Joint Space Narrowing | Conservative First | THA When Failed
- Groin pain with activity is classic presentation
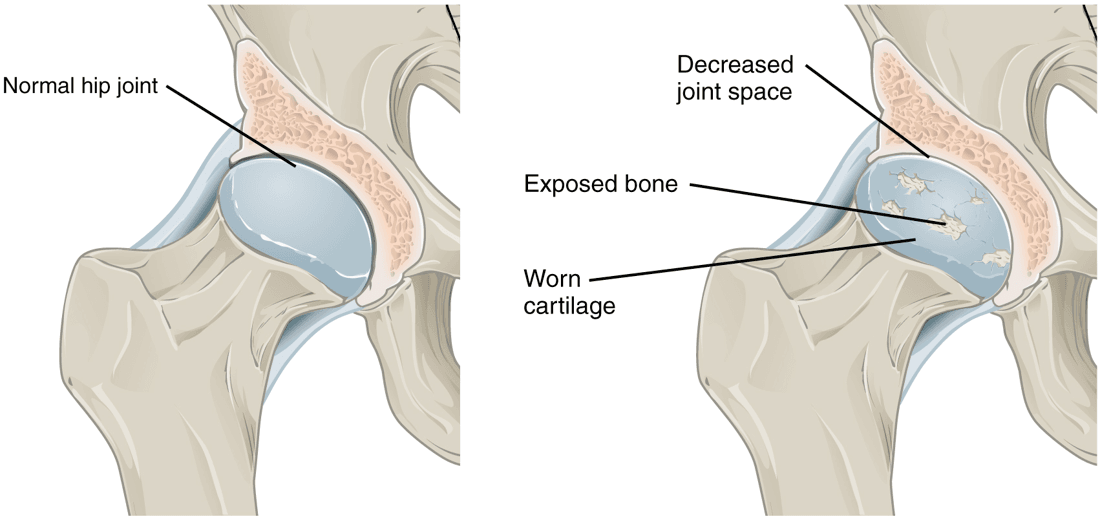
- Radiographs: JSN, osteophytes, sclerosis, cysts
- Conservative FIRST: weight loss, PT, NSAIDs, injections
- THA when conservative fails and quality of life impaired
- Primary OA most common; secondary includes AVN, DDH, FAI
- “Internal rotation first motion lost
- “AP pelvis + lateral of affected hip for imaging
- “Young patients consider hip preservation before THA
- “Avoid THA in active infection, poor health that precludes surgery
True hip pathology causes GROIN pain. Lateral hip pain is often trochanteric bursitis. Buttock pain may be referred from spine.
Always trial conservative measures before THA. Weight loss, physiotherapy, walking aids, NSAIDs, injections. Surgery for failed conservative.
Classic X-ray changes: Joint space narrowing, osteophytes, subchondral sclerosis, subchondral cysts. LOSS is mnemonic.
Consider hip preservation first in young patients - osteotomy, arthroscopy for FAI/labral tears. THA means revision surgery in future.
- Pain Location
- Groin
- Key Feature
- Activity-related, stiffness
- Imaging
- JSN, osteophytes
- Pain Location
- Lateral
- Key Feature
- Point tenderness GT
- Imaging
- Normal or bursitis
- Pain Location
- Groin
- Key Feature
- Risk factors (steroids, alcohol)
- Imaging
- Crescent sign, collapse
- Pain Location
- Groin, clicking
- Key Feature
- Younger, mechanical symptoms
- Imaging
- MRA shows tear
LOSSOA X-ray Findings
Hook:LOSS of cartilage causes all these changes!
DAFTSecondary OA Causes
Hook:DAFT causes lead to secondary OA!
WIPEConservative Treatment
Hook:WIPE out the pain with conservative treatment!
Overview and Epidemiology
Primary OA = no identifiable cause (wear and tear). Secondary OA = underlying condition (DDH, AVN, FAI, trauma, inflammatory arthritis). Secondary OA often affects younger patients.
- 10% of adults over 60
- Increases with age
- More symptomatic in females
- Obesity major risk factor
- Leading indication for THA
- Age: Primary risk factor
- Obesity: Increased joint loading
- Genetics: Strong family history component
- Occupation: Heavy labor
- Prior pathology: DDH, Perthes, SCFE, FAI
Pathophysiology and Anatomy
Hip Joint Anatomy
Femoral head articulates with acetabulum.
Hyaline cartilage covers both surfaces. 3-4mm thick.
Fibrocartilaginous rim deepens socket by 22%.
Strong, reinforced by iliofemoral, pubofemoral, ischiofemoral ligaments.
MFCA (primary to head), LFCA, artery of ligamentum teres.
In younger patients (under 50) with hip OA, always consider secondary causes - DDH, AVN, FAI, SCFE sequelae. These affect treatment planning and prognosis.
Classification Systems
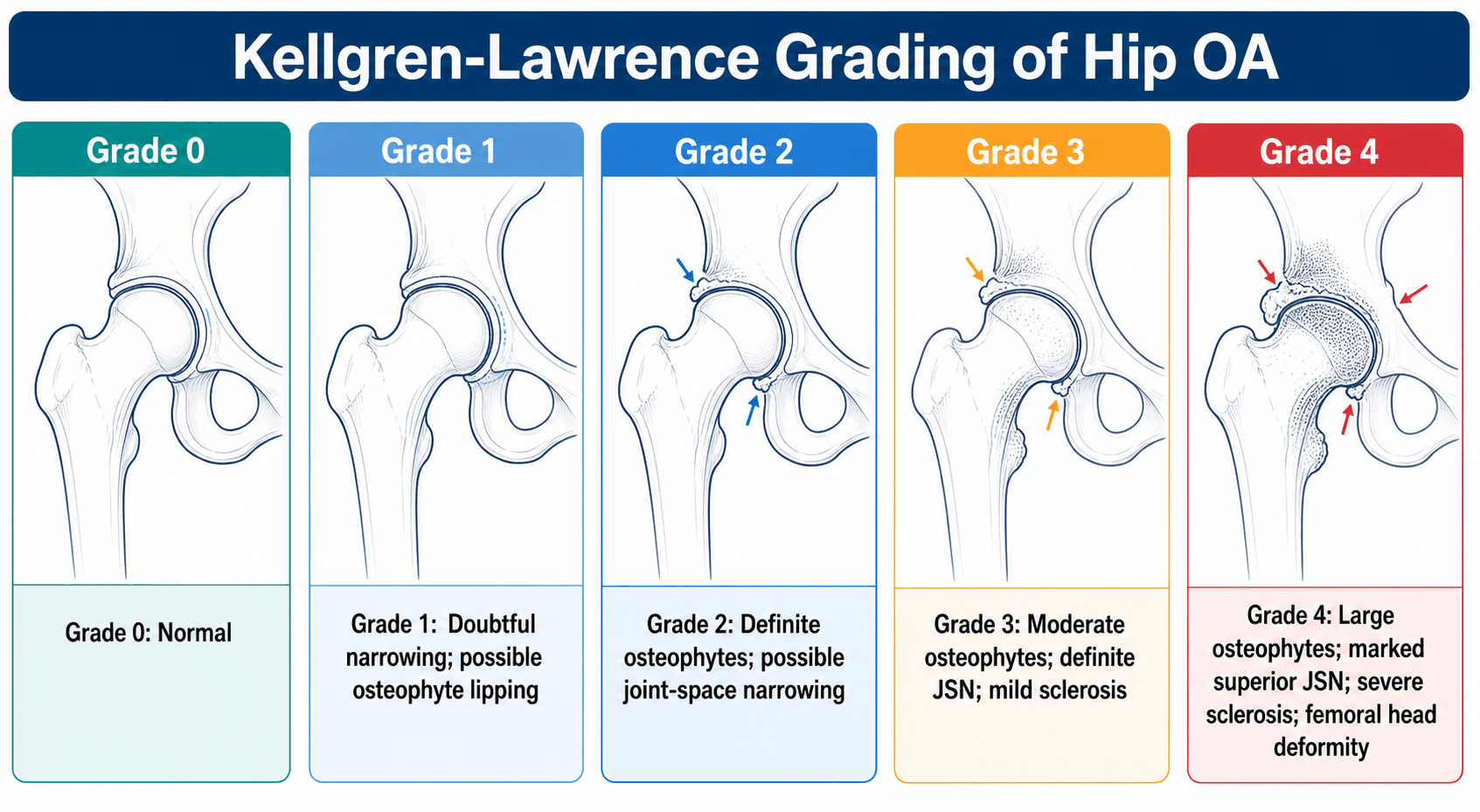
Kellgren-Lawrence Grading
- Description
- No features of OA
- Clinical Correlation
- Normal
- Description
- Doubtful JSN, possible osteophytes
- Clinical Correlation
- May be asymptomatic
- Description
- Definite osteophytes, possible JSN
- Clinical Correlation
- Mild symptoms
- Description
- Moderate osteophytes, definite JSN, some sclerosis
- Clinical Correlation
- Moderate symptoms
- Description
- Large osteophytes, marked JSN, severe sclerosis, cysts
- Clinical Correlation
- Severe, THA candidate
Widely used, good inter-observer reliability for extremes.
Clinical Assessment
- Pain: Groin (true hip), activity-related
- Stiffness: Morning, improves with movement
- Function: Walking distance, stairs, ADLs
- Night pain: Advanced disease
- Impact on QoL: Work, recreation, sleep
- Gait: Antalgic, Trendelenburg
- ROM: Internal rotation lost first
- FABER/FADIR: Provoke pain
- Leg length: May be shortened
- Trendelenburg: Abductor weakness
Internal rotation is the first motion lost in hip OA and often the most painful. Check ROM with patient supine and hip at 90 degrees flexion for accurate assessment.
Outcome Measures
Classic outcome measure. Pain, function, ROM, deformity.
Patient-reported, 12 questions. Widely used.
Hip Disability and Osteoarthritis Outcome Score. Comprehensive.
Investigations
Plain Radiographs
- AP pelvis (weight-bearing if possible)
- Lateral of affected hip (cross-table or frog-leg)
- Loss of joint space
- Osteophytes
- Subchondral sclerosis
- Subchondral cysts
May underestimate cartilage loss compared to MRI.
Weight-bearing AP pelvis shows true joint space narrowing. Non-weight-bearing films may overestimate cartilage thickness. Always try to obtain weight-bearing views.

Management Algorithm
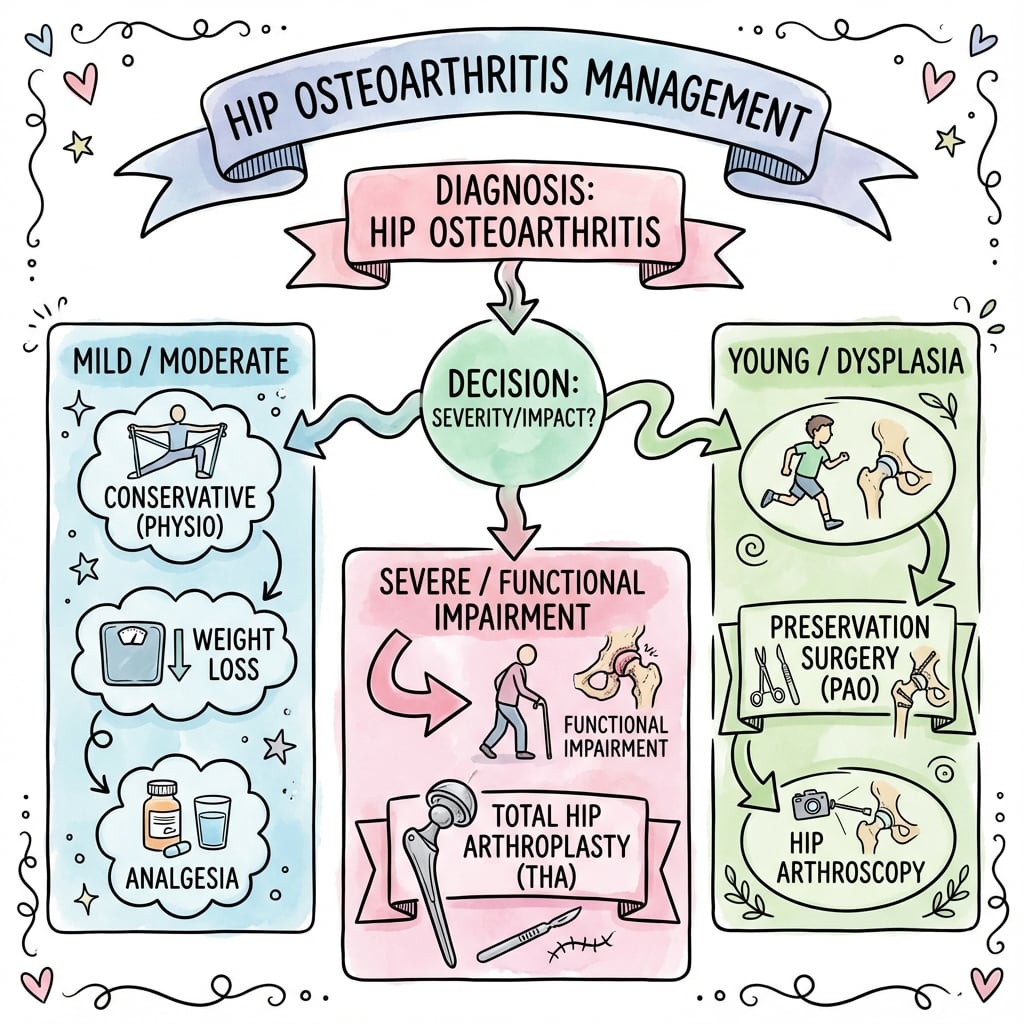
Hip OA Treatment Algorithm
Management Pathway
Clinical history and examination. Radiographs. Rule out secondary causes.
Weight loss, exercise, PT, NSAIDs, walking aids. Trial injections if needed.
If quality of life significantly impaired despite conservative measures, consider surgery.
THA (most common). Consider preservation surgery in young if appropriate.
Surgical Considerations
Indications for THA
- Failed conservative treatment
- Significant functional impairment
- Pain affecting quality of life
- Radiographic evidence of OA
- Active infection
- Poor health precluding surgery
- Unrealistic expectations
- Neuropathic joint (Charcot)
Age alone is not a contraindication.
Young patients (under 50) undergoing THA must be counseled about revision surgery probability. Current implants may last 20+ years but revision is likely within their lifetime.
THA Bearing Surfaces
The articulating couple, or bearing, determines wear, particle generation and therefore long-term survival. Wear debris drives osteolysis and aseptic loosening, so bearing choice is a core arthroplasty decision, particularly in younger, more active patients.
- Wear and behaviour
- Historical standard with relatively high polyethylene wear generating debris
- Key concern
- Osteolysis and aseptic loosening over time
- Wear and behaviour
- Markedly lower wear than conventional polyethylene; current workhorse
- Key concern
- Small oxidation risk, addressed by vitamin-E-doped variants
- Wear and behaviour
- Lowest wear, highly biocompatible, no metal ions
- Key concern
- Rare fracture and occasional squeaking
- Wear and behaviour
- Low volumetric wear but releases cobalt and chromium ions
- Key concern
- ALVAL, pseudotumour and high early revision; largely abandoned
Cross-linking polyethylene dramatically reduces wear and the osteolysis that historically limited implant life, which is why metal- or ceramic-on-highly-cross-linked-polyethylene and ceramic-on-ceramic have replaced conventional polyethylene and metal-on-metal in most practice. Metal-on-metal bearings are now avoided because cobalt and chromium ion release causes ALVAL and pseudotumours.
THA Fixation: Cemented versus Uncemented
Components are fixed to bone either with polymethylmethacrylate (PMMA) cement or by biological bony integration. Cement is not an adhesive: it works by mechanically interdigitating into prepared trabecular bone, the principle behind Charnley's low-friction arthroplasty. Uncemented implants achieve fixation through bone ingrowth into a porous surface or ongrowth onto a hydroxyapatite coating, which requires a stable press-fit and adequate bone quality.
- Mechanism and best suited to
- PMMA interdigitation; reliable in older or osteoporotic bone; registries show low revision for cemented stems in older patients
- Key concern
- Bone cement implantation syndrome (hypotension, hypoxia, arrhythmia during cementation)
- Mechanism and best suited to
- Bone ingrowth or ongrowth; favoured in younger patients with good bone; needs initial press-fit stability
- Key concern
- Periprosthetic fracture, thigh pain and stress shielding
- Mechanism and best suited to
- Cemented stem with an uncemented cup (or the reverse), combining the advantages of each
- Key concern
- Selection by bone quality, age and surgeon practice
Bone cement fixes the implant by interdigitating into trabecular bone, not by adhesion. Cemented or hybrid fixation gives lower revision in older patients in registry data, while uncemented fixation is usually chosen for younger patients with good bone. Be alert to bone cement implantation syndrome during pressurised cementation.
Complications
- Conservative
- NSAIDs risk
- THA
- N/A
- Conservative
- N/A
- THA
- 1% (PJI)
- Conservative
- N/A
- THA
- 1-3%
- Conservative
- N/A
- THA
- Despite prophylaxis
- Conservative
- N/A
- THA
- Measured and addressed
- Conservative
- N/A
- THA
- Long-term, leads to revision
NSAIDs have significant risks: GI bleeding, renal impairment, cardiovascular events. Use lowest dose for shortest time. Consider PPI cover. Acetaminophen is safer for chronic use.
Postoperative Care (THA)
THA Recovery
Mobilize day of surgery. DVT prophylaxis. Pain control. Precautions if posterior approach.
Discharge home 1-3 days. PT, gait aids. Wound care. Continue DVT prophylaxis.
Increase mobility. Wean walking aids. Drive when safe. Return to desk work.
Most return to pre-morbid activities. Low-impact sport allowed. Full function.
Posterior approach precautions: Avoid hip flexion greater than 90 degrees, internal rotation, adduction past midline. Duration varies (6-12 weeks). Anterior approach may have fewer precautions.
Outcomes and Prognosis
THA Outcomes
95%+ at 15 years in correctly selected patients.
Dramatic pain relief and functional improvement.
Over 90% satisfied.
Higher in young, active patients. Polyethylene wear, loosening, infection main causes.
Non-Operative Outcomes
Progressive deterioration. Rate varies.
Symptom management. Does not alter disease progression.
Guidelines, Registries & Global Practice
Global Epidemiology
- 595 million people lived with osteoarthritis worldwide in 2020 (7.6% of the global population); hip OA cases are projected to rise about 79% by 2050 with population ageing.
- High BMI accounts for roughly one-fifth of total OA burden, making obesity the dominant modifiable risk factor.
- Symptomatic radiographic hip OA prevalence rises steeply after age 50; secondary OA (DDH, FAI, AVN, post-trauma) predominates in younger patients.
Side-by-Side Major Guidelines
- Core Recommendation
- Therapeutic exercise as core treatment for all; offer arthroplasty when QoL substantially impaired
- Notable Position
- Do NOT refer based on age, sex, BMI or smoking alone; paracetamol/weak opioids deprioritised
- Core Recommendation
- Strongly recommends exercise and weight management; arthritis education core
- Notable Position
- Conditional support for topical/oral NSAIDs; IA steroid for short-term relief
- Core Recommendation
- Strong evidence for NSAIDs and physical therapy; THA effective for end-stage disease
- Notable Position
- Limited/inconclusive evidence for viscosupplementation and glucosamine in the hip
- Core Recommendation
- Strongly recommends exercise, weight loss, oral/topical NSAIDs; conditional IA steroid
- Notable Position
- Strongly recommends AGAINST hyaluronic acid injection in the hip
Registry Evidence
- National registries (AOANJRR, NJR for England and Wales, Swedish and Norwegian arthroplasty registries) consistently show THA among the most successful elective operations, yet report lower long-term survival than single-centre case series.
- Pooled registry data indicate about 58% of hip replacements survive to 25 years, versus the over-optimistic 78% from case series - the figure to quote when consenting younger patients.
- Registries demonstrate higher revision rates in younger, more active patients and have driven away from metal-on-metal bearings after high early-revision signals.
High- vs Limited-Resource Practice
- Timely access to elective THA, advanced bearings, navigation/robotics in some centres
- Registry-guided implant selection and outcome surveillance
- Multidisciplinary conservative care (physiotherapy, weight-management programmes)
- Arthroplasty may be unaffordable or unavailable, leading to prolonged conservative management and disability
- Greater reliance on analgesia, exercise and walking aids; later presentation with advanced disease
- GBD highlights this access gap as a driver of global health inequity
Hip OA is extremely common in viva. Know conservative treatment first, THA indications, and be able to consent a patient with registry-based longevity figures (around 58% at 25 years). Discuss approaches, complications, and manage expectations appropriately.
Controversies and Areas of Uncertainty
The McAlindon JAMA trial showed scheduled intra-articular triamcinolone caused greater cartilage loss with no durable pain benefit (in the knee). Whether repeated hip injections accelerate joint failure or compromise later arthroplasty remains debated; most now reserve injection for short-term flare relief or diagnosis.
PROHIP confirms THA outperforms exercise once a surgical indication exists, but around 1 in 5 patients improve enough with exercise to defer surgery. Defining the "tipping point" - and avoiding both premature and unduly delayed surgery - is unresolved.
Direct anterior versus posterior approach remains contested: anterior may speed early recovery but carries a learning curve and lateral femoral cutaneous nerve risk. Registry data show approach matters less than surgeon volume and experience.
In young dysplastic or FAI hips, the threshold of remaining cartilage at which PAO or arthroscopy still works (versus proceeding to THA) is uncertain; established radiographic OA predicts PAO failure.
There is no proven disease-modifying drug for hip OA. Glucosamine, chondroitin and hyaluronic acid injection lack convincing evidence in the hip (ACR strongly recommends against hip viscosupplementation). All current treatment is symptomatic or surgical.
MCQ Practice Points
Q: Where does true hip pathology cause pain? A: GROIN. Lateral pain = trochanteric bursitis. Buttock pain = sacroiliac or lumbar spine.
Q: What is the first motion lost in hip OA? A: Internal rotation. Often most painful as well. Test at 90 degrees flexion.
Q: What are the radiographic features of OA (LOSS)? A: Loss of joint space, Osteophytes, Subchondral Sclerosis, Subchondral cysts.
Q: What is Kellgren-Lawrence Grade 4? A: Large osteophytes, marked joint space narrowing, severe sclerosis, cysts, bone-on-bone. End-stage OA.
Q: What is first-line treatment for hip OA? A: Conservative: weight loss, exercise, physiotherapy, acetaminophen, walking aids. NSAIDs with caution.
Q: What is 15-year survival of THA? A: Greater than 95% in correctly selected patients. Higher revision in young, active patients.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old woman presents with 2 years of progressive right groin pain worse with walking and stairs. She has stiffness in the morning for 20 minutes. X-rays show joint space narrowing, osteophytes, and subchondral sclerosis. She has not tried any formal treatment. What is your management?”
“A 42-year-old active man presents with bilateral hip pain and stiffness. X-rays show moderate bilateral hip OA with acetabular dysplasia (CE angle 18 degrees). He is frustrated with symptoms affecting his tennis. What is your approach?”
“A 72-year-old woman has tried physiotherapy, lost 8kg, uses a walking stick, and has had two steroid injections over 18 months. She still has significant right hip pain limiting her to walking 200m and disturbing her sleep. X-rays show bone-on-bone changes. She asks about her options. What would you advise?”
Presentation
- Groin pain (true hip)
- Activity-related, improves with rest
- Morning stiffness (less than 30 min)
- Internal rotation first lost
Radiograph (LOSS)
- Loss of joint space
- Osteophytes
- Subchondral Sclerosis
- Subchondral cysts
Conservative (WIPE)
- Weight loss
- Injections (steroid)
- Physiotherapy
- Exercise and NSAIDs
Kellgren-Lawrence
- Grade 1: doubtful narrowing
- Grade 2: definite osteophytes
- Grade 3: definite narrowing
- Grade 4: bone on bone
THA Indications
- Failed conservative treatment
- Significant functional impairment
- Impact on quality of life
- Radiographic OA
Secondary Causes (DAFT)
- DDH (dysplasia)
- AVN
- FAI
- Trauma
Evidence Base and Key Studies
PROHIP: Total Hip Replacement vs Resistance Training for Severe Hip OA
- Multicentre RCT, 109 patients aged 50+ with severe hip OA and a surgical indication
- Oxford Hip Score improved 15.9 points with THA vs 4.5 with resistance training (difference 11.4, 95% CI 8.9 to 14.0, P less than 0.001) at 6 months
- 21% of the training group crossed over to THA by 6 months; 9% of surgical group had not had surgery
- Serious adverse events similar between groups, mostly known THA complications
How Long Does a Hip Replacement Last? Registry Meta-Analysis
- Systematic review and meta-analysis of case series plus AOANJRR and Finnish registry data (over 215,000 registry THAs)
- 25-year pooled survival was 77.6% from case series but only 57.9% from national registries
- Registry estimates regarded as less biased - about 58% of hip replacements last 25 years
- Case-series data systematically overestimate implant longevity
Intra-articular Triamcinolone vs Saline: Cartilage and Pain
- 2-year double-blind RCT, 140 patients with symptomatic knee OA and synovitis (40 mg triamcinolone every 12 weeks vs saline)
- Triamcinolone caused significantly greater cartilage volume loss (-0.21 vs -0.10 mm; difference -0.11 mm)
- No significant difference in pain between steroid and saline at 2 years
- Does not support repeated scheduled corticosteroid injection for symptomatic OA
Exercise for Osteoarthritis of the Hip (Cochrane Review)
- Meta-analysis of 10 RCTs (549-715 participants) of land-based exercise vs no exercise
- High-quality evidence: exercise reduced pain (SMD -0.38) and improved physical function (SMD -0.38)
- Benefit sustained for at least 3 to 6 months after stopping supervised treatment
- No clear effect on quality of life; adverse events rare and minor