Coronal Plane | Often Missed | Anatomic Reduction Essential | Posterior-to-Anterior Screws
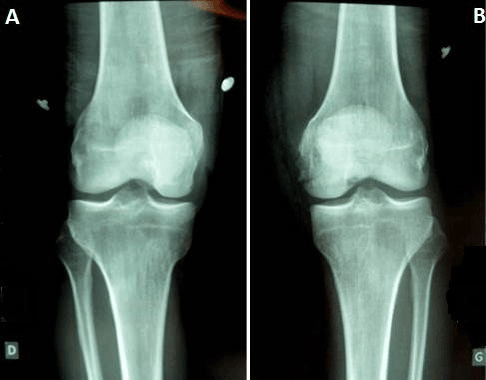
- Coronal plane fracture - often missed on AP and lateral X-rays
- Lateral condyle more commonly affected (2:1 ratio)
- Complete fractures are avascular - no soft tissue attachments
- Anatomic reduction essential - articular surface fracture
- Posterior-to-anterior lag screws are gold standard fixation
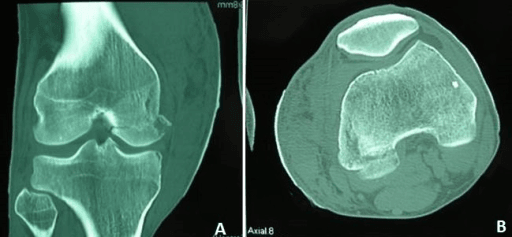
- “Look for sagittal CT - Hoffa often missed on plain films
- “Mechanism: direct blow to flexed knee or axial load
- “Gastrocnemius attachment may aid lateral fragment vascularity
- “Associated with high-energy trauma and other knee injuries
Frequently missed on plain radiographs because the coronal fracture plane may not be visible on AP or lateral views. CT is essential for diagnosis and surgical planning. Always suspect in high-energy distal femur trauma.
Complete Hoffa fragments have few soft tissue attachments beyond the posterior capsule and gastrocnemius origin, so they are relatively avascular. Anatomic reduction and stable fixation are critical to allow healing.
This is an articular fracture of the weight-bearing surface. Any step-off leads to post-traumatic arthritis. Anatomic reduction is non-negotiable. Assess under direct visualization.
Posterior-to-anterior lag screws are the standard fixation. They compress the fragment to the intact condyle. Countersink heads posteriorly to avoid impingement. Multiple screws provide better stability.
- Implication
- May be managed non-operatively if truly undisplaced
- Management
- Very close follow-up with CT, consider fixation
- Implication
- Will not heal, high risk of displacement
- Management
- Operative fixation required
- Implication
- Fix Hoffa first to restore condyle anatomy
- Management
- Then address supracondylar component
- Implication
- May need buttress plate
- Management
- Posterolateral or posteromedial approach
- Implication
- Emergent washout, staged fixation
- Management
- External fixation if soft tissue concerns
LATERALLATERAL - Why Lateral More Common
Hook:LATERAL condyle is more commonly affected - 2:1 ratio
SCREWSCREW - Fixation Principles
Hook:SCREW reminds you of the key fixation principles
Overview and Epidemiology
Hoffa fractures are coronal plane fractures of the posterior aspect of the femoral condyle. First described by Albert Hoffa in 1904, they are relatively rare but frequently missed injuries.
Mechanism of injury:
- Direct blow to flexed knee (dashboard injury)
- Axial load with knee in flexion
- Combined shear and compression forces
- Usually high-energy trauma
The fracture occurs in the coronal plane because of the loading mechanism. With the knee flexed, a direct blow or axial load creates shear forces that split off the posterior condyle. The coronal orientation is why it's easily missed on AP and lateral X-rays.
- Coronal-plane condylar fractures are rarer than sagittal-plane condylar fractures
- Male predominance; typically young adults
- High-energy trauma (motor vehicle and motorcycle collisions, falls)
- Lateral condyle is involved more often than the medial condyle
- May be isolated or associated with other injuries
- Supracondylar/intercondylar femur fractures (30-40%)
- ACL/PCL injuries
- Tibial plateau fractures
- Patellar fractures
- Neurovascular injury (rare)
Anatomy and Biomechanics
Femoral condyle anatomy:
The distal femur has two condyles that articulate with the tibia:
- Lateral Condyle
- More prominent
- Medial Condyle
- Less prominent
- Lateral Condyle
- Smaller area
- Medial Condyle
- Larger area
- Lateral Condyle
- Lateral gastrocnemius
- Medial Condyle
- Medial gastrocnemius
- Lateral Condyle
- More common (2:1)
- Medial Condyle
- Less common
Blumensaat line is the radiographic representation of the intercondylar roof. On lateral X-ray, it's a line along the roof of the intercondylar notch. The Letenneur classification uses this line to categorize Hoffa fractures.
Vascular considerations:
Complete Hoffa fragments are essentially avascular:
- No anterior soft tissue attachments
- No ligamentous attachments
- Only posterior periosteum/capsule
- Gastrocnemius attachment may provide some blood supply (especially lateral)
A complete Hoffa fragment is essentially avascular free bone. Unlike many fractures where periosteal blood supply aids healing, the Hoffa fragment relies entirely on the healing from the intact condyle after fixation. This emphasizes the importance of stable fixation and anatomic reduction.
- Posterior condyle is weight-bearing in flexion
- Malreduction leads to altered knee mechanics
- Any step-off causes accelerated arthritis
- Fragment may rotate or displace with knee motion
- Popliteal vessels (central, protected by fascia)
- Common peroneal nerve (lateral approach)
- Saphenous nerve (medial approach)
- Gastrocnemius muscle (retracted, not cut)
Classification Systems
Letenneur Classification (based on fracture line relative to Blumensaat line)
- Description
- Posterior to Blumensaat line
- Fragment Location
- Behind intercondylar roof
- Implications
- Posterior fragment only
- Description
- Crosses Blumensaat line
- Fragment Location
- Extends into weight-bearing
- Implications
- Larger fragment, more critical
- Description
- Oblique with smaller fragment
- Fragment Location
- Variable
- Implications
- May be more comminuted
Type II fractures involve more weight-bearing surface and may require more extensive fixation. Type III oblique fractures may have smaller fragments that are more challenging to fix.
LETENNEURLETENNEUR Classification
Hook:Types I-II-III: posterior only, crossing line, oblique small
Clinical Presentation and Assessment
History:
- Mechanism of injury (dashboard, direct blow, fall)
- High-energy vs low-energy
- Associated injuries
- Pre-injury function and activity level
Physical examination:
- Significance
- Hemarthrosis common
- Action
- Aspiration if tense
- Significance
- May localize Hoffa fracture
- Action
- Palpate both condyles
- Significance
- Expected finding
- Action
- Examine under anesthesia if needed
- Significance
- Associated ligament injury
- Action
- Document, may need staged repair
- Significance
- Open fracture
- Action
- Urgent washout, IV antibiotics
- Significance
- Vascular injury or compartment syndrome
- Action
- Urgent intervention
Key examination points:
- Palpate posterior condyles - may identify tenderness
- Assess ligamentous stability (may be limited by pain)
- Neurovascular examination - pulses, motor function, sensation
- Skin assessment - open wounds, abrasions, fracture blisters
- Compartment assessment if high-energy mechanism
Have a high index of suspicion for Hoffa fracture in any high-energy knee injury. The fracture is frequently missed on initial X-rays. If the mechanism is consistent (direct blow to flexed knee), order CT even if initial X-rays appear negative.
Investigations
- AP, lateral, and oblique views of knee
- Hoffa fracture may be subtle or invisible
- Look for double density sign on lateral view
- Measure fracture fragment size and displacement
- Coronal fracture line through posterior condyle
- Fragment may overlap with intact condyle on lateral
- Double density sign (superimposed condyle and fragment)
- Associated supracondylar fracture may be present
CT with 2D reconstructions is mandatory for all suspected Hoffa fractures. It defines fracture pattern, fragment size, displacement, comminution, and allows surgical planning. Plain radiographs alone are insufficient.
CT imaging:
- Thin-slice CT with sagittal and coronal reconstructions
- Assess fracture line orientation
- Measure fragment size as percentage of condyle
- Identify comminution
- Plan screw trajectory
MRI (if indicated):
- Not routine for Hoffa fractures
- May be helpful if ligament injury suspected
- Can assess cartilage damage
- Usually obtained after fracture healing if persistent symptoms
Key imaging findings to document:
- Significance
- Lateral vs medial
- Impact on Surgery
- Determines approach
- Significance
- Percentage of condyle
- Impact on Surgery
- Fixation method
- Significance
- Articular step-off
- Impact on Surgery
- Urgency of fixation
- Significance
- Multiple fragments
- Impact on Surgery
- May need plate
- Significance
- Supracondylar component
- Impact on Surgery
- Surgical sequence
Differential diagnosis of the acutely painful, swollen knee after distal femoral trauma:
- Distinguishing features
- Coronal-plane line through posterior condyle, often invisible on AP, tangential on lateral; lateral more common
- Key investigation
- CT with sagittal and coronal reconstructions
- Distinguishing features
- Vertical split visible on the AP view; far more common than coronal pattern
- Key investigation
- AP radiograph, confirmed on CT
- Distinguishing features
- Metaphyseal or T/Y articular pattern; may harbour an occult coexisting Hoffa fragment
- Key investigation
- CT to exclude a coronal component
- Distinguishing features
- Tibial-side bony injury, often with ligamentous instability
- Key investigation
- CT plus stress or MRI assessment
- Distinguishing features
- No fracture line; positive laxity tests once pain settles
- Key investigation
- MRI if radiographs and CT are normal
Management

- Truly undisplaced fractures (rare)
- Non-ambulatory patients
- Severe medical comorbidities precluding surgery
- Patient refusal of surgery
- Long leg cast or hinged knee brace
- Non-weight bearing for 6-8 weeks
- Very close follow-up with serial imaging
- CT at 2-4 weeks to assess displacement
- Low threshold for surgery if any displacement
Non-operative management carries high risk of secondary displacement. The posterior condyle bears load during knee flexion, and the fracture fragment has no soft tissue attachments to maintain position. Most surgeons favor operative fixation for all Hoffa fractures.
Surgical Technique
- Supine with bump under ipsilateral hip
- Knee flexed to 20-30 degrees over bolster
- Leg free for intraoperative flexion/extension
- Tourniquet optional
- Incision along distal IT band to lateral epicondyle
- Develop interval between IT band and biceps
- Incise lateral capsule to expose condyle
- Protect common peroneal nerve posteriorly
- Incision posterior to lateral epicondyle
- Identify and protect peroneal nerve
- Split lateral gastrocnemius if needed
- Excellent access to posterior condyle
The posterolateral approach provides direct visualization of the posterior condyle and is often preferred for Hoffa fractures.
Lag screws compress the fragment but do not neutralise shear, and the decision to add a plate is driven by the Letenneur fracture geometry. Types I and III have a near-vertical fracture line — the load across the condyle is largely shear, the fragment tends to slide proximally, and lag screws alone may fail — whereas type II is more transverse and is well controlled by interfragmentary lag screws alone. For the vertical types, a small posterior buttress (antiglide) plate applied along the posterior cortex converts shear into compression and resists proximal migration of the fragment, the same antiglide principle used for posterior malleolar and proximal-ulna fractures. A buttress plate is also added for comminution. The plate sits posteriorly (requiring posterior access) while lag screws provide interfragmentary compression.
The approach must deliver what the construct needs. A standard lateral or anterolateral (e.g. Swashbuckler) approach gives good articular visualisation and easily permits anterior-to-posterior or oblique screws, but it does NOT allow a true posterior-to-anterior screw or a posterior buttress plate. To place the biomechanically preferred P-A lag screws and a posterior antiglide plate, a dedicated posterior approach is required: a posterolateral approach (protecting the common peroneal nerve) for the lateral condyle, a posteromedial approach (protecting the saphenous nerve and vessels) for the medial condyle, or a direct posterior (Lobenhoffer) approach for posterior or bicondylar fragments, with lateral or prone positioning planned accordingly. The logic runs one way: decide whether the fracture geometry needs a posterior buttress, then let that decision drive the approach and patient position.
Complications
- Incidence
- 10-20%
- Prevention/Management
- Anatomic reduction, stable fixation, avoid smoking
- Incidence
- Variable
- Prevention/Management
- Anatomic reduction at surgery, confirm with fluoro
- Incidence
- 20-30%
- Prevention/Management
- Anatomic reduction, no step-off acceptable
- Incidence
- Rare if fixed
- Prevention/Management
- Stable fixation allows revascularization
- Incidence
- 15-25%
- Prevention/Management
- Early ROM, physiotherapy
- Incidence
- 1-5%
- Prevention/Management
- Antibiotic prophylaxis, atraumatic technique
- Incidence
- Variable
- Prevention/Management
- Countersink screws, consider removal later
- Major concern due to avascular fragment
- Risk factors: inadequate fixation, smoking, displacement
- Treatment: revision fixation with bone graft
- May require plate fixation if screws failed
- Leads to altered knee mechanics
- Even small step-off causes cartilage wear
- Prevention is key - confirm reduction intraoperatively
- Correction requires osteotomy (difficult)
Nonunion is a significant concern because the Hoffa fragment is essentially avascular. Prevention requires stable fixation with good compression, anatomic reduction, and patient optimization (smoking cessation). If nonunion occurs, revision with bone grafting may be needed.
Post-traumatic arthritis:
- Occurs in 20-30% despite good treatment
- Related to cartilage damage at injury
- Malreduction increases risk
- May require arthroplasty in severe cases
Postoperative Care and Rehabilitation
Postoperative protocol:
- Knee immobilizer for comfort
- Toe-touch weight bearing with crutches
- Ice, elevation, wound care
- Gentle ROM exercises as pain allows
- CPM machine optional
- Progressive ROM (goal: 0-90 degrees by week 4)
- Continue partial weight bearing (25-50% body weight)
- Quadriceps strengthening (isometrics, SLR)
- Stationary bike when ROM allows
- Pool exercises if incisions healed
- Radiographic assessment of healing
- Progressive weight bearing based on healing
- Full weight bearing typically by 8-12 weeks
- Aggressive ROM (goal: full ROM by 12 weeks)
- Progressive strengthening
- Full activity as tolerated
- Sport-specific training
- May require ongoing physiotherapy
- Hardware removal if symptomatic
Key rehabilitation principles:
- Early motion prevents stiffness
- Delayed weight bearing protects fixation
- Monitor for loss of reduction
- Individualize based on fixation stability
- Long-term follow-up for arthritis development
Delay full weight bearing until radiographic evidence of healing (typically 8-12 weeks). The posterior condyle bears load in knee flexion, stressing the fixation. Premature weight bearing may lead to loss of reduction or nonunion.
Outcomes and Prognosis
Outcome factors:
- Better Outcomes
- Anatomic
- Worse Outcomes
- Any step-off
- Better Outcomes
- Stable, multiple screws
- Worse Outcomes
- Unstable, single screw
- Better Outcomes
- Isolated Hoffa
- Worse Outcomes
- Combined patterns
- Better Outcomes
- Non-smoker, young
- Worse Outcomes
- Smoker, elderly
- Better Outcomes
- Larger
- Worse Outcomes
- Small/comminuted
The key to good outcomes is anatomic reduction and stable fixation. Any articular step-off leads to accelerated arthritis. Stable fixation allows early motion which prevents stiffness while protecting healing.
Long-term concerns:
- Post-traumatic arthritis (may develop years later)
- Stiffness (usually manageable with physiotherapy)
- Hardware prominence (may need removal)
- Functional limitations in high-demand activities
Guidelines, Registries & Global Practice
Global epidemiology:
- Global picture
- Coronal-plane condylar (Hoffa) fractures are rarer than sagittal-plane condylar fractures
- Source
- Zhou 2019 systematic review
- Global picture
- Lateral more frequent than medial; lateral fractures have a more vertical line over the weight-bearing zone
- Source
- Rabelo 2023 systematic review
- Global picture
- Male predominance, typically young adults
- Source
- Onay 2017; Zhou 2019
- Global picture
- Predominantly high-energy (road traffic and motorcycle collisions, falls); low-energy and iatrogenic cases also reported
- Source
- Zhou 2019
- Global picture
- Post-traumatic osteoarthritis in roughly half of a small surgically treated series (7 of 13)
- Source
- Onay 2017
Guideline and consensus position (there is no dedicated single-society Hoffa guideline):
- Position relevant to Hoffa fractures
- Classifies as a partial articular coronal fracture of the distal femur (AO/OTA 33-B3). Recommends anatomic articular reduction and absolute stability with interfragmentary lag screws, plus a buttress/antiglide plate when comminuted
- Evidence level
- Expert/principle-based
- Position relevant to Hoffa fractures
- CT mandatory for articular distal femur fractures; fix displaced articular fragments; fix the coronal (Hoffa) fragment before the metaphyseal component
- Evidence level
- Consensus, Level IV-V
- Position relevant to Hoffa fractures
- Generic complex articular fracture principles: CT for intra-articular involvement, senior decision-making, fixation that permits early movement
- Evidence level
- Guideline (indirect)
- Position relevant to Hoffa fractures
- Endorses posterior-to-anterior screw orientation with posterior buttress plating for unstable patterns
- Evidence level
- Consensus, Level IV
The recommendations converge: there is broad international agreement on CT diagnosis, anatomic reduction, lag-screw fixation and fixing the Hoffa fragment first in combined injuries.
Registry evidence:
- There is no joint or fracture registry that tracks Hoffa fractures specifically; major registries (NJR, AJRR, AOANJRR, SHAR, Norwegian, NZJR) capture arthroplasty, not coronal condylar fixation. Evidence therefore rests on systematic reviews and single-centre series.
Practice variation:
- Variation
- Posterior-to-anterior (biomechanically favoured) versus anterior-to-posterior (familiar approach, lower neurovascular risk)
- Reason
- Surgeon familiarity and approach choice; Rabelo 2023
- Variation
- Headless compression versus headed cannulated lag screws
- Reason
- Headless reduce prominence and implant failure; Maheshwari 2018
- Variation
- Added for Letenneur I and III and comminuted patterns; omitted for simple osteochondral type II
- Reason
- Fracture geometry; Rabelo 2023
- Variation
- High-resource centres use CT routinely and complex posterior approaches; limited-resource settings rely more on radiographs, increasing the missed-fracture and nonunion burden
- Reason
- Imaging access
In any orthopaedic exam, be prepared to discuss why Hoffa fractures are missed (coronal plane poorly seen on AP and lateral X-rays), the mandatory role of CT, the AO/OTA 33-B3 designation, and the technical aspects of fixation (posterior-to-anterior lag screws, at least two screws, countersinking, buttress plate for comminution). Also know the sequence for combined injuries: fix the Hoffa fragment first.
MCQ Practice Points
Q: What is a Hoffa fracture? A: A coronal plane fracture of the posterior femoral condyle. The fracture line runs in the coronal plane, separating the posterior condyle from the anterior condyle and shaft.
Q: Why are Hoffa fractures frequently missed on plain X-rays? A: The fracture occurs in the coronal plane, which is parallel to the X-ray beam on AP view and tangential on lateral view. CT with sagittal reconstructions is required for diagnosis.
Q: Why is the Hoffa fragment essentially avascular? A: The fragment has no anterior soft tissue attachments (capsule, ligaments) and only posterior periosteum. It is essentially a free bone fragment relying on fixation-mediated healing.
Q: Why should screws be placed posterior-to-anterior in Hoffa fracture fixation? A: P-A screw placement puts the threads in the well-vascularized intact bone rather than the avascular fragment, providing better purchase. The screw heads are also easier to countersink posteriorly.
Q: In a combined Hoffa and supracondylar fracture, which component should be fixed first? A: Fix the Hoffa fracture first. This reconstitutes the condyle anatomy, creating a solid block to which the shaft can then be reduced and fixed.
HOFFAHOFFA - Key Points
Hook:HOFFA reminds you this is Hidden, needs ORIF, involves Femoral condyle, Fixed P-A, and is Avascular
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old man presents to ED after a motorcycle accident. Initial knee X-rays were reported as normal, but he has significant pain and cannot bear weight. You examine him 2 days later in fracture clinic. What is your approach?”
“CT scan of a 50-year-old woman after MVA shows a distal femur fracture with both a supracondylar component and a Hoffa fracture of the lateral condyle. How do you approach this complex injury?”
“A patient presents 6 months after Hoffa fracture fixation with persistent pain and CT showing nonunion. The original fixation was with a single 6.5mm screw. What is your management?”
DEFINITION AND KEY POINTS
- Coronal plane fracture of posterior femoral condyle
- Frequently missed on initial X-rays - CT essential
- Lateral condyle more common (2:1 ratio)
- Complete fragments are avascular
CLASSIFICATION
- Letenneur Type I: Posterior to Blumensaat line
- Letenneur Type II: Crosses Blumensaat line (weight-bearing)
- Letenneur Type III: Oblique with smaller fragment
- Also classified by condyle: lateral, medial, or bicondylar
SURGICAL PRINCIPLES
- Anatomic reduction is essential (articular fracture)
- Posterior-to-anterior lag screws (gold standard)
- Minimum 2 screws for rotational control
- Countersink screw heads posteriorly
COMBINED INJURIES
- Fix Hoffa FIRST to reconstitute condyle
- Then fix supracondylar component
- Lateral locked plate or retrograde nail for metaphysis
- May need combined approaches for bicondylar
COMPLICATIONS
- Nonunion (10-20%) - due to avascular fragment
- Malunion - any step-off causes arthritis
- Post-traumatic arthritis (20-30%)
- Stiffness (15-25%)
TRAPS AND PEARLS
- High-energy knee + normal X-rays = get CT
- Single screw fixation is insufficient
- A-P screws are inferior to P-A
- Early motion, delayed weight bearing
- Anatomic reduction is non-negotiable
Evidence Base
- 113 studies synthesised. Lateral coronal-plane fractures are more frequent than medial, have a more vertical fracture line and concentrate on the weight-bearing zone. The Letenneur system is the most widely used classification. Posterior-to-anterior lag screws (with a posterior buttress plate for Letenneur types I and III) are biomechanically more efficient than anterior-to-posterior fixation; no consensus exists on screw number or diameter.
- 105 articles reviewed. Coronal-plane condylar fractures are rarer than sagittal-plane fractures and usually follow high-energy trauma. Letenneur, CT-based, AO and modified-AO classifications are all in use. Radiographs may be negative in questionable cases, so CT and MRI should be obtained. Non-displaced fractures carry a high risk of redisplacement, so open reduction and internal fixation is preferred with headless compression screws inserted perpendicular to the fracture line from posterior to anterior.
- 13 surgically treated isolated coronal-plane condylar fractures, mean follow-up 93 months. All united (mean 10 weeks). Post-traumatic osteoarthritis developed in 7 of 13 (54%) and avascular necrosis in 2 of 13 (15.4%). Medial Hoffa fractures had worse functional scores (mean KSS 66.5) than lateral fractures (mean KSS 83.8). Fractures may be overlooked if imaging is not scrutinised.
- 32 isolated Hoffa fractures fixed with cancellous lag screws and/or antiglide plate (lateral approach for lateral, medial for medial). All united at a mean of 11.6 weeks with no subsequent displacement, fixation failure, arthritis or avascular necrosis. Mean Knee Society Score 83.2 and mean IKDC 81.6; knee stiffness in 4 patients.
- 30 coronal-plane condylar fractures randomised between headless compression screws and cannulated cancellous (headed) screws. Good Neer outcomes in 13 of 15 (86.7%) headless versus 10 of 15 (66.7%) headed. Range of motion did not differ, but complications and implant failure were significantly higher with headed cancellous screws.
- 12 lateral Hoffa nonunions, frequently the sequel of a missed acute fracture, treated at a tertiary referral centre. All 12 united (one after re-fixation); loss of reduction 7.7% and post-traumatic arthrosis 7.7%. Mean final knee flexion 104.5 degrees with significant range-of-motion improvement.