Realignment Osteotomy | Opening vs Closing Wedge | Medial Compartment OA | Young Active Varus | Coventry Principles | Coronal Correction Planning
- HTO is indicated for isolated medial compartment OA in a young, active patient with varus malalignment and a correctable deformity - it is a joint-preserving procedure, not an alternative to TKA in the elderly
- The goal is slight valgus overcorrection (femorotibial angle of approximately 170 degrees or 3-5 degrees of valgus) to shift the mechanical axis into the lateral compartment, unloading the damaged medial side
- Opening wedge is now the dominant technique - it preserves lateral bone stock, avoids fibular osteotomy and peroneal nerve dissection, and does not shorten the limb
- Patient selection is the key to success: full-thickness lateral compartment cartilage loss, inflammatory arthritis, obesity (BMI greater than 30-35), and severe tricompartmental disease are contraindications
- Conversion to TKA after HTO is more challenging after closing wedge (bone loss, patella baja, altered anatomy) than after opening wedge - this is a major argument favouring the opening wedge
- “Always begin a viva answer with patient selection criteria - examiners test whether you know who NOT to operate on
- “The weight-bearing line (WBL) should pass through 62-66% of the tibial plateau width (just lateral to the tibial spine) for optimal correction
- “Conventry's principle: correct the deformity at or near the site of deformity - for a varus knee, that is the proximal tibia
- “The lateral cortex must remain intact in opening wedge HTO - it is the hinge; if it fractures, fixation is destabilised
High Tibial Osteotomy
HTO fails when the lateral compartment is already diseased, when the patient has inflammatory arthritis, when range of motion is severely limited (less than 90 degrees of flexion), or when the varus deformity is too large (greater than 15-20 degrees). Examiners want to see you exclude these patients before describing the technique. A 70-year-old sedentary patient with tricompartmental OA needs a TKA, not an osteotomy.
- Best option
- High tibial osteotomy (opening wedge)
- Reasoning
- Joint-preserving; unloads the medial side; allows return to high-impact activity; delays TKA
- Best option
- Unicompartmental knee arthroplasty (UKA)
- Reasoning
- Predictable pain relief; faster recovery than HTO; but requires intact ligaments and is less durable in the young, active patient
- Best option
- Total knee arthroplasty (TKA)
- Reasoning
- Addresses all compartments; reliable pain relief and function; higher durability in older, lower-demand patients
- Best option
- HTO combined with ACL reconstruction
- Reasoning
- Correcting varus reduces forces on the ACL graft; staged or single-stage depending on surgeon preference
Overview and Indications
The high tibial osteotomy (HTO) is a realignment procedure that corrects varus malalignment of the proximal tibia in order to shift the mechanical axis laterally and unload the damaged medial compartment of the knee. It is a joint-preserving operation for carefully selected younger patients with isolated medial compartment osteoarthritis. The concept was pioneered by Jackson and Waugh and popularised by Coventry at the Mayo Clinic.
by realigning the lower limb from varus into slight valgus, the weight-bearing line (WBL) is transferred from the arthritic medial compartment across to the healthier lateral compartment. This reduces medial compartment contact pressures, relieves pain, and slows disease progression.
- Age less than 60-65 years (some authors extend to 70 in very active patients)
- Isolated medial compartment OA with preserved lateral compartment (full-thickness cartilage on weight-bearing radiographs and MRI)
- Varus malalignment (correctable, typically less than 15-20 degrees of varus)
- Good range of motion (flexion greater than 90 degrees, flexion contracture less than 15 degrees)
- Active patient who wishes to continue impact sports or heavy labour
- Stable knee or instability that can be addressed simultaneously (ACL reconstruction with HTO)
- Motivated and compliant for the prolonged rehabilitation required
- ACL-deficient knee with varus thrust (HTO with or without ACL reconstruction)
- Post-traumatic medial compartment OA after tibial plateau fracture
- Osteonecrosis of the medial femoral condyle (early stage)
Examiners test your ability to say no. Key contraindications: lateral compartment disease, inflammatory arthritis, tricompartmental OA, severe obesity (BMI greater than 30-35), poor range of motion (less than 90 degrees), severe patellofemoral OA, inflammatory or neuropathic arthropathy, and varus greater than 15-20 degrees that exceeds what is correctable by HTO alone.

Relevant Anatomy and Biomechanical Principles
- The proximal tibial metaphysis is subcutaneous anteromedially, making the medial approach straightforward. The tibial tubercle (TT) is a critical landmark - the osteotomy is performed distal to the TT to avoid detaching the patellar tendon insertion.
- The medial collateral ligament (MCL) is released or partially detached during opening wedge HTO to allow distraction; in closing wedge the MCL is preserved.
- The common peroneal (fibular) nerve courses around the fibular neck laterally and is at risk during closing wedge HTO, fibular osteotomy, or proximal tibiofibular joint disruption.
- The popliteal fossa contents (popliteal artery, tibial nerve) lie directly posterior to the proximal tibia; the osteotomy must not breach the posterior cortex beyond a controlled depth.
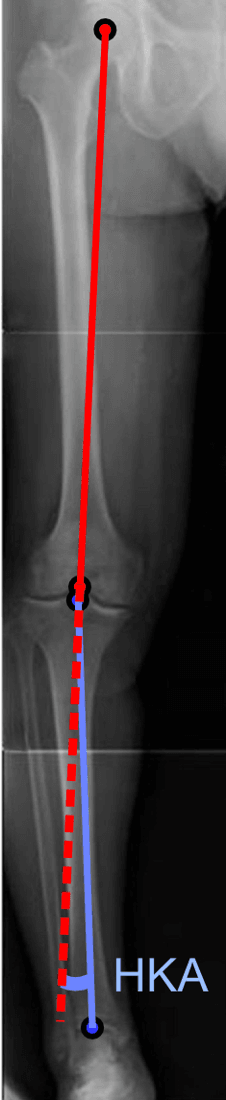
- The mechanical axis runs from the centre of the femoral head to the centre of the ankle mortise. In a normal knee, this passes through or just medial to the centre of the knee.
- In varus malalignment, the mechanical axis falls medial to the knee joint, overloading the medial compartment.
- The weight-bearing line (WBL) is the mechanical axis projected onto the tibial plateau. The goal of HTO is to shift the WBL to 62-66% of the tibial plateau width (measured from the medial edge), placing it just lateral to the tibial eminence.
- Fujisawa point: the classic target, approximately 62-66% across the tibial plateau, corresponds to about 3-5 degrees of valgus femorotibial angle. Overcorrection beyond this risks lateral compartment overload.
- Correct the deformity at or near the site of the deformity
- The osteotomy should be above the tibial tubercle (proximal metaphysis) where bone healing is favourable
- Slight overcorrection into valgus is intentional to account for settling and progressive medial wear
Internervous Plane and Surgical Interval
The approach depends on the type of osteotomy:
- Interval: directly over the anteromedial proximal tibia, between the patellar tendon (fibular collateral ligament side) and the medial collateral ligament. This is a subperiosteal exposure, not a true internervous plane, as the medial proximal tibia is subcutaneous.
- The pes anserinus (gracilis, semitendinosus, sartorius) is encountered and may be released or retracted distally.
- The medial collateral ligament is released from the tibia as a sleeve to allow distraction.
- The superficial medial collateral ligament is the key structure; release must be sufficient to permit opening without spring-back.
- Interval: between the iliotibial band (ITB) anteriorly and the lateral collateral ligament (LCL) / biceps femoris posteriorly.
- The common peroneal nerve is at risk as it passes posterior to the fibular head and must be identified and protected if a fibular osteotomy is performed.
- The proximal tibiofibular joint may be disrupted (Coventry technique) or a fibular osteotomy performed at the mid-shaft to allow the tibial fragments to close.
The common peroneal nerve is the most commonly injured nerve in HTO, particularly during closing wedge procedures that involve fibular osteotomy or proximal tibiofibular joint disruption. Opening wedge avoids this exposure entirely, which is one of its major advantages.
Lateral Hinge Fracture: the Takeuchi Classification
The lateral hinge is the linchpin of an opening-wedge HTO, and an intra-operative or post-operative lateral hinge fracture is graded by the Takeuchi classification, which guides whether extra fixation is needed.
- Fracture location
- Lateral cortex fractures at or just proximal to the proximal tibiofibular joint
- Stability and management
- Usually stable; generally heals with standard fixation and protected weight-bearing
- Fracture location
- Fracture line runs distal to the proximal tibiofibular joint into the metaphysis
- Stability and management
- Potentially unstable; risk of loss of correction and delayed/nonunion - consider additional lateral fixation
- Fracture location
- Fracture extends into the lateral tibial plateau (intra-articular)
- Stability and management
- Unstable; risk of plateau displacement - needs supplementary fixation (lateral plate/screws) and is the most concerning
A fractured lateral hinge is not all-or-nothing: Takeuchi Type I (at or above the tibiofibular joint) is usually stable and heals; Type II (distal into the metaphysis) risks loss of correction and may need extra lateral fixation; Type III (into the lateral plateau, intra-articular) is the unstable one needing supplementary fixation. Recognise it intra-operatively and protect or fix it rather than ignoring it.
Patient Positioning and Setup
- Position: supine on a radiolucent table. A bolster under the ipsilateral hip may help control rotation. The leg is draped free to allow full range of motion and fluoroscopic assessment.
- Anaesthesia: general or spinal anaesthesia. A femoral nerve block or adductor canal block may supplement analgesia but should not block assessment of common peroneal nerve function post-operatively.
- Fluoroscopy: essential. The image intensifier is positioned to obtain AP and lateral views of the proximal tibia. The long-leg alignment view (or intra-operative electrocautery cord from hip to ankle) confirms the mechanical axis correction.
- Tourniquet: a high thigh tourniquet is used for a bloodless field but should be released before wound closure to check haemostasis and assess the common peroneal nerve.
- Pre-operative planning: full-length standing lower-limb radiographs (hip-to-ankle) are mandatory for calculating the required correction angle. The Miniaci, Dugdale or Hernigou method is used to plan the correction.
Surgical Technique
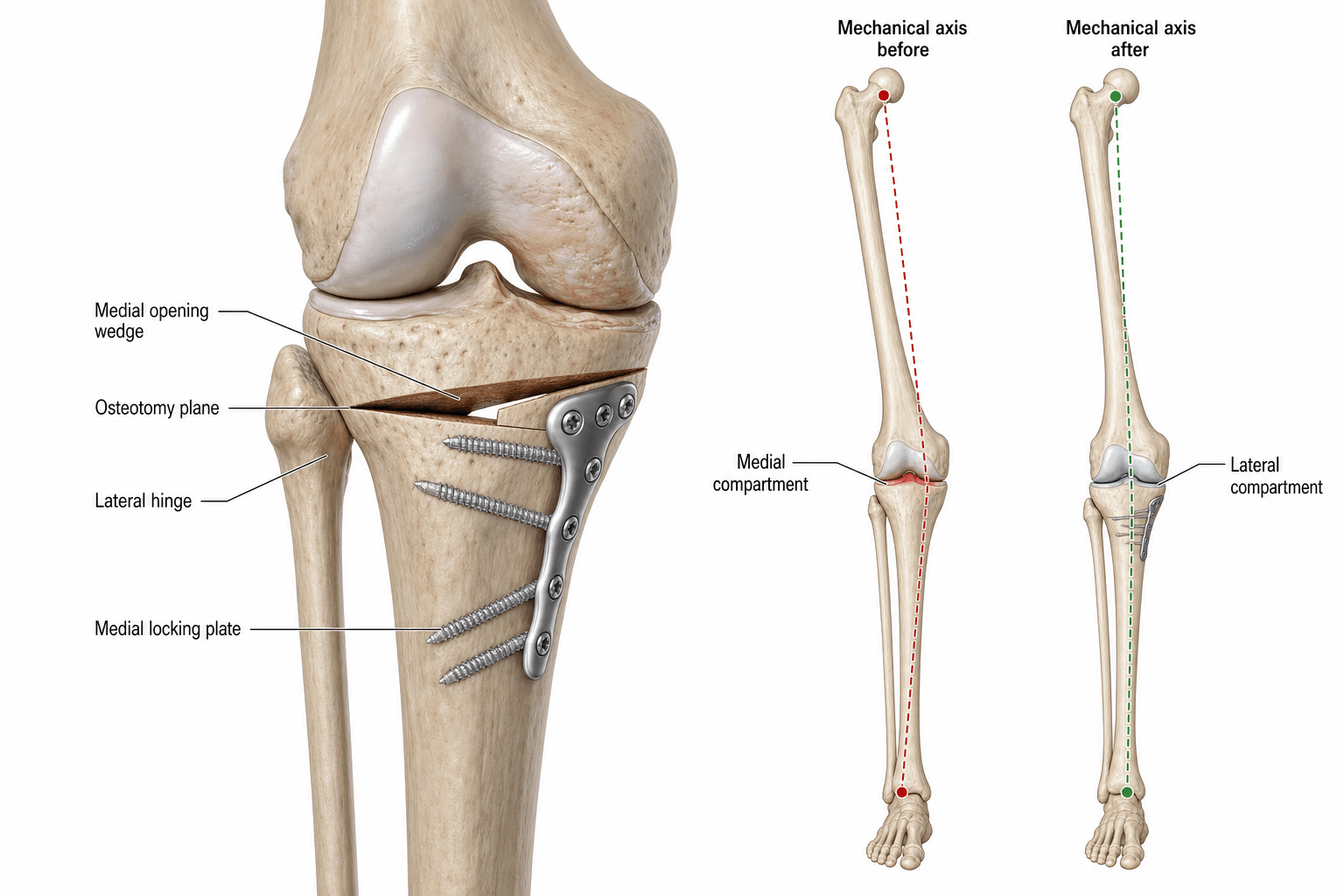

The current workhorse technique. A longitudinal incision is made over the anteromedial proximal tibia, between the patellar tendon and the MCL. The MCL is released subperiosteally. A guide wire is inserted under fluoroscopy from medial to lateral, directed towards the tip of the fibular head, staying proximal to the tibial tubercle and preserving the lateral cortex as a hinge.
The osteotomy is performed with an oscillating saw or osteotomes along the guide wire, stopping approximately 5-10 mm short of the lateral cortex. The osteotomy is gradually opened with a calibrated spreader or wedge dilators to the pre-planned correction. The mechanical axis is checked with an electrocautery cord from the femoral head to the ankle centre (fluoroscopic confirmation at the hip and ankle).
Fixation is achieved with a locked proximal tibial plate (TomoFix, Puddu, or similar) with multiple proximal screws engaging the tibial plateau. The gap may be grafted (autologous iliac crest, BMP, allograft, or bone substitute) depending on the size of the opening and surgeon preference - gaps greater than 10-12 mm are generally grafted.
If the lateral cortex fractures during opening, the osteotomy becomes unstable and the correction cannot be maintained. Protect the hinge by: (1) leaving at least 5-10 mm of intact lateral cortex, (2) using gradual rather than sudden distraction, and (3) positioning the osteotomy obliquely so the lateral exit point is in strong metaphyseal bone near the fibular head. A fractured hinge requires additional fixation (lateral plate) or conversion to a closing wedge.
The Sagittal Plane: Controlling Posterior Tibial Slope
Planning concentrates on the coronal plane, but a medial opening-wedge HTO also changes the posterior tibial slope in the sagittal plane - an examiner favourite because it interacts with cruciate-ligament status.
Why the slope changes:
- The proximal tibia is roughly triangular and wider posteriorly than anteriorly. If the osteotomy gap is opened by an equal amount front and back, the posterior tibial slope increases.
- To keep the slope unchanged in a medial opening wedge, the anterior opening should be about half the posterior opening (a true wedge that is larger posteromedially); opening too much anteriorly inadvertently increases the slope.
- A lateral closing-wedge HTO tends to decrease or maintain the slope, depending on the resection geometry.
Why it matters (cruciate interaction):
- Effect on the tibia
- Tibia translates anteriorly
- Clinical relevance
- Raises ACL strain - avoid in an ACL-deficient or ACL-reconstructed knee; can be used deliberately to help a PCL-deficient knee
- Effect on the tibia
- Tibia translates posteriorly
- Clinical relevance
- Reduces anterior translation - a slope-reducing osteotomy is used for chronic ACL deficiency; avoid in PCL deficiency
A medial opening-wedge HTO increases the posterior tibial slope unless the wedge is deliberately opened wider posteromedially (the anterior opening about half the posterior). In an ACL-deficient or ACL-reconstructed knee, avoid increasing the slope (or actively reduce it); in a PCL-deficient knee, increasing the slope is favourable. Always plan the sagittal plane, not just the coronal correction.
Structures at Risk and Complications
HTO carries a meaningful complication profile. A systematic review reported an overall complication rate of approximately 18-37% depending on technique and definition, with serious complications in approximately 4-10%.
- Common peroneal (fibular) nerve palsy - the most feared nerve complication, predominantly associated with closing wedge HTO, fibular osteotomy, or proximal tibiofibular joint disruption. Most are neuropraxias but some are permanent. Opening wedge HTO largely avoids this risk.
- Nonunion or delayed union - more common in opening wedge HTO with large corrections (greater than 12-15 mm opening) and inadequate fixation or grafting. Smoking is a significant risk factor.
- Loss of correction - collapse of the osteotomy site post-operatively, especially if fixation is insufficient or the lateral hinge fractures.
- Patella baja (infera) - the tibial tubercle-to-joint line distance decreases, particularly after closing wedge HTO. This complicates future TKA exposure (difficulty everting the patella) and alters patellofemoral biomechanics. Opening wedge has less effect or may even increase the TT-TG distance.
- Deep infection - the proximal tibia is subcutaneous; wound dehiscence and deep infection are reported in approximately 1-3% of cases.
- Hardware irritation - prominent plate and screws on the subcutaneous medial tibia frequently require removal after union (approximately 20-40% of cases).
- Compartment syndrome - rare but reported, particularly with extensive soft-tissue dissection or post-operative bleeding.
- Progression of arthritis - lateral compartment OA may develop over time, especially if overcorrected; undercorrection leads to continued medial wear and early failure.
- Vascular injury - the popliteal artery and its branches are at risk if the osteotomy cuts breach the posterior cortex aggressively.
- Fracture into the tibial plateau - intra-articular extension of the osteotomy, particularly if the proximal cut is too close to the joint line or if the lateral hinge fractures into the joint.
After closing wedge HTO, the tibial tubercle moves proximally relative to the joint line (patella baja). During TKA conversion this makes patellar eversion extremely difficult and increases the risk of patellar tendon avulsion. Opening wedge HTO causes less patella baja (or may cause slight patella alta) - another reason it is now preferred.
Guidelines, Registries and Global Practice
There is no single universal guideline for HTO; practice follows the evidence-based principles of patient selection and alignment correction described above. Several international societies have published consensus statements:
- AAOS (US): HTO is recognised as a joint-preserving option in younger patients with varus malalignment and medial compartment OA; the evidence supports strict patient selection criteria. The AAOS clinical practice guideline for knee OA treatment of osteoarthritis (non-arthroplasty) gives a limited recommendation for realignment osteotomy.
- NICE/BOA (UK): osteotomy is supported in national guidance as an option for younger patients with unicompartmental OA and malalignment, often in specialist knee units.
- EFORT/European consensus: European practice has historically been more aggressive in favouring HTO, with large series from France, Germany, and Japan. The European Knee Society has published position statements supporting osteotomy as the first-line joint-preserving procedure for young patients with medial compartment OA and varus.
- National joint replacement registries (NJR - UK, AOANJRR - Australia) track conversion from HTO to TKA, providing real-world survivorship data. Registry data generally confirm approximately 85-90% 10-year survivorship free of TKA conversion.
- The Swedish Knee Register and Finnish Arthroplasty Register have published data showing that prior HTO increases the complexity of subsequent TKA (longer operative time, more blood loss, higher complication rate) but does not significantly compromise implant survivorship when the TKA is performed by experienced surgeons.
- European and Japanese surgeons have historically performed HTO more frequently than surgeons in North America, where UKA and TKA have been more commonly offered to younger patients. This gap is narrowing as long-term data support HTO durability.
- In low- and middle-income settings, HTO is particularly valued as a durable, lower-cost alternative to arthroplasty in young manual labourers.
- The shift from closing wedge to opening wedge is now nearly universal in high-volume centres, driven by the lower nerve injury rate, preservation of bone stock, and easier TKA conversion.
- Conversion is technically more demanding than primary TKA, particularly after closing wedge (patella baja, bone defects, altered tibial anatomy, retained hardware).
- Opening wedge HTO results in less distortion of anatomy and a more straightforward TKA conversion.
- Most registries report good implant survivorship after TKA conversion from HTO, though with slightly higher early complication rates than primary TKA.
Memory Aids
VARUSPatient Selection - VARUS is the KEY
Hook:Only operate when all five VARUS criteria are met - the wrong patient is the commonest cause of HTO failure
OPENOpening vs Closing Wedge - OPEN vs CLOSE
Hook:OPEN preserves bone and is adjustable; CLOSE removes bone but heals by direct apposition
HTOComplications After HTO - DANGER
Hook:HTO complications cluster around DANGER - Deep infection, Arthritis progression, Nerve injury, Graft problems, Extensor mechanism, Reoperation
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 48-year-old labourer presents with progressive right knee pain localised to the medial compartment. He has a visible varus deformity. Standing radiographs show isolated medial compartment OA with a varus mechanical axis deviation of 8 degrees. The lateral compartment is preserved. Discuss your management.”
“A 58-year-old woman had a closing wedge HTO 12 years ago at age 46. She now has progressive, global knee pain and worsening function. Radiographs show lateral compartment osteoarthritis with a valgus mechanical alignment and patella baja. How would you manage her?”
One-liner
- Realignment osteotomy of the proximal tibia for isolated medial compartment OA with varus malalignment in young active patients
- Pioneered by Jackson/Waugh and Coventry; goal is to shift the weight-bearing line laterally into the healthy lateral compartment
Patient selection (VARUS)
- Varus less than 15-20 degrees, correctable
- Active, age less than 60-65
- Range of motion greater than 90 degrees
- Unicompartmental (medial) disease, lateral cartilage preserved
- Stable knee (or reconstructable)
Contraindications
- Lateral compartment OA, tricompartmental disease
- Inflammatory arthritis (RA, etc.)
- BMI greater than 30-35, smoking
- Severe stiffness (less than 90 degrees flexion)
- Neuropathic joint, severe PFJ disease
Correction planning
- Full-length standing hip-to-ankle radiographs mandatory
- Target: WBL at 62-66% tibial plateau (Fujisawa point)
- Aim for 3-5 degrees valgus femorotibial angle
- 1 mm opening roughly equals 1 degree correction
- Methods: Miniaci, Dugdale, Hernigou
Opening vs Closing wedge
- Opening: medial approach, lateral hinge intact, adjustable, preserves bone stock, no fibular osteotomy, easier TKA later
- Closing: lateral approach, wedge resection, Coventry technique, fibular osteotomy needed, peroneal nerve at risk, causes patella baja
Complications (DANGER)
- Deep infection (1-3%)
- Arthritis progression (lateral compartment)
- Nerve palsy (common peroneal, mainly closing wedge)
- Graft/nonunion problems (opening wedge, large corrections)
- Extensor mechanism: patella baja (closing wedge), hardware irritation
- Reoperation/conversion to TKA at 10-15 years (~10-15%)
Conversion to TKA
- More complex than primary TKA
- Patella baja makes exposure difficult (plan tibial tubercle osteotomy)
- Bone defects may require augments or stems
- Opening wedge conversion is easier than closing wedge
- Long-term implant survivorship is comparable to primary TKA
Evidence Base
- In 87 valgus proximal tibial osteotomies (median follow-up 10 years), survivorship depended on two factors: angular correction and body weight. If valgus angulation at one year was 8 degrees or more and the patient was not substantially overweight, survival was at least 90% at 5 years and 65% at 10 years; if valgus was less than 8 degrees in an overweight patient, survival fell to 38% at 5 years and 19% at 10 years.
- Serial arthroscopy before and after HTO showed that fibrocartilaginous repair of the ulcerated medial compartment occurred when the mechanical axis was realigned to pass through a point about 30 to 40 per cent lateral to the midpoint of the tibial plateau (the Fujisawa point). Repair of the affected area was well established by roughly one and a half to two years after surgery when correction was ideal.
- In 42 patients randomised to medial opening-wedge or lateral closing-wedge HTO (both fixed with a TomoFix plate), radiostereometry showed no clinically relevant difference in fixation stability, time to full weight-bearing, union, or improvement in pain and function. The opening-wedge technique was more likely to achieve the intended correction.
- Across 21 randomised/controlled trials (1,065 patients), valgus high tibial osteotomy reduced pain and improved knee function in medial-compartment osteoarthritis. No clear difference was demonstrated between different osteotomy techniques, and there was insufficient evidence to conclude whether HTO is superior to unicompartmental knee replacement or to non-operative care. The aHTO group had a higher reoperation rate (largely hardware removal) than closing-wedge.