Non-Operative Success Rate High | Radial Nerve at Risk | Functional Bracing Gold Standard
- Functional bracing achieves over 90% union with acceptable alignment in most cases
- Radial nerve spirals around posterior humerus - vulnerable at junction of middle and distal thirds
- Holstein-Lewis fracture: Distal third spiral fracture with high radial nerve palsy risk
- Acceptable alignment: under 20° anterior angulation, under 30° varus/valgus, less than 3cm shortening, under 15° rotation
- Primary radial nerve palsy (at injury): observe 3-4 months before exploration
- “70% of radial nerve palsies recover spontaneously without exploration
- “Secondary palsy after manipulation = urgent exploration
- “Pendulum exercises begin immediately with functional brace
- “Antegrade IMN avoids radial nerve but risks rotator cuff injury
Document wrist/finger extension and sensation before any manipulation. Primary palsy = observe, Secondary palsy post-manipulation = explore. Nerve crosses posterior humerus at spiral groove.
Gold standard non-operative management. Humeral brace with adjustable straps. Allows elbow and shoulder motion. Gravity alignment maintains reduction.
Polytrauma, open fractures, vascular injury, floating elbow, bilateral fractures, pathological fractures. Also consider for unacceptable alignment and patient factors (obesity).
ORIF with plate vs IMN. Plates preferred for distal fractures (avoid rotator cuff). IMN for proximal/middle shaft. MIPO technique reduces iatrogenic nerve injury.
Overview and Epidemiology
Humeral shaft fractures are unique in that non-operative management achieves excellent outcomes in the majority of cases. The shoulder and elbow joints compensate well for residual angulation and shortening, making functional bracing the gold standard treatment.
- Bimodal distribution: Young males (high-energy), elderly females (low-energy falls)
- Male predominance in working age (sports, MVA)
- Female predominance in elderly (osteoporotic)
- Mean age: 45-55 years
- Direct blow: Transverse fractures (50%)
- Indirect/Torsion: Spiral/oblique fractures (50%)
- Falls (most common overall)
- Motor vehicle accidents
- Sports (throwing, arm wrestling)
- Frequency
- 30%
- Common Pattern
- Spiral/Oblique
- Nerve at Risk
- Axillary nerve (rare)
- Frequency
- 60%
- Common Pattern
- Transverse/Spiral
- Nerve at Risk
- Radial nerve (spiral groove)
- Frequency
- 10%
- Common Pattern
- Spiral (Holstein-Lewis)
- Nerve at Risk
- Radial nerve (highest risk)
Anatomy and Pathophysiology
The radial nerve is the most commonly injured nerve in humeral shaft fractures. It enters the posterior compartment from medial to lateral, wrapping around the posterior humerus in the spiral groove at the junction of the middle and distal thirds. Here it is tethered by the lateral intermuscular septum.

- Proximal Fragment
- Abduction, ER (rotator cuff)
- Distal Fragment
- Adduction (pec major, deltoid)
- Resulting Deformity
- Apex lateral angulation
- Proximal Fragment
- Adduction (pec major)
- Distal Fragment
- Abduction (deltoid)
- Resulting Deformity
- Apex medial angulation
- Proximal Fragment
- Abduction (deltoid)
- Distal Fragment
- Proximal pull (biceps, triceps)
- Resulting Deformity
- Shortening, variable angulation
- Surgical neck: Transition to shaft (axillary nerve)
- Deltoid insertion: V-shaped, mid-shaft lateral
- Spiral groove: Posterior, middle-distal junction
- Supracondylar ridge: Transition to distal humerus
- Enters arm in axilla (posterior cord)
- Supplies triceps proximally
- Spiral groove: 14-20cm from lateral epicondyle
- Pierces lateral intermuscular septum at distal third
- Divides into PIN and superficial radial at elbow
The radial nerve supplies the triceps before entering the spiral groove. Therefore, triceps function may be preserved despite radial nerve injury at the spiral groove level. Always test wrist and finger extension - these are the key clinical findings for radial nerve palsy.
Classification Systems
AO/OTA Classification (12-A/B/C)
- Description
- Two fragments, over 90% cortical contact
- Subgroups
- A1: Spiral, A2: Oblique (over 30°), A3: Transverse (under 30°)
- Treatment Tendency
- Functional bracing
- Description
- Three fragments, contact between main fragments possible
- Subgroups
- B1: Spiral wedge, B2: Bending wedge, B3: Fragmentary wedge
- Treatment Tendency
- Bracing or surgery
- Description
- Multiple fragments, no contact between main fragments
- Subgroups
- C1: Spiral, C2: Segmental, C3: Irregular comminuted
- Treatment Tendency
- Usually surgical
AO/OTA classification determines complexity and comminution. Simple fractures (A) have excellent outcomes with functional bracing. Complex fractures (C) often require surgical stabilization.
Clinical Assessment
- Mechanism: Direct blow vs torsion vs fall
- Hand dominance: Functional implications
- Occupation: Manual vs sedentary work
- Comorbidities: Diabetes, smoking, osteoporosis
- Previous injury: Pathological fracture concern
- Look: Deformity, swelling, bruising, skin condition
- Feel: Point tenderness, crepitus, neurovascular status
- Move: Limited by pain, test shoulder and elbow
- Neurovascular: Radial nerve critical, brachial artery
Document radial nerve function before and after any intervention. Test: wrist extension against gravity, finger MCP extension, thumb extension (hitchhiker), sensation first dorsal web space. Record in notes clearly.
- Technique
- Extend wrist against resistance
- Finding
- Wrist drop if absent
- Interpretation
- Radial nerve palsy - most reliable sign
- Technique
- Extend fingers at MCP against resistance
- Finding
- Cannot extend MCPs
- Interpretation
- PIN involvement
- Technique
- Extend thumb (hitchhiker sign)
- Finding
- Cannot extend thumb
- Interpretation
- EPL - PIN involvement
- Technique
- Light touch dorsal first web
- Finding
- Numbness/decreased
- Interpretation
- Superficial radial nerve
- Technique
- Extend elbow against resistance
- Finding
- Usually preserved
- Interpretation
- Branches given before spiral groove
Primary palsy (present at injury): Usually neurapraxia from stretch/contusion. Observe for 3-4 months - 70% recover spontaneously. Secondary palsy (develops after manipulation/reduction): Suggests nerve entrapment in fracture site - warrants urgent exploration.
- Distinguishing Features
- Mid-arm deformity, crepitus, abnormal mobility; possible wrist drop
- Key Investigation
- AP/lateral humerus including shoulder and elbow
- Pitfall to Avoid
- Missing associated radial nerve palsy by not testing wrist extension
- Distinguishing Features
- Low-energy mechanism, antecedent arm pain, known malignancy, lytic lesion
- Key Investigation
- Radiographs +/- CT/MRI, bloods, staging if primary unknown
- Pitfall to Avoid
- Treating as simple trauma and missing underlying tumour or myeloma
- Distinguishing Features
- Pain and deformity localised to shoulder, not mid-arm; axillary nerve at risk
- Key Investigation
- Shoulder AP and axillary/scapular-Y views
- Pitfall to Avoid
- Mislabelling a surgical-neck fracture as a shaft fracture
- Distinguishing Features
- Elbow-centred pain, articular involvement, possible ulnar nerve signs
- Key Investigation
- CT for articular extension
- Pitfall to Avoid
- Underestimating articular involvement on plain films
- Distinguishing Features
- Wrist drop without bony injury (e.g. Saturday-night palsy, penetrating wound)
- Key Investigation
- Nerve conduction studies, ultrasound/MRI of nerve
- Pitfall to Avoid
- Attributing wrist drop to a fracture that is not present
- Distinguishing Features
- Fever, systemic upset, atraumatic or trivial trauma, raised inflammatory markers
- Key Investigation
- Bloods (CRP, WCC), MRI, aspiration
- Pitfall to Avoid
- Plating through occult infection
Investigations
Imaging Protocol
AP and lateral of entire humerus. Must include shoulder and elbow joints. Assess fracture pattern, displacement, angulation, and any articular involvement.
Include shoulder and elbow joints on separate views if not fully visualized. Rule out associated injuries (floating elbow, shoulder dislocation).
Indicated for: articular extension, preoperative planning for comminuted fractures, pathological fracture workup.
MRI: pathological fracture evaluation, soft tissue injury. Angiography: if vascular injury suspected (rare).
- What to Assess
- Simple vs comminuted
- Normal/Acceptable
- Simple preferred for bracing
- Action if Abnormal
- Comminuted may need surgery
- What to Assess
- AP view
- Normal/Acceptable
- less than 20 degrees
- Action if Abnormal
- Reduction needed if over 20°
- What to Assess
- Lateral view
- Normal/Acceptable
- less than 30 degrees
- Action if Abnormal
- Reduction needed if over 30°
- What to Assess
- Compare with normal
- Normal/Acceptable
- less than 3cm
- Action if Abnormal
- Usually acceptable
- What to Assess
- Shoulder and elbow
- Normal/Acceptable
- None
- Action if Abnormal
- CT if suspected
Look specifically for distal third spiral oblique fracture pattern on radiographs. This is the Holstein-Lewis fracture with high radial nerve palsy risk. Even with intact nerve function, consider lower threshold for surgical intervention.


At a Glance Treatment Decision Guide
- Nerve Status
- Intact
- Key Factor
- Compliant patient
- Treatment
- Functional brace - gold standard
- Nerve Status
- Primary radial palsy
- Key Factor
- Closed injury
- Treatment
- Functional brace + observe nerve 3-4 months
- Nerve Status
- Secondary palsy post-manipulation
- Key Factor
- New deficit after reduction
- Treatment
- Urgent ORIF + nerve exploration
- Nerve Status
- With or without palsy
- Key Factor
- High nerve risk location
- Treatment
- Strong consideration for ORIF
- Nerve Status
- Any status
- Key Factor
- Associated injuries
- Treatment
- ORIF or IMN mandatory
Management Algorithm
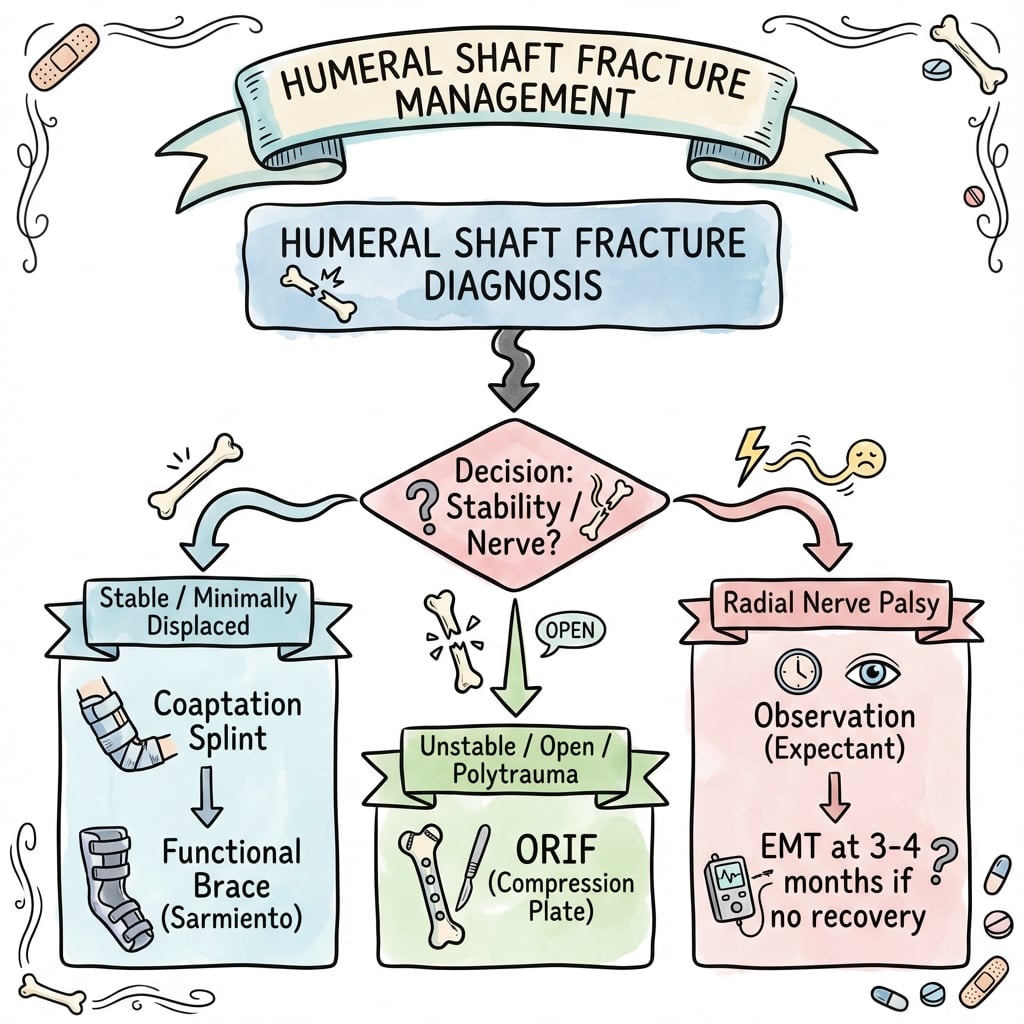
Non-Operative Management - Functional Bracing
Gold standard for most humeral shaft fractures. Pioneered by Sarmiento, achieves over 90% union rate.
Functional Bracing Protocol
Coaptation splint (sugar tong) or U-slab. Sling for comfort. Ice, elevation. Begin pendulum exercises immediately if pain allows.
Convert to prefabricated humeral brace once swelling subsides. Circumferential compression with adjustable straps. Allows elbow and shoulder motion.
Active shoulder and elbow ROM. Pendulum exercises 4-6 times daily. Gravity alignment maintains reduction. Wean sling.
Weekly X-rays initially to ensure maintained alignment. Then every 2-4 weeks until union (usually 8-12 weeks).
Wean brace once clinical and radiographic union. Progressive strengthening. Full activity by 4-6 months.
The brace provides hydraulic compression via soft tissue containment. This, combined with gravity, aligns the fracture. The key is early motion - muscle contraction maintains alignment and promotes healing.
- Compliant patient
- Simple fracture pattern
- Acceptable initial alignment
- Early active motion
- Weekly X-ray follow-up initially
- Obesity (poor soft tissue compression)
- Skin problems (burns, dermatitis)
- Non-compliance
- Transverse fractures at narrow isthmus
- Segmental fractures
The humerus is the second most common long bone for skeletal metastases (after the femur), so "pathological fracture" appears in the indication list - but the examinable decision-making behind it is distinct from a normal trauma fracture.
Impending fracture (still intact bone with a destructive lesion) - quantify the risk with the Mirels score (1 to 3 points each for: site, pain, lesion type lytic/blastic/mixed, and size as a fraction of cortical diameter):
- Score 9 or more = prophylactic fixation before it breaks (a fixed bone is far easier than a pathological fracture, and avoids the morbidity of a sudden break).
- Score 7 or less = radiotherapy and surveillance; 8 is borderline and individualised.
- Functional bracing's usual forgiveness does not apply: tumour bone will not unite, so the goal is durable mechanical stability for the patient's remaining life, not union.
Implant choice for diaphyseal disease differs from trauma:
- A long intramedullary nail spanning the whole bone is often preferred for diaphyseal metastases - it protects the entire humerus against further lesions and allows immediate load-bearing, unlike a plate that protects only the fracture.
- Plate plus cement (PMMA) is an alternative where a nail is unsuitable or for periarticular lesions, filling the defect for immediate stability.
- Always biopsy/confirm the diagnosis before fixing an unknown solitary lesion (it may be a primary sarcoma where a nail would contaminate the whole bone), and give postoperative radiotherapy to the construct to control local tumour.
Exam point: for a humeral lesion, score the impending fracture with Mirels (fix if 9 or more, irradiate if 7 or less); for diaphyseal metastatic disease favour a long IMN spanning the whole bone plus postoperative radiotherapy, and biopsy an unknown solitary lesion before fixation to avoid seeding a primary sarcoma.
Surgical Technique
Open Reduction Internal Fixation - Plating

- Supine with arm on arm board (anterolateral approach)
- Lateral decubitus or prone for posterior approach
- Beach chair for proximal fractures
- Incision along lateral border of biceps
- Develop interval between brachialis (musculocutaneous) and brachioradialis (radial)
- Radial nerve runs between these muscles - identify and protect
- Plate applied anterolaterally on flat humerus
- Midline posterior incision
- Split triceps in midline or elevate medial and lateral heads
- Radial nerve identified in spiral groove, protected
- Plate applied to flat posterior surface
- 4.5mm narrow LCP or broad LCP
- Minimum 3-4 screws (6-8 cortices) each side of fracture
- Compression plate for simple patterns
- Bridge plating for comminution
Minimally Invasive Plate Osteosynthesis uses small incisions proximally and distally with submuscular plate passage. Reduces soft tissue stripping and theoretical nerve injury risk. Requires fluoroscopy.

Complications
- Incidence
- 12-18% (primary)
- Risk Factors
- Distal third, spiral, Holstein-Lewis
- Management
- Observe primary, explore secondary
- Incidence
- 2-10%
- Risk Factors
- Transverse pattern, distraction, non-compliance
- Management
- ORIF + bone graft
- Incidence
- Variable
- Risk Factors
- Non-operative with poor follow-up
- Management
- Usually well tolerated, osteotomy if symptomatic
- Incidence
- Common initially
- Risk Factors
- Prolonged immobilization, poor compliance
- Management
- Early motion, physiotherapy
- Incidence
- 1-3%
- Risk Factors
- Open fractures, poor soft tissues
- Management
- Debridement, antibiotics, revision
- Incidence
- 2-5%
- Risk Factors
- Early loading, inadequate fixation
- Management
- Revision fixation
- Incidence
- 2-5% (surgical)
- Risk Factors
- Posterior approach, ORIF
- Management
- Careful dissection, MIPO technique
Radial Nerve Palsy Management
Primary palsy (at injury): 70% recover spontaneously. Observe for 3-4 months with clinical and EMG monitoring. If no recovery by 4 months, explore. Secondary palsy (post-manipulation): Urgent exploration - nerve likely trapped in fracture site.
- Primary Palsy
- Present at injury
- Secondary Palsy
- Develops after manipulation/surgery
- Primary Palsy
- Stretch/contusion (neurapraxia)
- Secondary Palsy
- Entrapment in fracture site
- Primary Palsy
- 70% within 3-4 months
- Secondary Palsy
- Unlikely without exploration
- Primary Palsy
- Observe, wrist splint, EMG at 3-4 weeks
- Secondary Palsy
- Urgent surgical exploration
Management of Primary Radial Nerve Palsy
Document findings clearly. Wrist cock-up splint to maintain function. Proceed with non-operative management if otherwise indicated.
Baseline EMG/NCS to confirm nerve injury type and level. Monitor clinically for Tinel sign progression (sign of regeneration).
Repeat EMG if no clinical recovery. Look for reinnervation potentials. Continue monitoring.
If no clinical or EMG recovery, plan surgical exploration. Nerve grafting may be required if gap identified.
If nerve recovery incomplete, consider tendon transfers (PT to ECRB, FCR to EDC, PL to EPL).
If radial nerve does not recover: PT to ECRB (wrist extension), FCR to EDC (finger extension), PL to EPL (thumb extension). These restore functional wrist and finger extension.
Transverse fracture pattern has higher nonunion risk with functional bracing (2-10% vs 5% or less for oblique/spiral). The narrow isthmus and transverse orientation provide poor cortical contact. Consider primary ORIF for transverse fractures at the narrow diaphyseal portion.
The topic notes transverse fractures unite less reliably, but the higher-order skill is predicting nonunion early so a brace can be converted to fixation before a stiff, atrophic nonunion develops (which then needs plating plus bone graft).
Validated risk factors for humeral shaft nonunion (cluster these mentally):
- Fracture features: transverse pattern, a fracture gap or distraction (often from an over-heavy cast/brace or interposed soft tissue), proximal-third location, and high comminution.
- Biology/host: smoking, diabetes, obesity, advanced age, alcohol, NSAID use, and any over-distraction.
Early radiographic and clinical warning signs at the 6 to 12 week reviews:
- Absence of bridging callus by about 6 to 8 weeks in a fracture that should be forming it.
- Persistent fracture-site motion or pain on clinical stressing once early union would be expected.
- A visible or widening fracture gap on serial films - distraction is the single most correctable cause, addressed by adjusting the brace to allow gravity to close the gap.
Acting on it: the at-risk fracture is recognised early and managed by correcting distraction first; if there is still no callus and ongoing motion by around 12 weeks, early conversion to compression plating (with bone graft for atrophic patterns) gives better, faster results than waiting many months for an established nonunion. This is also the practical message of the operative-versus-bracing trials (e.g. the FISH and Matsunaga RCTs): early fixation does not improve final function much but markedly reduces nonunion and secondary reintervention.
Exam point: nonunion is predicted, not just diagnosed - transverse pattern, a distraction gap, proximal-third location and poor host biology flag the at-risk fracture; absent callus plus persistent motion by 6 to 12 weeks should trigger correction of distraction and, if it persists, early conversion to compression plating rather than prolonged bracing.

Pendulum exercises from day one are critical. The key to successful functional bracing is EARLY MOTION. Shoulder stiffness is a preventable complication with appropriate rehabilitation.
Postoperative Care and Rehabilitation
Post-ORIF Rehabilitation
Sling for comfort. Wound care. Gentle pendulum exercises. No active shoulder elevation against gravity.
Active-assisted shoulder ROM. Active elbow ROM. Gentle strengthening begins at 4 weeks if stable fixation.
Progressive resistive exercises. Wean sling. Radiographic union usually evident by 8-12 weeks.
Full activity when clinically and radiographically healed. Sport-specific training as appropriate.
Outcomes and Prognosis
- Impact
- Significant
- Notes
- Simple patterns do well with bracing; transverse at risk
- Impact
- Critical for bracing
- Notes
- Non-compliance leads to malunion/nonunion
- Impact
- Important
- Notes
- Primary palsy usually recovers; secondary needs surgery
- Impact
- Variable
- Notes
- Polytrauma patients may need surgical fixation
- Impact
- Negative
- Notes
- Higher nonunion rates
- Impact
- Negative
- Notes
- Delayed healing, higher complications
Meta-analyses show similar union rates for plate vs nail (both over 95%). However, plating has lower reoperation rates and less shoulder problems. Nailing is faster but associated with more shoulder pain (antegrade) or elbow issues (retrograde).
Guidelines, Registries & Global Practice
Global Epidemiology
- Population
- Sweden, adults
- Humeral Shaft Incidence
- 13.4
- Key Pattern
- 13% of all humeral fractures; F:M 2.4:1; mean age 66.8
- Population
- Western Europe
- Humeral Shaft Incidence
- Approximately 13-20
- Key Pattern
- Bimodal: young males high-energy, elderly females low-energy falls
- Population
- Global
- Humeral Shaft Incidence
- Approximately 1-3% of all fractures
- Key Pattern
- Most are closed, low-energy, isolated injuries
The Swedish Fracture Register (Bergdahl et al, BMC Musculoskelet Disord 2016) provides the cleanest contemporary denominator: humeral shaft fractures occur at 13.4 per 100,000 person-years, are predominantly low-energy falls in older women (F:M 2.4:1), and make up about 13% of all humeral fractures. Only ~1% are open.
Guideline & Registry Landscape
- Position on Humeral Shaft Fractures
- Functional bracing remains a reasonable default for most closed isolated fractures; surgery for absolute indications and selected relative ones. AO principles guide implant choice (plate for distal/articular, nail or plate for mid-shaft)
- Evidence Basis
- Synthesis of RCTs and meta-analyses (Level I-II)
- Position on Humeral Shaft Fractures
- Emphasis on documented neurovascular assessment, early senior decision-making, and shared decision-making between bracing and fixation; no mandate for routine surgery
- Evidence Basis
- Consensus standards informed by RCT evidence
- Position on Humeral Shaft Fractures
- Bracing and operative fixation both endorsed; growing interest in primary fixation to reduce nonunion and shorten disability in selected adults
- Evidence Basis
- Level I RCT and meta-analysis data
- Position on Humeral Shaft Fractures
- Competency expected in both non-operative and operative management; mandatory documentation of radial nerve status; informed consent must include nerve-injury discussion
- Evidence Basis
- Training and examination standards
There is genuine international practice variation: the historical Sarmiento data and Shao systematic review underpin a non-operative-first culture in many UK/European and Australian units, whereas the Matsunaga RCT and lower nonunion rates with fixation have driven a trend toward earlier operative management in some centres. No registry or guideline currently mandates routine surgery for the typical closed isolated fracture.
Key documentation requirements:
- Document radial nerve function before AND after any manipulation
- Record complete motor (wrist, finger, thumb extension) and sensory (dorsal first web) exam
- Document discussion of treatment options including functional bracing vs surgery
- Informed consent for surgery must include: infection, nonunion, nerve injury (especially iatrogenic), shoulder stiffness (IMN), need for hardware removal
- If radial palsy present: document as primary vs secondary and management plan
Specific risks to discuss: Radial nerve injury (iatrogenic 2-5%), infection, nonunion, hardware failure/irritation, need for bone grafting, shoulder stiffness. For IMN: add rotator cuff injury and shoulder pain (15-30%).
Key Mnemonics
WESTRadial Nerve Motor Testing
Hook:WEST - Wrist drop is the classic finding! Test wrist extension against gravity, if absent = radial nerve palsy.
STOP BRACESurgical Indications for Humeral Shaft
Hook:STOP the BRACE when surgery is needed - these are your absolute and relative surgical indications!
20-30-3-15Acceptable Angulation (Rule of 20-30-3-15)
Hook:20-30-3-15: The shoulder hides angulation well, making humeral shaft fractures forgiving for non-operative management!
HoLLyHolstein-Lewis Fracture Features
Hook:HoLLy Hurts the Radial nerve! Distal third spiral = high risk for nerve injury = consider ORIF.
MCQ Practice Points
Q: At what level does the radial nerve cross the posterior humerus in the spiral groove? A: The junction of the middle and distal thirds, approximately 14-20cm from the lateral epicondyle. Here it is tethered by the lateral intermuscular septum.
Q: What is a Holstein-Lewis fracture? A: A distal third spiral oblique fracture of the humerus with high radial nerve palsy rate (22-32%). The sharp proximal spike can trap or lacerate the radial nerve at the lateral intermuscular septum.
Q: What are the acceptable angulation limits for humeral shaft fractures treated non-operatively? A: Less than 20° sagittal (AP) angulation, less than 30° coronal (varus/valgus), less than 3cm shortening, less than 15° rotation. The shoulder compensates well for these deformities.
Q: A patient develops wrist drop after manipulation of a humeral shaft fracture. What is your management? A: This is secondary radial nerve palsy - the nerve is likely trapped in the fracture. Urgent exploration is required. Do not observe as you would for primary palsy.
Q: What is the expected spontaneous recovery rate for primary radial nerve palsy in closed humeral shaft fractures? A: 70% recover spontaneously within 3-4 months. Observe with wrist splint and EMG monitoring. Explore if no recovery by 4 months.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old man presents after falling off a ladder onto his outstretched arm. He has obvious deformity of his right upper arm and cannot extend his wrist or fingers. X-rays show a spiral fracture of the distal third of the humerus. How would you assess and manage this patient?”
“A 55-year-old woman sustains a closed transverse humeral shaft fracture at the mid-diaphysis in a motorcycle accident. She also has a closed tibial shaft fracture. Her radial nerve is intact. How would you manage this patient?”
“You are called to see a 40-year-old man in ED who had a closed humeral shaft fracture reduced in a backslab by the junior doctor. He now cannot extend his wrist or fingers - he had normal function before the reduction. What is your management?”
Key Anatomy
- Radial nerve in spiral groove at middle-distal third junction
- Nerve tethered by lateral intermuscular septum
- Triceps branches given BEFORE spiral groove (usually spared)
- Muscular deforming forces vary by fracture level
Classification
- AO/OTA: 12-A (simple), B (wedge), C (complex)
- Holstein-Lewis: distal third spiral = high radial palsy risk
- Location: proximal (30%), middle (60%), distal (10%)
- Pattern: transverse (direct blow), spiral (torsion)
Acceptable Alignment (20-30-3-15)
- under 20° sagittal (AP) angulation
- under 30° coronal (varus/valgus) angulation
- less than 3cm shortening
- under 15° rotation
Treatment Algorithm
- Most fractures: Functional bracing (over 90% union)
- STOP BRACE indications: Segmental, Transverse isthmus, Open, Polytrauma, Bilateral, Radial 2° palsy, Arterial injury, Cannot tolerate, Extended joints (floating elbow)
- Plate preferred over nail (less shoulder pain, lower reop rate)
- MIPO technique reduces iatrogenic nerve injury
Radial Nerve Palsy
- Primary palsy: observe 3-4 months, 70% recover
- Secondary palsy (post-manipulation): URGENT exploration
- Test: wrist extension, finger MCP extension, thumb extension
- Tendon transfers if no recovery: PT-ECRB, FCR-EDC, PL-EPL
Evidence Base
Sarmiento Functional Bracing Series
- 922 humeral diaphyseal fractures treated with a prefabricated functional brace; 620 (67%) available for follow-up
- Nonunion in 16 of 620 followed patients - 9 of 155 open fractures (6%) versus 7 of 465 closed fractures (less than 2%)
- Coronal angulation healed at less than 16° varus in 87% and anterior angulation less than 16° in 81%
- 98% retained shoulder motion loss of 25° or less at brace removal
Plate vs Nail Meta-Analysis (Heineman)
- Meta-analysis of 4 RCTs (203 patients) comparing intramedullary nails and plates
- No statistically significant difference in total complication rate, non-union, infection, nerve palsy, or reoperation
- Included trials were small with methodological limitations
- Authors called for a definitive large RCT
Plate vs Nail Meta-Analysis (Bhandari)
- Meta-analysis of 3 RCTs (155 patients) of compression plating versus intramedullary nailing
- Plating reduced relative risk of reoperation versus nailing (RR 0.26, 95% CI 0.007-0.9, p=0.03)
- Plating reduced shoulder problems versus nailing (RR 0.10, 95% CI 0.03-0.4, p=0.002)
- Roughly one reoperation prevented for every 10 patients treated with a plate
Radial Nerve Palsy Natural History (Shao Systematic Review)
- Systematic review of 35 studies; overall palsy prevalence 11.8% (532 palsies in 4517 fractures)
- Overall recovery 88.1%; spontaneous recovery 70.7% in conservatively managed patients
- Middle and middle-distal shaft fractures had the highest association with palsy
- No significant difference in final outcome between early exploration and expectant management
Holstein-Lewis Fracture (Original Description)
- Original description of the distal-third spiral oblique humeral fracture associated with radial-nerve paralysis
- Sharp proximal fragment displaces the radial nerve where it pierces the lateral intermuscular septum
- Established the pattern as a recognised cause of fracture-associated radial nerve injury
Bridge Plate vs Functional Brace RCT (Matsunaga)
- RCT of 110 patients - minimally invasive bridge-plate osteosynthesis versus functional brace
- DASH score modestly better with surgery at 6 months only (10.9 vs 16.9, p=0.046)
- Lower nonunion rate with surgery (0% vs 15%)
- No difference in SF-36, pain, or Constant-Murley score; coronal angulation lower with plating (2.0° vs 10.5°)
Population Epidemiology - Swedish Fracture Register
- 2,011 adult humeral fractures from the Swedish Fracture Register (2011-2013); 13% were shaft fractures
- Humeral shaft fracture incidence 13.4 per 100,000 person-years
- Female:male ratio 2.4:1; mean age 66.8 years, with most fractures from low-energy falls in patients over 50
- Only 1.2% open and 1.3% pathological