Commonest SA/OM Under 4 Years | Indolent Presentation | Blood-Culture-Bottle + PCR Diagnosis
- Gram-negative coccobacillus; oropharyngeal commensal in young children
- Commonest cause of septic arthritis and osteomyelitis in children aged 6-48 months in regions where PCR is used
- Indolent presentation: low-grade or absent fever, child may still weight-bear, modest CRP elevation
- Inoculate joint aspirate into blood culture bottles (dramatically increases yield vs standard agar)
- Real-time PCR targeting cpn60 gene is the gold-standard diagnostic test
- Uniformly susceptible to beta-lactams; excellent prognosis with appropriate antibiotics
- “Any child under 4 with septic arthritis or osteomyelitis: think Kingella kingae first
- “Lower CRP and ESR than Staph aureus: do not let normal inflammatory markers reassure you
- “Blood culture bottle inoculation of joint aspirate increases culture yield substantially
- “PCR is gold standard but not universally available: high clinical suspicion must drive treatment
- “Preceded by upper respiratory infection or oral ulcers in up to half of cases
Gram-negative coccobacillus, member of Neisseriaceae. Fastidious: requires enriched media (blood agar with hemin, chocolate agar). Oropharyngeal commensal colonizing 10-30 percent of children under 4. Hematogenous spread to bones and joints after mucosal breach (URI, stomatitis).
Peak age 6-24 months. The commonest cause of osteoarticular infection in children under 4 where PCR-based studies have been performed. Daycare attendance is a risk factor. Seasonal peaks in autumn and winter. Outbreaks reported in daycare centres.
Indolent onset over days to weeks. Low-grade or absent fever. Child may still partially weight-bear. CRP and ESR often only mildly elevated. Joint aspirate WBC often lower than classical septic arthritis threshold. Can be misdiagnosed as transient synovitis or trauma.
Inoculate joint aspirate into blood culture bottles rather than plating on agar: yield increases dramatically because the organism thrives in liquid enrichment media. Real-time PCR (cpn60 target) is the gold standard. Standard agar cultures are frequently negative.
- Diagnosis
- Joint aspirate into blood culture bottles + PCR (cpn60)
- Treatment
- IV cefazolin or ampicillin, then oral step-down
- Key Pearl
- Think Kingella first in this age group
- Diagnosis
- MRI + blood culture bottles from tissue/blood + PCR
- Treatment
- IV beta-lactam then oral, total 3-4 weeks
- Key Pearl
- Lower CRP than Staph aureus osteomyelitis
- Diagnosis
- Standard cultures negative; retest with PCR/bottles
- Treatment
- Start empiric beta-lactam if clinical suspicion high
- Key Pearl
- Indolent course means delayed diagnosis is common
KINGIdentifying Kingella kingae
Hook:KING of paediatric bone and joint infections in the under-4 age group!
Overview and Epidemiology
Kingella kingae has emerged as the commonest bacterial cause of osteoarticular infections in children under 4 years in regions where PCR-based diagnostic methods are used. Before PCR, the organism was missed because it is fastidious and difficult to culture on standard agar. Many cases previously labelled "culture-negative septic arthritis" were likely Kingella. Its indolent presentation means it is easily confused with transient synovitis, delaying diagnosis. Every orthopaedic trainee must know this organism for paediatric oral and written examinations.
- Age: Peak 6-24 months; over 80 percent of cases under 4 years
- Gender: Male preponderance (approximately 60-65 percent)
- Season: Autumn and winter peaks (correlates with respiratory illness)
- Risk factors: Daycare attendance, recent upper respiratory infection, oral ulcers or stomatitis
- Colonization: 10-30 percent of healthy children under 4 carry K. kingae in the oropharynx
- Transmission: Respiratory droplets; outbreaks in daycare centres documented
- Septic arthritis: Most common manifestation (approximately 50-65 percent of osteoarticular cases)
- Osteomyelitis: Approximately 20-30 percent; distal femur, proximal tibia, calcaneus
- Spondylodiscitis: Approximately 5-10 percent; lumbar spine predominates
- Tenosynovitis: Distinctive feature; more common with Kingella than other pathogens
- Endocarditis: Rare but serious; consider if bacteremia with cardiac murmur
Microbiology and Pathogenesis
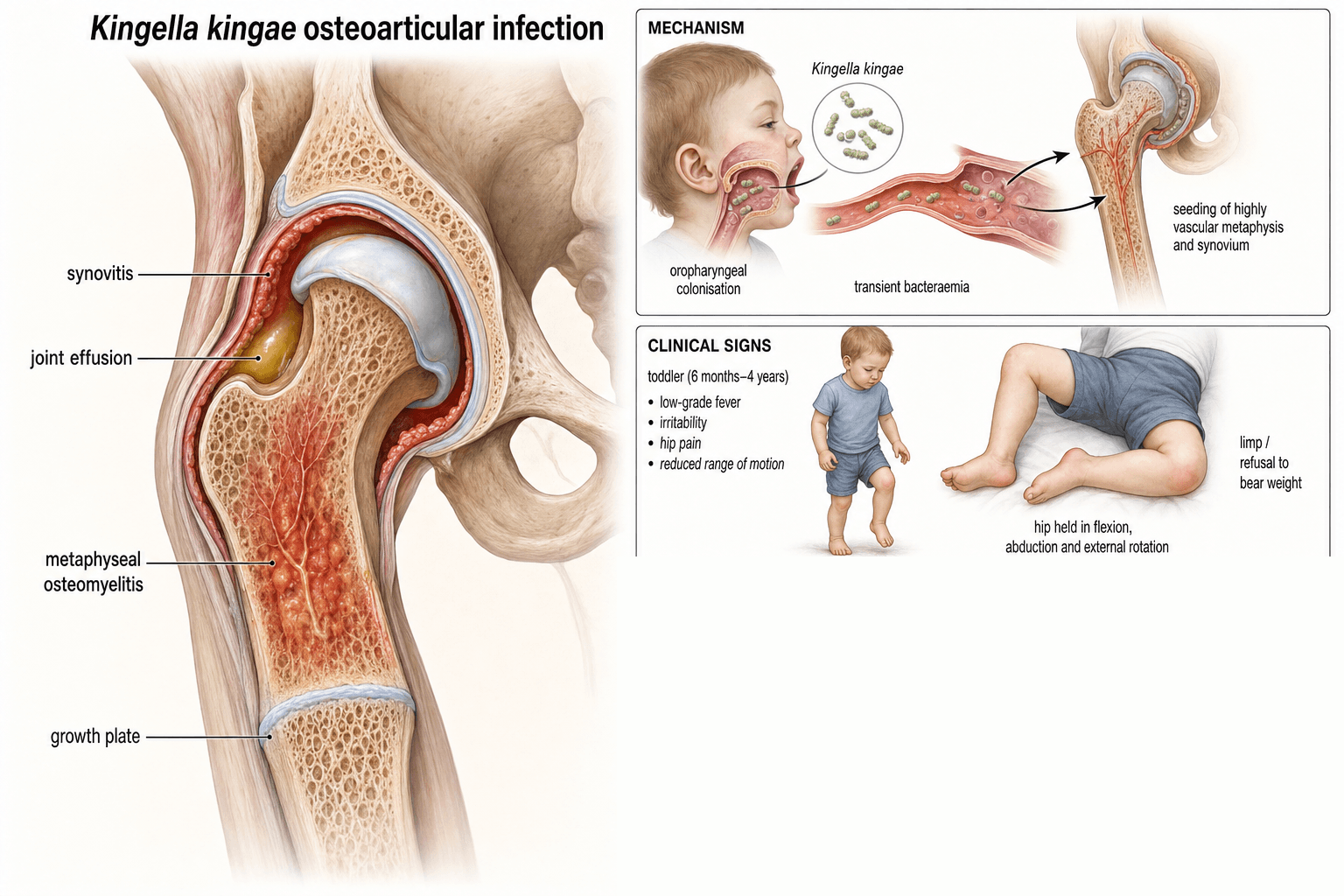
Kingella kingae is a Gram-negative coccobacillus, facultative anaerobe, member of the Neisseriaceae family. It is a fastidious organism that grows poorly on standard agar media but thrives in enriched liquid media (blood culture bottles, chocolate agar with hemin). It colonizes the oropharynx of young children and causes invasive disease when mucosal integrity is breached (by viral upper respiratory infections, oral ulceration, or teething). Transient bacteremia seeds the skeleton via hematogenous spread. The organism's affinity for synovial and osseous tissues in toddlers is well established but the precise molecular mechanisms remain under investigation.
- Kingella kingae
- 6-48 months (toddlers)
- Staphylococcus aureus
- All ages; bimodal (neonates and adolescents)
- Kingella kingae
- Indolent (days to weeks)
- Staphylococcus aureus
- Acute (hours to days)
- Kingella kingae
- Low-grade or absent
- Staphylococcus aureus
- High fever, toxic-appearing child
- Kingella kingae
- Modest elevation (CRP often under 50)
- Staphylococcus aureus
- Marked elevation (CRP often over 80)
- Kingella kingae
- May partially weight-bear
- Staphylococcus aureus
- Usually completely non-weight-bearing
- Kingella kingae
- Frequently negative (fastidious)
- Staphylococcus aureus
- Usually positive on standard media
- Kingella kingae
- Rapid (24-48 hours), excellent prognosis
- Staphylococcus aureus
- Variable; depends on abscess and MRSA status
Step 1: Oropharyngeal colonization (10-30 percent of young children)
Step 2: Mucosal breach (viral URI, stomatitis, teething)
Step 3: Transient bacteremia
Step 4: Hematogenous seeding of metaphyseal bone or synovium
Step 5: Local infection with indolent clinical course
The RTX (repeats in toxin) toxin and type IV pilus are key virulence factors that facilitate epithelial adherence and invasion.
Immune factors: Waning maternal antibodies and immature adaptive immunity in the 6-24 month window
Behavioural: Mouthing objects, frequent respiratory infections, daycare exposure
Anatomical: Rich vascular supply to growth plates creates favourable conditions for bacterial seeding
Colonization pressure: Peak oropharyngeal colonization occurs in this age group
The topic refers to Kingella as a "member of the HACEK group" - an examiner will expect you to expand the acronym and explain its significance. HACEK is a group of fastidious, slow-growing Gram-negative oropharyngeal commensals that classically cause subacute, culture-negative infective endocarditis:
- H - Haemophilus species (and Aggregatibacter aphrophilus, formerly Haemophilus aphrophilus)
- A - Aggregatibacter actinomycetemcomitans
- C - Cardiobacterium hominis
- E - Eikenella corrodens
- K - Kingella kingae (and Kingella species)
Why it matters: like the joint infections, HACEK organisms are fastidious and grow slowly, so they were historically a cause of "culture-negative" endocarditis - hence the same diagnostic lesson applies (prolonged incubation, enriched/automated blood-culture systems, and molecular methods improve yield). In children, Kingella endocarditis is rarer than its osteoarticular disease but carries far higher morbidity and mortality, can affect previously normal valves, and may present with embolic phenomena. This is the rationale for echocardiography in a child with Kingella bacteraemia, especially with a murmur or persistent positive cultures.
Exam point: "What is the HACEK group and why does it matter?" - fastidious Gram-negative oropharyngeal flora causing subacute culture-negative endocarditis; Kingella is the K, and the same fastidious-organism diagnostic principles (enriched media, prolonged incubation, PCR) recur.
Classification and Types
Osteoarticular Manifestations of Kingella kingae
- Frequency
- 50-65 percent of cases
- Common Sites
- Knee, hip, ankle, shoulder
- Distinguishing Features
- Indolent; lower joint aspirate WBC than Staph; may mimic transient synovitis
- Frequency
- 20-30 percent of cases
- Common Sites
- Distal femur, proximal tibia, calcaneus, talus
- Distinguishing Features
- Subacute presentation; MRI shows bone marrow oedema; lower CRP
- Frequency
- 5-10 percent of cases
- Common Sites
- Lumbar (L2-L4 most common)
- Distinguishing Features
- Refusal to walk, back stiffness, irritability; MRI shows disc and adjacent vertebra changes
- Frequency
- Reported feature
- Common Sites
- Foot and ankle tendons most common
- Distinguishing Features
- Relatively distinctive for Kingella; tendon sheath swelling with minimal joint involvement
- Frequency
- Rare but serious
- Common Sites
- Mitral and aortic valves
- Distinguishing Features
- Part of HACEK group; consider if cardiac murmur with Kingella bacteraemia; high morbidity
Septic arthritis is by far the most common manifestation and the one most likely to appear in examinations.
Clinical Assessment
- Age: Typically 6-48 months; daycare attendance is an important clue
- Onset: Gradual over days to a week (indolent)
- Preceding illness: Upper respiratory infection or oral ulcers in up to 50 percent of cases
- Symptoms: Limp, refusal to walk, irritability, reduced use of limb
- Fever: Low-grade or absent (unlike the high fever of Staph aureus)
- Weight-bearing: May partially weight-bear (child limps but walks)
- General: Child may appear well or mildly unwell (not toxic)
- Joint: Effusion, warmth, restricted range of motion (especially in hip, knee, ankle)
- Tenderness: Localized to affected joint or metaphyseal region
- Spine: Refusal to sit or walk, back stiffness, paravertebral muscle spasm if spondylodiscitis
- Tendon sheaths: Swelling along tendon sheaths (tenosynovitis pattern) suggests Kingella
- Oropharynx: May see oral ulcers or signs of recent URI
Kingella kingae septic arthritis is frequently misdiagnosed as transient synovitis because the child is afebrile or has low-grade fever, may still weight-bear, and has modest inflammatory markers. The distinction matters: untreated Kingella septic arthritis can cause joint destruction, whereas transient synovitis is self-limiting. Any child under 4 with a joint effusion and limp who is not improving within 24-48 hours should have joint aspiration with inoculation into blood culture bottles and PCR sent. Do not be falsely reassured by normal or mildly elevated inflammatory markers in this age group.
- Age
- 6-48 months
- Fever
- Low-grade or absent
- Key Discriminator
- Indolent; blood culture bottle aspirate + PCR positive
- Age
- Any age
- Fever
- High, toxic
- Key Discriminator
- Acute onset, high CRP/ESR, positive standard cultures
- Age
- 3-8 years (can occur younger)
- Fever
- Low-grade or absent
- Key Discriminator
- Self-limiting; follows URI; all cultures negative; resolves in days
- Age
- 1-3 years
- Fever
- Afebrile
- Key Discriminator
- X-ray shows spiral tibial fracture; no joint effusion; trauma history may be absent
- Age
- 4-8 years (unusual under 3)
- Fever
- Afebrile
- Key Discriminator
- Insidious onset hip limp; X-ray shows femoral head changes; chronic course
- Age
- Any age
- Fever
- Afebrile
- Key Discriminator
- Multiple fractures in different stages; metaphyseal corner fractures; inconsistent history
In a child under 4 presenting with a limp, the presence of recent upper respiratory symptoms or oral ulcers should specifically raise suspicion for Kingella kingae. Unlike Staph aureus, the child looks relatively well. Unlike transient synovitis, the symptoms persist or worsen. The combination of toddler age, indolent onset, preceding URI, and persistent joint findings is the classic Kingella presentation.
Investigations
Diagnostic Workup
CRP: Often only modestly elevated (frequently under 50 mg/L); may be normal initially
ESR: Mildly to moderately elevated; less elevated than Staph aureus
WBC: Frequently normal or only mildly elevated
Blood cultures: Positive in approximately 60 percent of bacteraemic Kingella cases when drawn before antibiotics; yield is higher than joint aspirate on standard media
Key point: Normal inflammatory markers do NOT exclude Kingella osteoarticular infection. Clinical suspicion must guide investigation.
Technique: Ultrasound-guided if deep joint (hip); aspiration under sterile conditions
CRITICAL step: Inoculate aspirate directly into blood culture bottles (BACTEC or similar), NOT onto agar plates. The fastidious organism thrives in liquid enrichment media. Yield increases dramatically compared with standard plating.
Synovial fluid WBC: Often lower than the classical 50,000/mL threshold for septic arthritis. Counts of 10,000-40,000/mL are common with Kingella.
Gram stain: Usually negative (organism is difficult to visualize)
Send for PCR: If available, send synovial fluid for real-time PCR targeting cpn60 or other Kingella-specific gene targets.
Target: cpn60 gene (chaperonin) or other Kingella-specific sequences
Sensitivity: Far superior to culture; detects organism even after antibiotics started
Turnaround: Hours to days depending on laboratory
Clinical impact: Studies using PCR have shown Kingella is responsible for the majority of osteoarticular infections in children under 4, replacing "culture-negative" as the most common category
Availability: Not universally available; varies by institution and country. Where unavailable, blood culture bottle inoculation remains the most practical strategy.
X-ray: Often normal early. May show soft tissue swelling, joint space widening, or late periosteal reaction in osteomyelitis. In spondylodiscitis: disc space narrowing with adjacent endplate changes.
Ultrasound: Detects joint effusion (hip, knee, ankle). Guides aspiration. Demonstrates synovial thickening and tenosynovitis.
MRI: Most sensitive for osteomyelitis and spondylodiscitis. Shows bone marrow oedema (T2/STIR hyperintensity), soft tissue involvement, and joint effusion. Essential for surgical planning if abscess present.
Bone scan: Rarely needed if MRI available. May be used when multiple sites are suspected.
The single most important investigation step for Kingella is inoculating joint aspirate into blood culture bottles. This simple technique transforms culture yield from near-zero on standard agar to substantially improved detection. In exam scenarios, always mention this step when discussing paediatric joint aspiration. Combined with PCR (where available), diagnostic accuracy approaches 100 percent for Kingella osteoarticular infections.
BOTTLEDiagnostic Approach to Kingella
Hook:Put the joint aspirate in a BOTTLE and your culture yield will soar!
Management Algorithm
Kingella kingae Septic Arthritis
Goal: Eradicate infection and preserve joint function
Treatment Protocol
Joint aspiration: Ultrasound-guided for hip; aspirate under sterile conditions
Inoculate into blood culture bottles: Send for PCR if available
Blood tests: CRP, ESR, WBC, blood cultures
Start empiric antibiotics: Do not wait for culture results. IV cefazolin or ampicillin/sulbactam
Surgical washout: Indicated for hip septic arthritis (to protect the femoral head) and for any joint with purulent effusion under pressure. Knee and ankle may be managed with aspiration alone if early and the child responds rapidly.
Confirm organism: PCR or blood culture bottle results typically available
Narrow antibiotics: If Kingella confirmed, switch to high-dose ampicillin or cephalexin (organism is uniformly beta-lactam susceptible)
Assess response: Fever should resolve within 24-48 hours. CRP should trend downward. Pain and range of motion should improve.
If not improving: Repeat aspiration, consider MRI for adjacent osteomyelitis or abscess
Oral step-down: Switch to high-dose oral ampicillin or cephalexin once clinically improving and inflammatory markers trending down
Total duration: 3-4 weeks (IV and oral combined). Shorter courses than Staph aureus infections.
Monitoring: Weekly clinical review; repeat CRP at 1 week to confirm downward trend
Clinical: Ensure full return of range of motion and normal gait
Imaging: Follow-up X-ray or ultrasound if initial imaging showed significant changes
Physiotherapy: May be needed if residual stiffness; most children recover full mobility spontaneously
Long-term: Excellent prognosis; significant joint damage is rare with appropriate treatment
Hip septic arthritis always warrants surgical washout regardless of the organism, because increased intracapsular pressure threatens the femoral head blood supply. For knee and ankle septic arthritis caused by Kingella, if the child is clinically improving after aspiration and antibiotics, repeat aspiration or washout may not be necessary. However, if there is persistent effusion or inadequate clinical response, formal washout remains appropriate.
The mnemonics above say Kingella is "uniformly susceptible to beta-lactams / no resistance issues." That is the general rule and the prognosis is excellent, but the nuanced, examinable truth is that a minority of K. kingae strains produce a beta-lactamase (TEM-type), and the proportion is region- and carriage-dependent (reported higher in some carriage surveys). A beta-lactamase-positive strain can render plain penicillin or ampicillin ineffective.
Practical consequences:
- This is a major reason many centres choose a beta-lactamase-stable cephalosporin (e.g. cefazolin / cefuroxime) for empiric and definitive therapy, or amoxicillin-clavulanate, rather than plain ampicillin - the cephalosporin covers the organism whether or not it produces the enzyme.
- Susceptibility testing should still be performed when the organism is isolated; do not assume penicillin will work in a slow or non-responding case.
- Kingella remains resistant to many agents used against other paediatric pathogens - notably it has reduced susceptibility to clindamycin and vancomycin and intrinsic resistance to several others, so an MRSA-oriented empiric regimen (e.g. vancomycin/clindamycin alone) can under-treat a Kingella infection. This is an argument for including beta-lactam cover in the under-4 age group.
Exam point: Kingella is usually but not uniformly beta-lactam susceptible - beta-lactamase-producing strains exist, so a cephalosporin (or co-amoxiclav) is the safer empiric/definitive choice, and a clindamycin/vancomycin-only "Staph" regimen may miss it.
CUREKingella kingae Treatment
Hook:You will CURE Kingella infections easily with beta-lactams!
Complications
- Incidence
- Mild and transient in most cases
- Risk Factors
- Delayed treatment, inadequate physiotherapy
- Management
- Physiotherapy; usually resolves spontaneously in young children
- Incidence
- Rare with Kingella
- Risk Factors
- Osteomyelitis adjacent to physis; delayed treatment
- Management
- Monitor growth with serial clinical and radiographic assessment; epiphysiodesis if significant discrepancy
- Incidence
- Very rare with Kingella
- Risk Factors
- Delayed diagnosis, inadequate antibiotic duration
- Management
- Prolonged antibiotics; surgical debridement if sequestrum
- Incidence
- Reported but uncommon
- Risk Factors
- Hip septic arthritis with delayed washout
- Management
- Similar to any septic hip: proximal femoral osteotomy or reconstruction if deformity
- Incidence
- Rare but life-threatening
- Risk Factors
- Bacteraemia with cardiac involvement
- Management
- Prolonged IV antibiotics (4-6 weeks); cardiac surgery if valve destruction
Kingella kingae osteoarticular infections have a markedly better prognosis than Staph aureus infections when treated appropriately. However, the indolent presentation means diagnosis is often delayed, and the clinician must remain vigilant for complications, particularly in hip septic arthritis (risk of avascular necrosis) and endocarditis (rare but associated with significant morbidity). Any child with Kingella bacteraemia should have cardiac evaluation including echocardiography.
Outcomes and Prognosis
- Typical Treatment
- IV then oral beta-lactam 3-4 weeks; washout for hip
- Expected Outcome
- Rapid improvement in 24-48 hours; full recovery typical
- Long-term Sequelae
- Rare; excellent prognosis with appropriate treatment
- Typical Treatment
- IV then oral beta-lactam 3-4 weeks
- Expected Outcome
- Good resolution; faster than Staph aureus
- Long-term Sequelae
- Growth disturbance very rare; monitor if physeal involvement
- Typical Treatment
- IV then oral beta-lactam 3-4 weeks
- Expected Outcome
- Excellent; disc space fusion well tolerated
- Long-term Sequelae
- Spontaneous disc fusion common; rarely symptomatic
- Typical Treatment
- Prolonged IV beta-lactam 4-6 weeks
- Expected Outcome
- Variable; depends on valve involvement
- Long-term Sequelae
- Valve destruction possible; may require cardiac surgery
The prognosis for Kingella kingae osteoarticular infections is excellent when the diagnosis is made and appropriate antibiotics are administered. This is in stark contrast to Staph aureus, which carries a higher rate of complications including chronic osteomyelitis, growth disturbance, and joint destruction. The key is early recognition: any child under 4 with an indolent joint or bone presentation should have Kingella specifically investigated using blood culture bottle inoculation and PCR.
Key threshold: Children who start appropriate antibiotics within the first week of symptoms have near-universal excellent outcomes. Delayed diagnosis beyond 2-3 weeks modestly increases the risk of residual joint stiffness but significant long-term morbidity remains uncommon.
Guidelines, Registries & Global Practice
- Israel, Switzerland, France: Highest reported Kingella rates (pioneers of PCR-based diagnosis)
- North America: Increasingly recognized; studies from US centres show Kingella as a dominant pathogen in toddlers when PCR is used
- Australia and New Zealand: Emerging data; the organism is recognized in paediatric orthopaedic guidelines
- Resource-limited settings: Kingella is likely under-diagnosed globally because PCR and blood culture bottle inoculation are not universally available
- High-resource (PCR available): Kingella confirmed as the dominant osteoarticular pathogen under 4 years; PCR-guided targeted therapy with short beta-lactam courses
- Moderate-resource (blood culture bottles available): Bottle inoculation provides good culture yield; PCR may be limited to reference laboratories
- Limited-resource: Standard agar cultures miss Kingella; many cases treated empirically as "culture-negative septic arthritis" with broad-spectrum antibiotics; clinical outcomes often still good because beta-lactams cover the organism
- Universal principle: The clinical response to beta-lactams is excellent regardless of whether the organism is formally identified
- Organism Emphasis
- Kingella kingae is the commonest osteoarticular pathogen under 4 years
- Diagnostic Approach
- Joint aspirate into blood culture bottles; PCR where available; MRI for osteomyelitis/spondylodiscitis
- Treatment
- IV beta-lactam followed by oral step-down; 3-4 weeks total
- Organism Emphasis
- Recognized as a leading cause in toddlers; included in paediatric musculoskeletal infection guidance
- Diagnostic Approach
- Blood culture bottle inoculation recommended; PCR increasingly available in UK paediatric centres
- Treatment
- IV cefazolin or ampicillin empirically; narrow to beta-lactam once confirmed
- Organism Emphasis
- Swiss and French groups pioneered Kingella recognition; European guidelines increasingly specific
- Diagnostic Approach
- PCR recommended as first-line investigation in children under 4 with osteoarticular infection
- Treatment
- Short-course IV then oral beta-lactam; excellent outcomes
- Organism Emphasis
- Focuses on surgical management of paediatric osteoarticular infections
- Diagnostic Approach
- Joint aspiration into blood culture bottles; biopsy if atypical or failing treatment
- Treatment
- Surgical washout for hip; aspiration may suffice for other joints if early response
There is no specific arthroplasty or implant registry for paediatric osteoarticular infections, as these are medical rather than implant-related conditions. However, multicentre surveillance networks in Europe and North America have tracked Kingella epidemiology. The key global message is that Kingella kingae is underdiagnosed in regions where PCR and blood culture bottle inoculation are not routine practice. The clinical principle is universal: in any child under 4 with an osteoarticular infection, beta-lactam empiric therapy will cover Kingella, and the prognosis with appropriate antibiotics is excellent worldwide.
The dramatic difference in reported Kingella rates between PCR-using and non-PCR-using centres illustrates a fundamental principle: the apparent epidemiology of paediatric osteoarticular infections depends on diagnostic methodology. In exam answers, always specify that Kingella kingae is the commonest cause under 4 years in regions where sensitive detection methods (PCR, blood culture bottles) are employed. In regions relying on standard agar cultures, Staphylococcus aureus may still be reported as the most common pathogen because Kingella is missed.
Controversies & Areas of Uncertainty
Real-time PCR for Kingella kingae is the gold-standard diagnostic test but is not universally available, particularly in resource-limited settings. Blood culture bottle inoculation is a pragmatic and widely accessible alternative that substantially improves yield over standard agar. The global gap in diagnostic capacity means Kingella remains underdiagnosed in many regions.
Most protocols recommend 3-4 weeks total for Kingella osteoarticular infections, but the precise minimum duration has not been defined by randomized trials. Some centres use shorter courses (2-3 weeks) for uncomplicated septic arthritis with good results. The excellent susceptibility profile and rapid clinical response support the trend toward shorter durations, but evidence is limited.
Hip septic arthritis universally requires washout to protect the femoral head. However, for Kingella septic arthritis of the knee, ankle, or other joints, the role of formal washout versus aspiration-alone is debated. Many centres now manage responding cases with aspiration and antibiotics alone, reserving washout for inadequate clinical response. No randomized data exist.
Kingella kingae is a member of the HACEK group and can cause endocarditis. The indication for routine echocardiography in children with Kingella osteoarticular infection is debated. Some experts recommend echocardiography for all bacteraemic Kingella cases, while others reserve it for children with cardiac murmurs or persistent bacteraemia. No consensus guideline exists.
MCQ Practice Points
Q: What is the most common bacterial cause of septic arthritis in children aged 6-48 months (in regions where PCR is used)? A: Kingella kingae. PCR-based studies have shown that Kingella kingae surpasses Staphylococcus aureus as the leading cause of osteoarticular infections in this specific age group. Before PCR, many of these cases were labelled "culture-negative" because the fastidious organism was missed on standard agar.
Q: What is the most important laboratory technique for improving Kingella kingae culture yield from joint aspirate? A: Inoculation into blood culture bottles (liquid enrichment media) rather than plating on standard agar. Kingella kingae is a fastidious Gram-negative coccobacillus that grows poorly on conventional solid media but thrives in the enriched liquid environment of blood culture bottles. This simple technique dramatically increases diagnostic yield.
Q: How does the clinical presentation of Kingella kingae septic arthritis differ from Staphylococcus aureus? A: Kingella presents indolently: low-grade or absent fever, less toxic child, modest CRP elevation (often under 50 mg/L), and the child may still partially weight-bear. Staph aureus presents acutely with high fever, toxic appearance, markedly elevated inflammatory markers, and complete refusal to weight-bear. This distinction is a common exam question.
Q: What is the antibiotic of choice for confirmed Kingella kingae osteoarticular infection? A: High-dose ampicillin or cephalexin (beta-lactams). Kingella kingae is uniformly susceptible to beta-lactam antibiotics. Empiric therapy is typically IV cefazolin or ampicillin, with oral step-down once the child is clinically improving. Total duration is 3-4 weeks. The organism's universal beta-lactam susceptibility and excellent clinical response differentiate it from more resistant pathogens.
Q: What molecular target is used in real-time PCR for Kingella kingae detection? A: The cpn60 gene (chaperonin gene). Real-time PCR targeting cpn60 is the gold-standard diagnostic test for Kingella kingae, with sensitivity far exceeding standard culture methods. It can detect the organism even after antibiotics have been started.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 2-year-old boy presents with a 4-day history of right knee swelling and limp. He has had a mild cold for the past week. He is afebrile, looks well, and is partially weight-bearing on the right leg. Examination reveals a moderate right knee effusion with restricted flexion and extension. CRP is 28 mg/L, ESR is 35 mm/h, and WBC is 11.2. X-ray shows soft tissue swelling only. How would you investigate and manage this child?”
“An 18-month-old girl presents with a 2-week history of irritability, refusal to walk, and increased lumbar lordosis. She has been afebrile throughout. She attends daycare. Blood tests show CRP 22 mg/L, ESR 40 mm/h. MRI of the spine shows disc space narrowing at L3-L4 with adjacent endplate oedema and paravertebral soft tissue swelling. How would you investigate and manage this child?”
Microbiology
- Gram-negative coccobacillus, Neisseriaceae family, fastidious organism
- Oropharyngeal commensal in 10-30 percent of children under 4 years
- Hematogenous spread after mucosal breach (URI, stomatitis, teething)
- Member of HACEK group (rare endocarditis risk)
Clinical Features
- Commonest bacterial cause of SA/OM in children under 4 (where PCR used)
- Indolent: low-grade or absent fever, less toxic child, may partially weight-bear
- CRP and ESR often only mildly elevated; WBC frequently normal
- Preceding URI or oral ulcers in up to 50 percent of cases
Diagnosis
- Joint aspirate into BLOOD CULTURE BOTTLES (not standard agar)
- Real-time PCR targeting cpn60 gene is gold standard
- Blood cultures positive in approximately 60 percent of bacteraemic cases
- MRI for osteomyelitis and spondylodiscitis; ultrasound for joint effusion
Treatment
- Empiric: IV cefazolin or ampicillin; narrow to beta-lactam once confirmed
- Uniformly susceptible to beta-lactams; rapid clinical response (24-48 hours)
- Total duration 3-4 weeks (IV then oral); shorter than Staph aureus protocols
- Hip SA always needs surgical washout; other joints may be aspiration-only if responding
Prognosis & Pitfalls
- Excellent prognosis with appropriate antibiotics; long-term sequelae rare
- Most commonly misdiagnosed as transient synovitis (indolent presentation)
- Do NOT be falsely reassured by normal inflammatory markers in toddlers
- Endocarditis is rare but life-threatening: consider echo if bacteraemic
Evidence Base and Key Trials
Specific real-time polymerase chain reaction places Kingella kingae as the most common cause of osteoarticular infections in young children
- Used real-time PCR targeting cpn60 to detect Kingella kingae in osteoarticular samples from young children
- Kingella kingae was identified as the most common organism causing osteoarticular infections in children under 4 years, surpassing Staphylococcus aureus
- Many cases previously classified as culture-negative were PCR-positive for Kingella
- PCR detection rate far exceeded standard culture methods
Kingella kingae: carriage, transmission, and disease
- Comprehensive review of Kingella kingae biology, epidemiology, and clinical spectrum
- Oropharyngeal colonization rates of 10-30 percent in children under 4 years, declining with age
- Daycare attendance and seasonal clustering (autumn-winter) are consistent epidemiological features
- The organism is uniformly susceptible to beta-lactam antibiotics
Kingella kingae osteoarticular infections in young children: clinical features and contribution of a new specific real-time PCR assay
- Prospective study of young children with osteoarticular infections using a specific real-time PCR assay
- Kingella kingae detected in a majority of cases in children under 4 years
- Clinical presentation was typically indolent with modest inflammatory marker elevation
- Blood culture bottle inoculation of joint aspirate increased culture yield substantially compared with standard agar
Invasive Kingella kingae infections in children: clinical and laboratory characteristics
- Reviewed invasive Kingella infections including osteoarticular infections, bacteraemia, and endocarditis
- Osteoarticular infections comprised the majority of invasive cases
- Preceding upper respiratory infection was documented in a substantial proportion of cases
- Endocarditis, though rare, was associated with significant morbidity and mortality
Osteoarticular infections caused by Kingella kingae in children: contribution of polymerase chain reaction to the microbiologic diagnosis
- Developed and validated a specific PCR assay for Kingella kingae detection in osteoarticular samples
- PCR detected Kingella in cases where all conventional cultures remained negative
- Established the molecular basis for species-specific identification of Kingella kingae