
- Severe initial displacement
Management:
- Asymptomatic: observation
- Symptomatic: C2-C3 fusion (anterior or posterior)
Malunion
Patterns: Kyphotic deformity, residual translation, Type IIA treated in flexion
Management:
- Conservative if asymptomatic
- Corrective osteotomy and fusion if severe
Vertebral Artery Injury
Incidence: Rare (less than 5%), usually asymptomatic
Diagnosis: CTA cervical spine for high-energy injuries
Management: Observation, antiplatelet therapy, rarely endovascular intervention
Neurological Complications
Incidence: Overall 6%, highest in Type III (10-15%)
Pattern: Usually present at time of injury, delayed deterioration very rare
Management: Maintain alignment, surgical decompression if indicated
Halo Vest Complications
Incidence: 10-30%, higher in elderly
Types:
- Pin site infections (10-20%)
- Pin loosening (5-15%)
- Respiratory complications
- Skin breakdown
- Dysphagia
Management: Pin care, early recognition, may require early halo removal
Postoperative Care
Immediate Postoperative Period
Day 0-3:
- ICU or high-dependency monitoring if neurologically intact
- Cervical collar or halo vest immobilization
- Neurological checks every 2-4 hours
- Pain management (multimodal analgesia)
- DVT prophylaxis (mechanical and chemical)
- Early mobilization when stable
Immobilization Protocol
After Fusion Surgery:
- Hard cervical collar for 6-8 weeks (anterior fusion alone)
- Halo vest for 8-12 weeks (posterior fusion or combined)
- Serial radiographs at 2, 6, 12 weeks
- CT at 12 weeks to assess fusion
After Non-operative Treatment:
- Collar: 8-12 weeks for Type I
- Halo: 8-12 weeks for Type II/IIA
- Flexion-extension radiographs at 12 weeks
Follow-up Schedule
- Assessment
- Wound check, neurology
- Imaging
- Lateral radiograph
- Activity
- Collar/halo wear
- Assessment
- Pain, ROM assessment
- Imaging
- AP + Lateral radiographs
- Activity
- Light activities only
- Assessment
- Fusion assessment
- Imaging
- CT + flexion-extension
- Activity
- Wean immobilization
- Assessment
- Final fusion check
- Imaging
- CT if non-union concern
- Activity
- Return to full activity
- Assessment
- Discharge if healed
- Imaging
- Only if symptomatic
- Activity
- No restrictions
Rehabilitation
Phase 1 (0-6 weeks):
- Maintain immobilization
- Upper extremity exercises (shoulder, elbow)
- Core strengthening (no neck movement)
- Gait training with collar/halo
Phase 2 (6-12 weeks):
- Gradual collar/halo weaning
- Gentle active ROM exercises
- Progressive strengthening
- Proprioceptive training
Phase 3 (3-6 months):
- Full ROM restoration
- Advanced strengthening
- Sport-specific training (if appropriate)
- Return to work assessment
Return to Activity Guidelines
- Type I
- When comfortable in collar
- Type II/IIA
- When comfortable in halo
- Type III (Surgical)
- 6-8 weeks post-surgery
- Type I
- After collar weaned, full ROM
- Type II/IIA
- After halo removed, ROM restored
- Type III (Surgical)
- 3 months post-surgery minimum
- Type I
- 3 months, confirmed union
- Type II/IIA
- 4-6 months, confirmed union
- Type III (Surgical)
- 6 months post-fusion
- Type I
- 6 months if union confirmed
- Type II/IIA
- Case-by-case, often restricted
- Type III (Surgical)
- Generally not recommended
- Type I
- Patient decision after counseling
- Type II/IIA
- Counsel on risk
- Type III (Surgical)
- Not recommended
Outcomes and Prognosis
Overall Outcomes
Hangman's fractures have generally excellent outcomes when appropriately treated:
Type I:
- Near 100% union rate with collar
- Full return to function expected
- Minimal long-term neck pain (less than 10%)
- Excellent prognosis
Type II:
- 90-95% union rate with halo
- Good functional outcomes
- Some patients have mild chronic neck pain (20-30%)
- Non-union rate 5-10% (may require late surgery)
Type IIA:
- Good outcomes if recognized and treated correctly
- Key is avoiding traction
- Union rates similar to Type II with correct management
- May have more neck stiffness than Type I
Type III:
- Variable outcomes
- Highest rate of neurological injury (10-15%)
- Surgery usually achieves stable fusion (greater than 85%)
- Loss of C2-C3 motion segment
- May have persistent neck pain (30-40%)
Functional Outcomes
- Type I
- Greater than 95%
- Type II/IIA
- 90-95%
- Type III
- 85-90% (surgical)
- Type I
- 95% full duty
- Type II/IIA
- 85% full duty
- Type III
- 70% full duty
- Type I
- Less than 10%
- Type II/IIA
- 20-30%
- Type III
- 30-40%
- Type I
- Minimal
- Type II/IIA
- 10-20 degrees
- Type III
- Complete (if fused)
- Type I
- Excellent (90%)
- Type II/IIA
- Good (80%)
- Type III
- Fair-Good (70%)
Predictors of Poor Outcomes
Factors associated with worse long-term outcomes:
- Type III injuries (highest complication rate)
- Elderly patients (greater than 65 years)
- Neurological injury at presentation
- Delayed diagnosis or treatment
- Non-compliance with immobilization protocol
- High-energy mechanism
- Smoking and comorbidities
Guidelines, Registries & Global Practice
Global Epidemiology
- Traumatic spondylolisthesis of the axis ("hangman's fracture") accounts for approximately 4-7% of all cervical spine fractures and is the second most common axis fracture after the odontoid (Francis et al., J Bone Joint Surg Br 1981, PMID 7263740; Cai et al., Emerg Radiol 2022, PMID 35543854).
- Bimodal age distribution: high-energy motor vehicle collisions in younger adults and low-energy falls in older adults. Recent level-1 trauma-centre data report a mean age of 62.7 years, reflecting an ageing injured population (Cai et al., 2022, PMID 35543854).
- Neurological injury is uncommon (historically approximately 6%) because the bilateral pars fracture tends to decompress rather than narrow the canal; the main exceptions are Type III, atypical posterior-body fractures, and high-energy distraction (Starr & Eismont, Spine 1993, PMID 8272942).
Guideline & Classification Comparison
- Framework
- Evidence-based US spine-trauma guideline
- Core Guidance
- External immobilisation initially for most; surgery for severe C2-C3 angulation, disc disruption, or failure to maintain alignment
- Evidence Level
- Practice option (insufficient evidence for a standard)
- Framework
- Mechanistic 4-type classification
- Core Guidance
- I collar; II reduce then halo; IIA halo in extension (NO traction); III surgery
- Evidence Level
- Level IV defining series
- Framework
- Displacement-and-stability grading
- Core Guidance
- Stable/undisplaced - external brace; displaced or facet dislocation - consider surgery
- Evidence Level
- Level IV
- Framework
- Morphology + facet + modifiers
- Core Guidance
- Escalate to fixation with disco-ligamentous disruption or dislocation
- Evidence Level
- Expert consensus
Registry & Synthesised Evidence
- The largest systematic review (25 studies, 548 fractures) found non-operative union of 94.1% versus 99.4% surgically, with no mortality difference and both anterior and posterior approaches achieving high fusion (Murphy et al., J Orthop Trauma 2017, PMID 28816880).
- For low-grade fractures, a rigid collar matched halo immobilisation for union, with no demonstrable advantage of the halo and lower morbidity - particularly relevant for older patients (Al-Mahfoudh et al., Global Spine J 2015, PMID 27099816).
- There are no national hangman's-fracture–specific arthroplasty/registry datasets (unlike joint replacement); evidence is dominated by retrospective series and pooled reviews, so guidance remains at the level of practice options rather than standards (Hadley et al., 2002, PMID 12431297).
Practice Variation
- Immobilisation device: Halo use has declined in many high-income centres in favour of rigid collars for stable patterns, driven by halo morbidity (pin-site infection, loosening, pneumonia) especially in the elderly.
- Operative threshold: Surgeons increasingly favour early fixation for Type II with marked translation/angulation and for Type III, citing higher union and faster mobilisation; halo-based non-operative care remains standard for Type I and many Type II/IIA fractures.
- Vascular screening: High-grade fractures (Type IIA/III) warrant CT angiography for blunt cerebrovascular injury and brain imaging, given the markedly higher rates of vertebral artery injury and traumatic brain injury (Cai et al., 2022, PMID 35543854).
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old male is in an MVA. Lateral cervical radiograph shows a bilateral C2 pars fracture with 5mm translation and 8 degrees angulation. What is your classification and management?”
“A Hangman's fracture is identified with 2mm translation but 15 degrees of angulation. What type is this and how would you manage it differently?”
“Explain why neurological injury is rare in Hangman's fractures despite the unstable nature of the injury.”
MCQ Practice Points
High-Yield Facts for MCQs
Classification:
- Type I: less than 3mm translation, minimal angulation, collar treatment
- Type II: greater than 3mm translation, significant angulation, halo treatment
- Type IIA: minimal translation (less than 3mm) but severe angulation (greater than 11 degrees), NO TRACTION
- Type III: facet dislocation, surgical treatment
Q: How are Type I, II, and IIA distinguished by measurement? A: The Levine-Edwards classification uses 3mm translation and 11 degrees angulation thresholds. Type I is less than 3mm translation. Type II is greater than 3mm translation. Type IIA is less than 3mm translation but greater than 11 degrees angulation.
Key Measurements:
- 3mm: threshold between Type I and Type II translation
- 11 degrees: threshold for Type IIA angulation
- 8-12 weeks: typical immobilization duration
Q: What is the classic exam trap regarding Type IIA fractures? A: Type IIA is a FLEXION-DISTRACTION injury (unlike others). Traction is CONTRAINDICATED as it worsens displacement. Treatment is halo in extension.
Mechanism:
- Type I, II, III: hyperextension with axial loading
- Type IIA: flexion-distraction (opposite mechanism)
- Judicial hanging: hyperextension + distraction (usually fatal)
Neurological Injury:
- Overall rate: approximately 6%
- Explained by "auto-decompression" - canal expands
- Type III has highest risk
- Bilateral pars fractures allow posterior elements to separate
Q: Why is neurological injury rare (6%) in Hangman's fractures? A: "Auto-decompression" - the bilateral pars fractures allow the posterior elements to separate from the anterior body, expanding the spinal canal diameter rather than narrowing it.
Type IIA Critical Points:
- TRACTION IS CONTRAINDICATED
- Halo applied in EXTENSION position
- Flexion-distraction mechanism
- Angulation out of proportion to translation
- Most commonly tested pitfall in exams
Surgical Indications:
- Type III (facet dislocation)
- Failed non-operative management
- Irreducible Type II
- Patient unable to tolerate halo
- Non-union after appropriate immobilization
Q: Which Hangman's fracture requires surgical stabilization? A: Type III (with facet dislocation). It is highly unstable. Type I and II are usually managed with collar or halo respectively.
Imaging:
- Lateral cervical radiograph: key view
- Measure both translation AND angulation
- CT: fracture pattern, facet alignment
- MRI: disc disruption, cord, ligaments
Q: What specific measurements must be taken on lateral X-ray? A: Both translation AND angulation. Measuring only translation will miss Type IIA (minimal translation, severe angulation).
Common Exam Traps
- Type IIA traction: Most common mistake - traction worsens injury
- Neurological injury rate: Not high despite "unstable" fracture
- Measurement confusion: Must measure BOTH translation and angulation
- Mechanism confusion: Type IIA is flexion, not extension
- Surgical timing: Type III needs surgery, not all Hangman's fractures
- Collar vs halo: Type I gets collar, Type II gets halo
- Union rates: Generally excellent with appropriate treatment
MCQ Stems to Expect
- "A patient has C2 pars fracture with 2mm translation and 15-degree angulation. What is the classification and management?"
- "What explains the low neurological injury rate in Hangman's fractures?"
- "What is contraindicated in Type IIA Hangman's fracture?"
- "A Type III Hangman's fracture is characterized by..."
- "What is the most appropriate initial immobilization for a Type II Hangman's fracture?"
At a Glance Table
- Type I
- Less than 3mm
- Type II
- Greater than 3mm
- Type IIA
- Less than 3mm
- Type III
- Variable
- Type I
- Minimal
- Type II
- Significant
- Type IIA
- Severe (greater than 11°)
- Type III
- Variable
- Type I
- Extension + axial load
- Type II
- Extension then flexion
- Type IIA
- Flexion-distraction
- Type III
- Flexion-compression
- Type I
- Intact
- Type II
- Disrupted
- Type IIA
- Posterior disruption
- Type III
- Complete disruption
- Type I
- Stable
- Type II
- Unstable
- Type IIA
- Unstable
- Type III
- Very unstable
- Type I
- Rigid collar 8-12 weeks
- Type II
- Halo vest 8-12 weeks
- Type IIA
- Halo in EXTENSION (NO traction)
- Type III
- Surgery - fusion
- Type I
- Near 100%
- Type II
- 90-95%
- Type IIA
- High with correct treatment
- Type III
- Variable post-surgery
- Type I
- Most common type
- Type II
- May use traction initially
- Type IIA
- TRACTION CONTRAINDICATED
- Type III
- Facet dislocation present
HANGMAN
Hook:HANGMAN helps remember Hangman's fracture assessment and the critical Type IIA warning
TYPES
Hook:TYPES helps remember Levine-Edwards management - especially that Type IIA prohibits traction
ASSESS
Hook:ASSESS the Hangman's fracture patient systematically
COLLAR
Hook:COLLAR or halo - management depends on type, with special rules for IIA and III
Exam Cheat Sheet
Classification
- Type I: less than 3mm translation, minimal angulation = COLLAR
- Type II: greater than 3mm translation, angulation = HALO
- Type IIA: less than 3mm translation BUT greater than 11 degrees angulation = HALO IN EXTENSION, NO TRACTION!
- Type III: facet dislocation → SURGERY
Key Concepts
- Bilateral C2 pars fracture (traumatic spondylolisthesis)
- Neurological injury rare (6%) - canal expands (auto-decompression)
- Type IIA is flexion-distraction - traction worsens injury
- Measure translation AND angulation on lateral cervical radiograph
Critical Pitfalls
- Applying traction to Type IIA (CONTRAINDICATED)
- Missing Type IIA - look for angulation greater than translation
- Treating Type III non-operatively (needs surgery)
- Missing associated C1 or C3 fractures
Exam Tips
- Type IIA recognition is the classic exam trap
- minimal translation + severe angulation = Type IIA
- Explain auto-decompression for why cord spared
- Know surgical options for Type III
Evidence and Guidelines
Levine-Edwards Classification (defining series)
- 52 patients with traumatic spondylolisthesis of the axis (15 Type I, 29 Type II, 3 Type IIA, 5 Type III). Associated neurological deficit in only 4 patients. All fractures healed.
- Type IIA injuries showed INCREASED displacement when placed in traction and were reduced instead with gentle extension and compression in a halo vest - the origin of the 'no traction' rule.
- Fracture type correlated with mechanism: Type I hyperextension-axial loading; Type II hyperextension-axial loading then severe flexion; Type IIA flexion-distraction; Type III flexion-compression.
Francis Grading & Non-operative Outcomes
- Series of 123 patients with traumatic spondylolisthesis of the axis. High incidence of associated face/scalp injuries and upper cervical fractures, but LOW incidence of neurological injury despite apparent gross instability.
- Union was usual regardless of displacement; protection from extremes of flexion and extension was adequate treatment. Early mobilisation in a halo reduced hospital stay without jeopardising the result.
- Surgery (anterior C2-C3 interbody fusion to preserve atlanto-axial rotation) needed only for chronic instability with or without pain.
Atypical Hangman's Fractures (canal-narrowing pattern)
- 19 cases of traumatic spondylolisthesis: 13 standard hangman's fractures and 6 'atypical' fractures running through the posterior vertebral body with unilateral/bilateral continuity of the posterior cortex or pedicle.
- Unlike standard fractures, the atypical pattern NARROWS the spinal canal and was associated with paralysis in 33% - far more than previously anticipated.
- These atypical C2 injuries must be recognised as distinct from Levine-Edwards/Effendi types because of their greater neurological risk.
Effendi Classification (axis ring fractures)
- Retrospective analysis of 131 fractures of the ring of the axis, classified into three types by radiological displacement and stability (Type I undisplaced/stable; Type II displaced with abnormal C2-C3 disc; Type III displaced with C2-C3 facet dislocation).
- Provided the original three-type scheme later modified by Levine and Edwards (who added Type IIA) and refined by Francis (I-V grading).
Surgical vs Non-operative Treatment - Systematic Review
- Pooled union rate was 94.1% for 131 non-surgically treated fractures versus 99.4% for 417 surgically treated fractures; non-union was less likely with surgery (OR 0.12, 95% CI 0.02-0.71).
- No significant difference in mortality between surgical (0.16%) and non-surgical (1.04%) groups; treatment failure was lower in the surgical group.
- Both anterior and posterior approaches achieved high fusion rates with neither clearly superior.
Collar vs Halo for Low-Grade Fractures
- 41 hangman's fractures (mean age 59) from 105 axis fractures; 31.7% typical and 68.2% atypical. Most were low-grade (Type I/II).
- Bony union was achieved in ALL patients; there was NO difference in outcome between rigid collar and halo immobilisation for low-grade fractures, and only 7.3% needed surgery.
- Permanent neurological deficit occurred in just one patient (from associated injuries).
Modern Epidemiology & Vascular/Brain Injury Risk
- Traumatic spondylolisthesis of the axis accounts for 4-5% of all cervical fractures; mean age 62.7 years, motor vehicle collision the commonest cause at this level-1 trauma centre.
- Type I injuries healed well with conservative management, while Type IIA and III were significantly more likely to be managed surgically.
- Type IIA and III injuries carried significantly higher-grade vertebral artery injuries (Biffl III-IV) and an 11-fold increased risk of traumatic brain injury versus Type I/II - mandating CT angiography and TBI screening.