Herring Lateral Pillar Classification of Perthes
The Herring lateral pillar classification (also called the lateral pillar classification of Herring) is applied to the AP radiograph of the pelvis during the fragmentation stage of Perthes disease. It grades the lateral pillar (the lateral third of the epiphysis) by height preservation: A = no collapse, B = at least 50 percent preserved, B-C border = very narrow or exactly 50 percent, C = less than 50 percent or absent. Examiners expect you to classify a case from an AP radiograph, state the prognosis by age group, and explain how it guides containment decisions. Do not confuse it with Catterall (which assesses the whole head involvement in four groups) — Herring is more reproducible and prognostically superior.
The lateral pillar is the last part of the epiphysis to collapse in Perthes disease because it receives the most robust residual blood supply from the lateral circumflex artery anastomoses. This is why its preservation correlates so strongly with a good outcome — an intact lateral pillar mechanically supports the central and medial segments during reossification.
The classification assumes the disease; the examiner will ask you to frame it:
- Definition — idiopathic osteonecrosis (avascular necrosis) of the femoral capital epiphysis in a child, from interruption of its precarious blood supply (predominantly the medial femoral circumflex artery via the lateral epiphyseal/retinacular vessels), followed by revascularisation, structural weakening and repair.
- Epidemiology — boys about 4–5 times more often than girls; peak onset 4–8 years (range ~2–14); bilateral in roughly 10–15% but ASYNCHRONOUS / at different stages — simultaneous, same-stage bilateral disease should prompt a search for a skeletal dysplasia or other cause; associations include short stature/delayed bone age, low birth weight and passive smoking.
- Presentation — an insidious, often painless limp with intermittent groin/thigh or referred knee pain (obturator nerve), loss of hip abduction and internal rotation, a possible Trendelenburg gait and thigh atrophy; the child is well and afebrile (distinguishing it from septic arthritis).
- Waldenström radiographic stages — (1) initial/necrotic (a smaller, denser, sclerotic epiphysis, widened joint space, possible subchondral crescent), (2) fragmentation (the stage in which the Herring grade is assigned), (3) reossification/healing, (4) remodelled/residual.
- Bilateral-symmetric differential — multiple epiphyseal dysplasia, spondyloepiphyseal dysplasia, hypothyroidism, sickle cell disease, Gaucher disease and steroid-induced avascular necrosis.
The Herring Lateral Pillar Classification
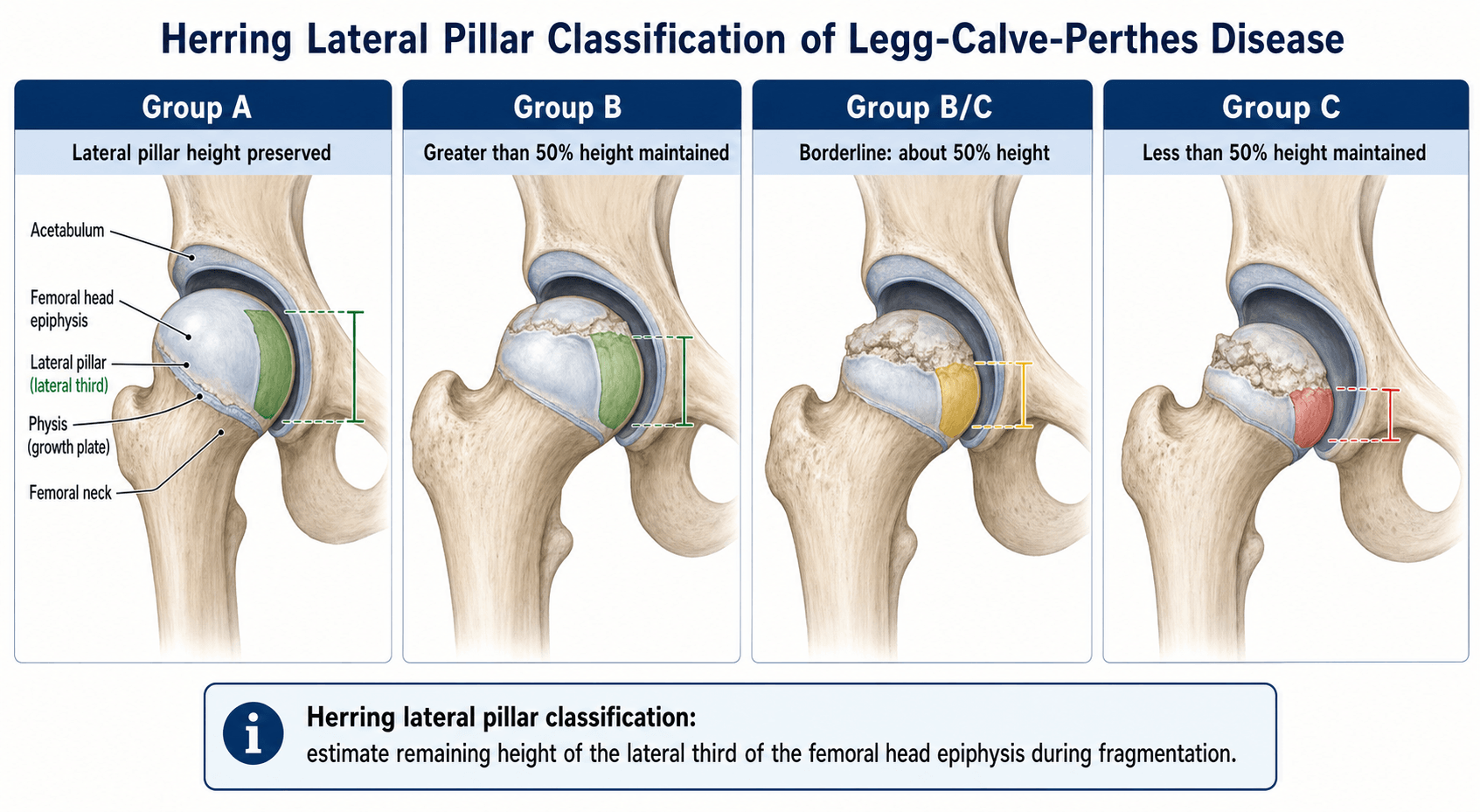

The classification is based on the height of the lateral pillar (the lateral one-third of the femoral capital epiphysis) on a true anteroposterior pelvic radiograph taken during the fragmentation stage of Legg-Calvé-Perthes disease.
- Lateral Pillar Height
- No loss of height; lateral pillar fully preserved
- Prognosis (Stulberg I/II)
- Excellent — near-universal Stulberg I or II
- Typical Management
- Observation; no containment needed
- Lateral Pillar Height
- At least 50 percent of original lateral pillar height maintained
- Prognosis (Stulberg I/II)
- Good if under age 6; guarded if over age 8
- Typical Management
- Observation under 6; consider containment over 8
- Lateral Pillar Height
- Very narrow lateral pillar (less than 50 percent but not fully collapsed), or exactly 50 percent with lateral calcification or Gage sign
- Prognosis (Stulberg I/II)
- Intermediate — outcome between B and C
- Typical Management
- Treat as B or C based on age and clinical factors; usually manage as C
- Lateral Pillar Height
- Less than 50 percent of original height, or complete collapse of the lateral pillar
- Prognosis (Stulberg I/II)
- Poor — high risk of Stulberg III, IV, or V
- Typical Management
- Early containment (osteotomy); consider older surgical options
A · B · B-C · CThe lateral pillar groups — A, B, B-C, C
Hook:A-B-C is a height ladder for the lateral third of the epiphysis; the lower the pillar, the worse the outcome.
Fragment — Fix — FollowWhen to apply the classification
Hook:The group is a moving target during fragmentation — re-grade on every serial film before committing to treatment.
Gage sign — a radiolucent V-shaped defect in the lateral epiphysis — is an early sign of Perthes that may accompany lateral pillar involvement. It does not define the Herring group but supports the diagnosis when seen alongside pillar changes.
Lateral Pillar versus Other Perthes Classifications
Several classification systems exist for Perthes disease. The Herring lateral pillar system has largely superseded earlier systems in clinical practice because of its superior inter-observer reliability and prognostic accuracy.
- What It Assesses
- Height of lateral pillar on AP in fragmentation phase
- Number of Groups
- 4 (A, B, B-C, C)
- Key Strength
- Best reproducibility and prognostic accuracy; validated multi-centre
- Key Limitation
- Must be applied during fragmentation phase only
- What It Assesses
- Extent of head involvement (all three pillars) on AP and lateral
- Number of Groups
- 4 (Groups I–IV)
- Key Strength
- First widely used classification; intuitive anatomical concept
- Key Limitation
- Moderate inter-observer reliability; less prognostically accurate than Herring
- What It Assesses
- Width of radiolucent crescent (subchondral fracture line) on early films
- Number of Groups
- 2 (A = less than half, B = more than half)
- Key Strength
- Simple; can be applied very early in disease
- Key Limitation
- Crescent sign often not visible; only two groups limit granularity
- What It Assesses
- Sphericity of the healed femoral head at maturity
- Number of Groups
- 5 (I–V)
- Key Strength
- Gold-standard outcome measure; correlates with late arthritis
- Key Limitation
- Outcome measure only — cannot be used to guide acute treatment
Pillar Predicts Prognosis PreciselyWhy lateral pillar is the exam favourite
Hook:Four P's: the Pillar Predicts Prognosis Precisely.
Two adjuncts the examiner expects you to define, not just name:
- Catterall "head-at-risk" signs (markers of a poorer prognosis that support containment): the Gage sign (a V-shaped lucency at the lateral epiphysis/metaphysis), calcification lateral to the epiphysis, lateral subluxation/extrusion of the femoral head, a horizontal physis, and metaphyseal cysts/reaction.
- Stulberg classification (sphericity and congruence at skeletal maturity — the outcome measure that predicts late arthritis): Class I a normal spherical head; Class II spherical but with coxa magna, a short neck or a steep acetabulum (I and II = "spherical congruency", good, low arthritis risk); Class III an ovoid/non-spherical (not flat) head; Class IV a flat head with a congruent flat acetabulum (III and IV = "aspherical congruency", intermediate); and Class V a flat head with a normal/incongruent acetabulum ("aspherical incongruency") — the worst, with premature osteoarthritis. The governing principle is that aspherical incongruency (V) predicts early OA, whereas congruency (I–IV) is protective — which is exactly the spherical outcome that lateral-pillar-guided containment aims to preserve.
Containment Decision-Making
The lateral pillar classification directly guides the decision to pursue containment — the principle of keeping the femoral head covered by the acetabulum during the fragmentation and reossification phases to promote spherical healing.
- Group A: No containment needed. The lateral pillar is intact and the prognosis is excellent with observation and activity modification alone.
- Group B (under age 6): Observation is reasonable. Good remodelling potential supports a non-operative approach.
- Group B (over age 8): Containment is recommended. Options include femoral varus derotational osteotomy, Salter innominate osteotomy, or a combination (shelf acetabuloplasty in selected cases). The choice depends on surgeon expertise, concomitant acetabular dysplasia, and range of motion.
- Group B-C border: Treat as C if over age 6. The risk of aspherical healing is high enough to justify intervention.
- Group C: Containment strongly recommended at any age. Even with containment, the prognosis is guarded, particularly in older children. Some surgeons advocate for more aggressive approaches including Petrie cast or broomstick cast as adjuncts.
Containment methods: Non-operative (Petrie casts, broomstick casts, abduction bracing) and operative (femoral varus derotational osteotomy, Salter innominate osteotomy, double-level osteotomy, shelf acetabuloplasty). The principle is the same: maintain femoral head coverage within the acetabulum during the vulnerable reossification phase. Operative containment is preferred in children over age 6 with lateral pillar B or worse because it provides more reliable and durable coverage.
Radiographic Technique and Pitfalls
Accurate lateral pillar classification depends on proper radiographic technique:
- True AP pelvis: The radiograph must be a true anteroposterior view of the pelvis, not a frog lateral or oblique. Internal or external rotation of the limb distorts the apparent pillar height.
- Timing during fragmentation: The classification is valid only during the fragmentation phase (typically 6 to 12 months after onset). Applying it too early (initial avascular phase) underestimates involvement; applying it too late (reossification) overestimates recovery.
- Serial radiographs: Because pillar height can change, the classification should be reassessed on sequential AP pelvic radiographs at 3 to 4-month intervals during fragmentation.
- Identify the lateral pillar correctly: The lateral pillar is the lateral one-third of the epiphysis, bordered medially by a vertical line from the junction of the middle and lateral thirds. The central and medial pillars are not assessed.
- Do not use the frog lateral for classification: The lateral pillar is assessed on the AP view only. The frog lateral is complementary for assessing head-at-risk signs and hinge abduction but does not provide the pillar measurement.
Hinge abduction is a critical concept in Perthes management. If the enlarged femoral head hinges on the lateral acetabular margin during abduction (visible on dynamic arthrogram or frog lateral), containment procedures will fail because the head cannot be reduced under the acetabular roof. Hinge abduction must be excluded before proceeding with containment surgery — an arthrogram under anaesthesia is the gold standard to assess this.
Prognosis by Age and Lateral Pillar Group

The interaction between age at onset and lateral pillar group is the critical prognostic determinant. The same lateral pillar group carries a very different prognosis in a four-year-old versus a ten-year-old.
- Under 6 years at onset
- Excellent — observe
- 6 to 8 years at onset
- Excellent — observe
- Over 8 years at onset
- Excellent — observe
- Under 6 years at onset
- Good — observe
- 6 to 8 years at onset
- Guarded — consider containment
- Over 8 years at onset
- Poor — containment recommended
- Under 6 years at onset
- Good to guarded
- 6 to 8 years at onset
- Guarded — lean toward containment
- Over 8 years at onset
- Poor — containment recommended
- Under 6 years at onset
- Guarded — consider containment
- 6 to 8 years at onset
- Poor — containment recommended
- Over 8 years at onset
- Poor — containment strongly recommended; outcome often unsatisfactory
Children over age eight at onset with lateral pillar group B or worse have a significantly increased risk of aspherical healing (Stulberg III or higher). Even with containment surgery, outcomes in this age group are less predictable. Early recognition and prompt referral to a paediatric orthopaedic surgeon are essential — the window for effective containment is during the fragmentation and early reossification phases and closes as the child approaches skeletal maturity.
Guidelines, Registries and Global Practice
- No single international guideline governs Perthes management. Treatment decisions are individualised based on age, lateral pillar group, range of motion, and surgeon preference. The evidence base consists primarily of retrospective cohort studies and expert consensus.
- POSNA (Pediatric Orthopaedic Society of North America) and EPOS (European Paediatric Orthopaedic Society) broadly endorse the lateral pillar classification as the preferred radiographic prognostic tool. Containment decisions follow the age-and-pillar framework described above.
- Global practice variation: North American surgeons more commonly use femoral varus osteotomy for containment. European surgeons, particularly in the UK and Scandinavia, more often favour Salter innominate osteotomy or non-operative containment (Petrie casts). Japanese centres have reported good results with prolonged bed rest and traction in younger children. These differences reflect training tradition rather than definitive evidence of superiority.
- The lateral pillar classification has been validated across multiple ethnic populations and healthcare settings, supporting its use as a global prognostic tool.
- Long-term follow-up to skeletal maturity is universally recommended regardless of treatment approach, because the Stulberg outcome cannot be reliably predicted before growth plate closure.
Viva practice
Exam Viva
Practise clinical reasoning and management decisions out loud
“A 7-year-old boy presents with a 4-month history of a limp and right hip pain. An AP pelvic radiograph shows Perthes disease in the fragmentation phase. The lateral pillar of the right femoral head has lost approximately 40 percent of its height. How would you classify this, what is the prognosis, and how would you manage him?”
“A 10-year-old girl presents with left hip Perthes disease. The AP radiograph in fragmentation shows complete collapse of the lateral pillar with lateral subluxation of the femoral head. She has limited abduction to 20 degrees. Classify, prognosticate, and outline your management.”
Exam cheat sheet
The four lateral pillar groups
- Group A: no lateral pillar height loss — excellent prognosis
- Group B: at least 50 percent of lateral pillar height preserved — good under 6, guarded over 8
- Group B-C border: very narrow pillar or exactly 50 percent with risk factors — treat as C
- Group C: less than 50 percent height or complete collapse — poor prognosis
Classification essentials
- Apply on true AP pelvis radiograph during the fragmentation phase only
- Assess the lateral one-third of the epiphysis (the lateral pillar)
- Age at onset and lateral pillar group together determine prognosis
- Serial radiographs at 3 to 4-month intervals — pillar height can change
Management by group and age
- Group A (any age): observe — no containment needed
- Group B under 6: observe; Group B over 8: containment surgery recommended
- Group C (any age): containment strongly recommended; prognosis still guarded
- Always exclude hinge abduction with arthrogram before containment surgery
Key distinctions for the exam
- Herring (lateral pillar) is more reproducible and prognostic than Catterall
- Containment options: femoral varus osteotomy, Salter osteotomy, or combined double-level
- Stulberg classification is the outcome measure at skeletal maturity, not a treatment guide
- The lateral pillar is the last to collapse because of robust lateral circumflex blood supply
Evidence
The lateral pillar classification of Legg-Calvé-Perthes disease
- The original paper introducing the lateral pillar classification (groups A, B, C), applied during the fragmentation stage to 93 hips (86 braced patients) followed to skeletal maturity by the Stulberg outcome.
- Group A had a uniformly good outcome (100% Stulberg I/II); group B did well if under 9 years at onset (92% Stulberg I/II) but worse if over 9; group C usually became aspherical at any age.
- Observers agreed 78% of the time, and the lateral pillar group predicted final outcome more strongly than age at onset.
Legg-Calvé-Perthes disease. Part II: prospective multicenter study of the effect of treatment on outcome
- Prospective multicentre study: 438 patients / 451 hips (age 6–12 at onset), each surgeon applying one method; 345 hips followed to skeletal maturity.
- Lateral pillar classification (p<0.0001) and age at onset (p=0.0001) were both strong independent prognostic factors.
- In children over 8 at onset, lateral pillar B and B/C-border hips did significantly better with surgery than non-operatively; group B under 8 did well regardless of treatment; group C did poorly whatever was done.
Radiographic classifications in Perthes disease
- Interobserver study of 42 patients (5 observers): original lateral pillar kappa 0.49 and Catterall kappa 0.43 (both moderate); the modified B/C-added version was only fair (kappa 0.40).
- The original lateral pillar classification was strongly associated with 5-year femoral-head sphericity (mean γ 0.75), better than the modified (0.55) or Catterall (0.64).
- Adding the borderline B/C group did not improve interobserver agreement or prognostic value over the original.
According to PubMed, the lateral pillar classification itself was introduced by Herring et al. 1992 (DOI 10.1097/01241398-199203000-00001; group A 100% Stulberg I/II, 78% observer agreement). The prognostic value of the lateral pillar group combined with age at onset — and the benefit of containment surgery for over-8s with group B/(B/C) — is from Herring, Kim & Browne 2004 (J Bone Joint Surg Am 2004;86(10):2121-34; PMID 15466720). The reliability/validity comparison showing the original lateral pillar classification best predicts 5-year sphericity (γ 0.75) is from Huhnstock et al. 2017 (DOI 10.1080/17453674.2017.1340040).