Systematic radiographic evaluation of joint replacements - component position, fixation, wear and the recognition of loosening, instability, periprosthetic fracture and adverse tissue reaction
- Progressive lucency greater than 2mm suggests loosening
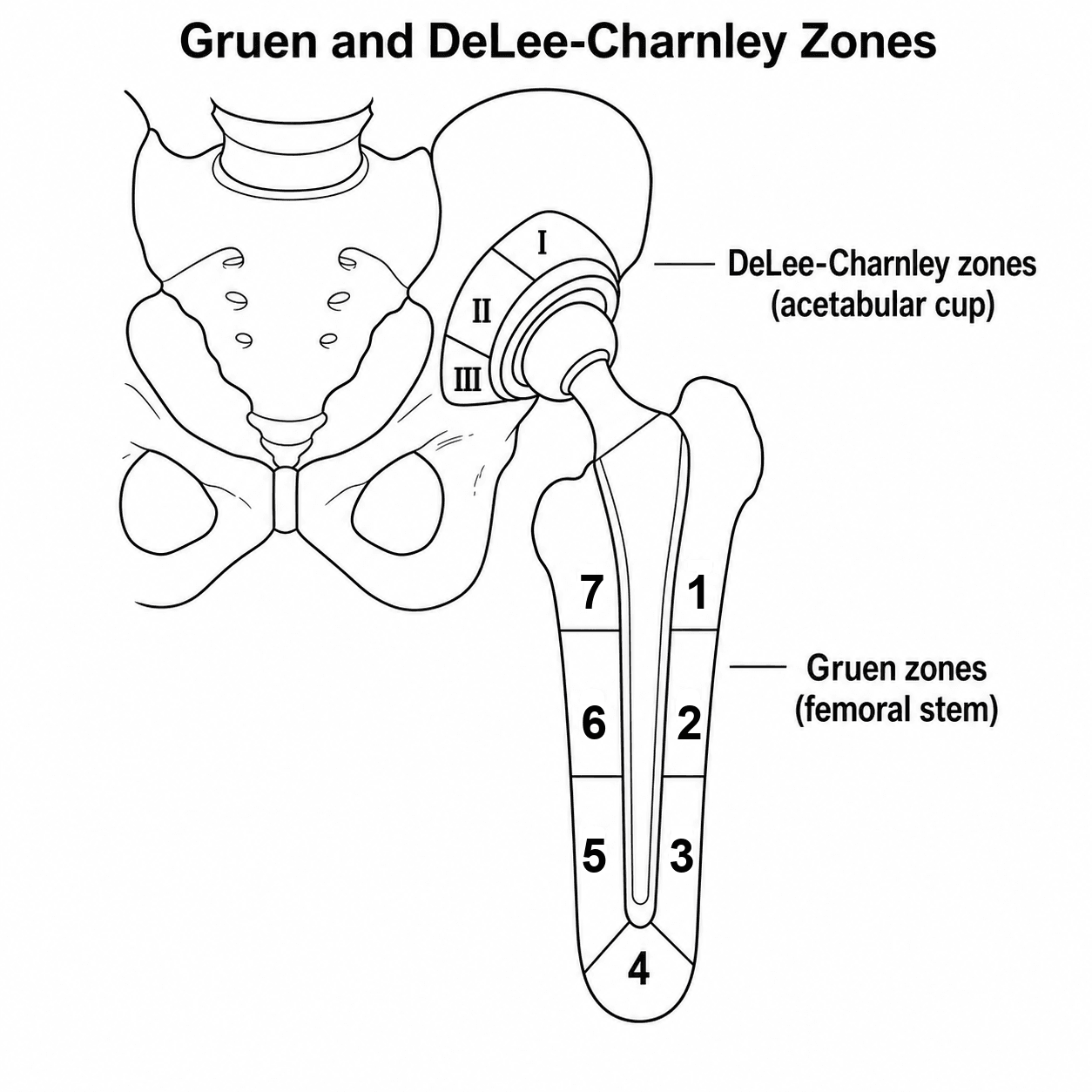
- DeLee-Charnley zones (acetabulum), Gruen zones (femur)
- Component migration is most specific sign of loosening
- Heterotopic ossification: Brooker classification (I-IV)
- Polyethylene wear: eccentric head position, osteolysis
- “Serial X-rays essential - single film cannot confirm loosening
- “All 3 acetabular zones or all femoral zones = definite loosening
- “PE wear precedes osteolysis by years
- “Varus/valgus stem: risk for periprosthetic fracture
- “CT with MARS for metal artefact reduction
Arthroplasty imaging is commonly examined. You must know the zone systems (Gruen, DeLee-Charnley), how to measure component position (cup inclination/anteversion, stem alignment), and differentiate loosening from normal radiolucent lines.
Overview & Imaging Principles
Arthroplasty is among the highest-volume elective procedures in orthopaedics, and surveillance imaging is a core skill tested in every fellowship exam. The plain radiograph remains the first-line and most informative single investigation: it assesses component position, fixation, polyethylene wear, periprosthetic bone and fracture, and - through serial comparison - is the principal tool for diagnosing loosening. Cross-sectional imaging (CT with metal-artefact reduction, MRI with MARS, ultrasound and nuclear medicine) is reserved for specific questions that plain films cannot answer.


Systematic Approach: Zone Classification Systems
- Location
- Lateral proximal (greater trochanter)
- Clinical Significance
- High stress area, loosening indicator
- Location
- Lateral middle
- Clinical Significance
- Cemented mantle assessment
- Location
- Lateral distal
- Clinical Significance
- Cement-bone interface
- Location
- Stem tip
- Clinical Significance
- End-bearing stress, pedestal formation
- Location
- Medial distal
- Clinical Significance
- Cement-bone interface
- Location
- Medial middle
- Clinical Significance
- Calcar region assessment
- Location
- Medial proximal (calcar)
- Clinical Significance
- High stress, loosening indicator
A-B-C-D-E-FSystematic Read of Any Arthroplasty Film
Hook:A single radiograph rarely confirms loosening - migration or progressive lucency on serial films is what counts. State this explicitly in the viva.
Loosening Assessment
- Description
- Radiolucent line increasing over time
- Significance
- Greater than 2mm or progressive = loosening
- Description
- Change in position over serial films
- Significance
- Most specific sign of loosening
- Description
- Break in cement mantle
- Significance
- Cemented component failure
- Description
- Focal lucent areas around component
- Significance
- Wear debris-induced resorption
- Description
- Lucent line with distal sclerosis
- Significance
- Distal load transfer, proximal loosening
- Description
- Distal migration of stem
- Significance
- Measure from tip to fixed landmark
Progressive = ProblemDifferentiating Loosening from Normal Lines
Hook:A single X-ray cannot confirm loosening - always compare with prior films and assess for progression
The 4 P'sWhen a Radiolucent Line Means Loosening
Hook:A thin (under 2 mm), non-progressive, single-zone line is usually a stable fibrous membrane, not loosening. Width AND progression together raise concern.
Cement Mantle Grading (Barrack)
The systematic read includes grading the femoral cement mantle (the "C" of the A-B-C-D-E-F mnemonic), not just describing zonal lucency. The Barrack classification grades the quality of a cemented femoral mantle on the immediate post-operative radiograph and is a recognised predictor of subsequent loosening: a thin, uniform, complete mantle reflects good cementing technique, whereas a deficient or incomplete mantle predisposes to debonding and early failure.
- Radiographic Appearance
- Complete 'white-out' at the cement-bone interface; canal fully filled by cement with no discernible lucency
- Significance
- Best fixation; lowest loosening risk
- Radiographic Appearance
- Near-complete mantle with a thin radiolucency at part of the cement-bone interface
- Significance
- Acceptable mantle
- Radiographic Appearance
- Radiolucency at 50-99% of the cement-bone interface
- Significance
- Poorer mantle; higher loosening risk
- Radiographic Appearance
- Deficient mantle - stem abuts cortex with the mantle thinner than about 1mm or absent in places
- Significance
- Mantle defect predisposing to debonding
- Radiographic Appearance
- Gross deficiency - failure to fill the canal, a mantle defect, or no cement distal to the stem tip; air at the interface
- Significance
- Worst grade; strongly associated with early loosening
Grade the mantle, do not just describe the line. After reporting zonal lucency, state the Barrack grade of a cemented femoral component. Barrack's original work linked inadequate (Grade C-D) mantles to markedly higher early femoral loosening than Grade A-B. This is a femoral-component grade reflecting cementing technique - a uniform mantle of adequate thickness with cement-bone "white-out" is the radiographic signature of good technique.
Polyethylene Wear
- Description
- Femoral head not centred in cup
- Clinical Implication
- Direct wear measurement possible
- Description
- Head moves toward dome of cup
- Clinical Implication
- Most common wear direction
- Description
- Measure head-cup distance on serial films
- Clinical Implication
- Greater than 0.2mm/year = excessive
- Description
- Lucent areas around components
- Clinical Implication
- Wear debris-induced bone resorption
- Description
- Balloon lesions expanding from joint
- Clinical Implication
- Requires revision to halt progression
Heterotopic Ossification
- Description
- Islands of bone within soft tissue
- Clinical Significance
- Usually asymptomatic
- Description
- Bone spurs from pelvis or proximal femur, greater than 1cm gap
- Clinical Significance
- Mild limitation
- Description
- Bone spurs with less than 1cm gap
- Clinical Significance
- Moderate limitation
- Description
- Apparent bony ankylosis
- Clinical Significance
- Severe limitation, may need excision
Instability and Dislocation
- Risk Contribution
- Abduction greater than 55° or less than 30°
- Radiographic Assessment
- Measure cup inclination on AP
- Risk Contribution
- Combined less than 25° or greater than 50°
- Radiographic Assessment
- CT for accurate measurement
- Risk Contribution
- Reduced offset decreases stability
- Radiographic Assessment
- Compare to contralateral
- Risk Contribution
- Smaller heads higher dislocation risk
- Radiographic Assessment
- Less than 32mm higher risk
- Risk Contribution
- Bone or soft tissue blocking motion
- Radiographic Assessment
- Look for osteophytes, HO
Periprosthetic Fracture
- Location
- Trochanteric region
- Subtype
- AG: Greater troch, AL: Lesser troch
- Treatment Principle
- Often non-operative if stable
- Location
- Around/below stem
- Subtype
- Stem WELL FIXED
- Treatment Principle
- ORIF, keep stem
- Location
- Around/below stem
- Subtype
- Stem LOOSE
- Treatment Principle
- Revision stem + ORIF
- Location
- Around/below stem
- Subtype
- Stem LOOSE + poor bone
- Treatment Principle
- Revision with structural allograft
- Location
- Below stem tip
- Subtype
- Stem unaffected
- Treatment Principle
- Treat as standard fracture
Metal Artefact Reduction
- Technique
- Standard technique
- Indication
- First-line, least artefact
- Technique
- Metal artefact reduction sequences
- Indication
- Bone detail, osteolysis assessment
- Technique
- Metal artefact reduction, STIR
- Indication
- Soft tissue, ALTR assessment
- Technique
- No metal artefact
- Indication
- Fluid collections, tendons
- Technique
- WBC/marrow scan
- Indication
- PJI assessment
Differential Diagnosis of the Painful Arthroplasty
A painful joint replacement is a common exam and clinic scenario. Imaging must be interpreted alongside the clinical picture and inflammatory markers, because the single most important diagnosis to exclude - prosthetic joint infection - can produce radiographs that look identical to aseptic loosening.
- Typical Pain Pattern
- Start-up / activity-related, deep
- Key Imaging Features
- Progressive lucency in all zones, migration, subsidence, no aggressive periostitis
- Confirmatory Test
- Serial radiographs; intra-operative findings
- Typical Pain Pattern
- Constant rest pain, early onset, stiffness
- Key Imaging Features
- Lucency that can be indistinguishable from aseptic loosening; periostitis or rapid osteolysis raise suspicion
- Confirmatory Test
- Aspiration (cell count, culture), CRP/ESR, alpha-defensin
- Typical Pain Pattern
- Often painless until late
- Key Imaging Features
- Eccentric head position, expansile balloon lucencies (particle disease)
- Confirmatory Test
- Serial wear measurement, CT for osteolysis volume
- Typical Pain Pattern
- Mechanical, positional, giving way
- Key Imaging Features
- Cup mal-orientation, eccentric head, impingement; combined version outside target
- Confirmatory Test
- CT for version; dynamic/stress views
- Typical Pain Pattern
- Acute, post-fall, unable to weight-bear
- Key Imaging Features
- Cortical break (Vancouver/Su); assess stem fixation
- Confirmatory Test
- Orthogonal radiographs; CT if occult
- Typical Pain Pattern
- Groin/thigh ache, swelling, clicking
- Key Imaging Features
- Effusion, pseudotumour, muscle/tendon damage on MARS-MRI
- Confirmatory Test
- MARS-MRI, serum cobalt/chromium ions
- Typical Pain Pattern
- Usually asymptomatic
- Key Imaging Features
- Proximal femoral bone loss with cementless stems, no migration
- Confirmatory Test
- Serial radiographs (not true loosening)
- Typical Pain Pattern
- Variable, non-mechanical
- Key Imaging Features
- Normal implant; look at spine, vessels, abdomen
- Confirmatory Test
- Targeted imaging of source
Never report progressive lucency around an implant as "aseptic loosening" without considering low-grade infection. Radiographs cannot reliably separate the two; the work-up of a painful arthroplasty must include inflammatory markers and a low threshold for joint aspiration.
Guidelines, Registries & Global Practice
Arthroplasty surveillance is informed by national joint registries and society guidance worldwide. Imaging recommendations converge on serial plain radiographs as the backbone, with risk-stratified cross-sectional imaging for specific failure modes.
- Focus
- THA/TKA surveillance & PJI
- Imaging-Relevant Guidance
- Plain radiographs first-line; standardised work-up for the painful arthroplasty including ESR/CRP and aspiration before attributing pain to aseptic loosening
- Focus
- Joint replacement follow-up
- Imaging-Relevant Guidance
- Risk-stratified radiographic follow-up (e.g. at defined intervals for higher-risk implants); registry-linked surveillance
- Focus
- Metal-on-metal & modular tapers
- Imaging-Relevant Guidance
- Risk-based surveillance using symptoms, serum cobalt/chromium ions and cross-sectional imaging (MARS-MRI or ultrasound) for adverse local tissue reaction
- Focus
- Outcome reporting & follow-up
- Imaging-Relevant Guidance
- Harmonised radiographic outcome measures; emphasis on registry data for implant performance
- Focus
- Implant identification
- Imaging-Relevant Guidance
- Underpins component traceability that aids radiographic implant recognition
- Contribution
- Large primary & revision volumes
- Imaging Relevance
- Implant- and bearing-specific revision rates flag designs warranting closer radiographic surveillance
- Contribution
- Detailed revision-by-diagnosis data
- Imaging Relevance
- Early identification of poorly performing implants (e.g. certain MoM hips) prompting targeted imaging
- Contribution
- Growing national dataset
- Imaging Relevance
- Benchmarking revision causes including loosening, instability and PJI
- Contribution
- Long-term implant survival
- Imaging Relevance
- Decades-long survivorship informing follow-up intervals and revision-risk imaging
Special Circumstances
Scapular Notching Grading (Reverse Shoulder)
The Special Circumstances note flags scapular notching as the key thing to watch on a reverse shoulder arthroplasty film, but notching is graded, not just described. The Sirveaux-Nerot classification grades the inferior scapular erosion that results from mechanical impingement of the humeral cup on the inferior scapular neck in adduction (a feature of the medialised Grammont design). It is assessed on a true AP (Grashey) view.
- Extent of Inferior Scapular Erosion
- Defect confined to the scapular pillar (inferior neck)
- Implication
- Minor; often asymptomatic
- Extent of Inferior Scapular Erosion
- Erosion reaching (in contact with) the inferior baseplate screw
- Implication
- Progressive impingement wear
- Extent of Inferior Scapular Erosion
- Erosion extending beyond/over the inferior screw
- Implication
- Concern for baseplate fixation over time
- Extent of Inferior Scapular Erosion
- Erosion extending under the baseplate towards the central peg/fixation
- Implication
- Threatens glenoid component fixation
Notching is impingement wear, and the grade matters. Scapular notching reflects repetitive contact of the polyethylene humeral cup on the inferior scapular neck; higher grades (3-4) are associated with poorer functional outcomes and possible glenoid component loosening. Radiographic strategies that reduce it - inferior glenosphere positioning, inferior tilt, and a larger or lateralised glenosphere - are the things to mention alongside grading it on the AP view.
Areas of Uncertainty & Controversy
MCQ & Exam Practice Points
Q: A radiolucent line is seen in only DeLee-Charnley zone III on a single post-operative pelvis film. Does this confirm acetabular loosening? A: No. A thin, non-progressive line in one zone is usually a stable fibrous membrane. Loosening requires lucency in all three zones, progression on serial films, or definite cup migration - a single film cannot confirm it.
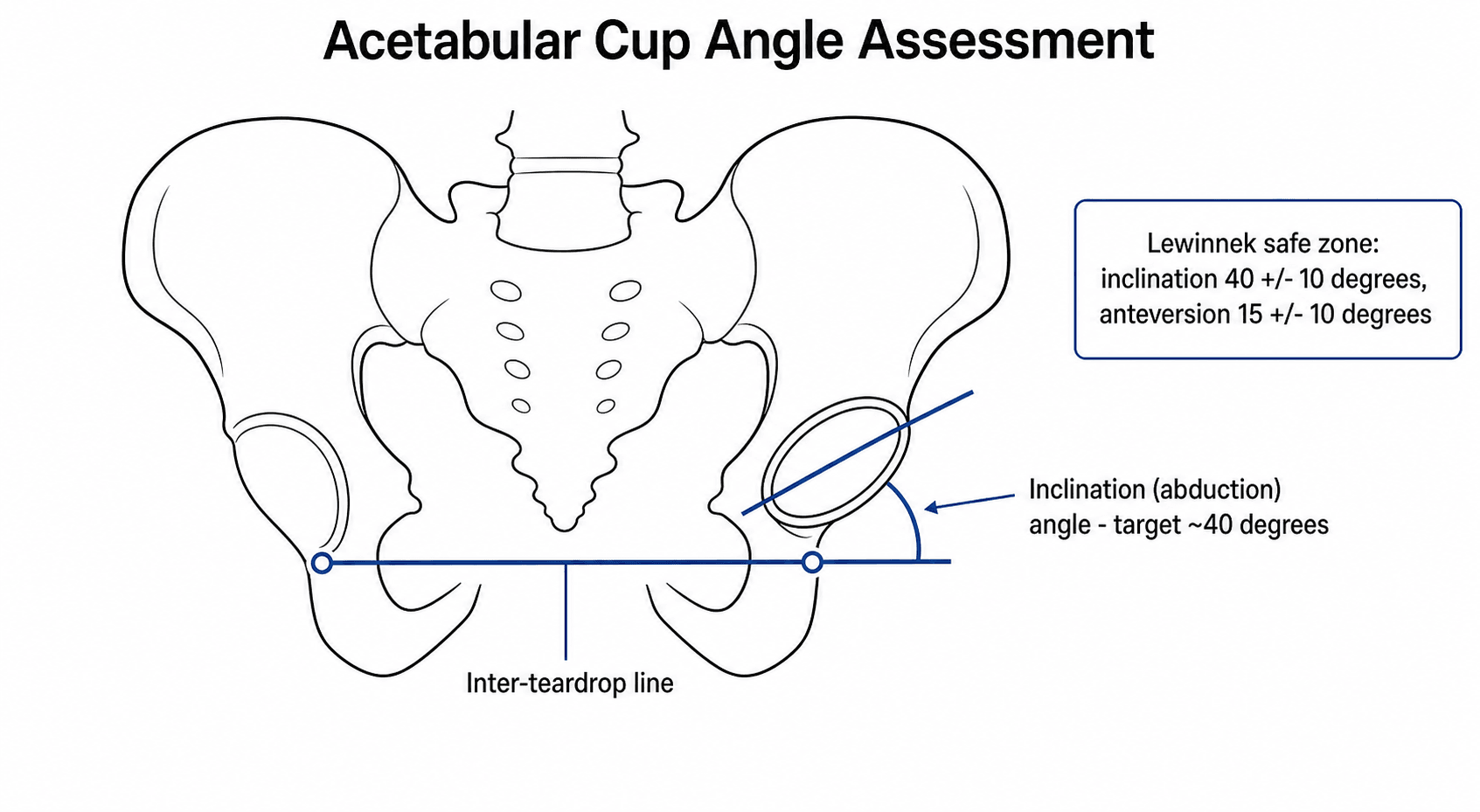
Q: A dislocated THA has a cup measured at 42 degrees inclination and 14 degrees anteversion. The cup is 'within the Lewinnek safe zone' - so cup position cannot be the problem, correct? A: Incorrect. Abdel et al. (CORR 2016) showed 58% of dislocating THAs had cups inside the Lewinnek zone. Stability is multifactorial - consider spinopelvic mobility, head size, soft-tissue tension, offset and approach.
Q: Which single radiographic sign is the most specific for component loosening? A: Component migration (a change in position on serial films). Progressive lucency over 2 mm is supportive, but migration is the most specific single sign - which is why prior films are essential.
Clinical Imaging: Standard Radiographic Assessment
- Measurement
- Angle between cup face and inter-teardrop line
- Normal/Optimal Range
- 40° ± 10° (30-50°)
- Measurement
- Lateral view or CT
- Normal/Optimal Range
- 15° ± 10° (5-25°)
- Measurement
- Superolateral cup covered by bone
- Normal/Optimal Range
- Greater than 80%
- Measurement
- Compare lesser trochanter to teardrop line
- Normal/Optimal Range
- Within 10mm of contralateral
- Measurement
- Centre of head to femoral shaft axis
- Normal/Optimal Range
- Restore native offset ± 5mm
- Measurement
- Varus/valgus relative to shaft
- Normal/Optimal Range
- Neutral to 3° valgus
- Measurement
- Distance from stem tip to fixed landmark
- Normal/Optimal Range
- Less than 2-3mm stable
Radiographic Examples
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 72-year-old presents with thigh pain 8 years after cemented total hip arthroplasty. You are shown an AP pelvis X-ray.”
“A 60-year-old falls at home 3 years after cementless THA. X-ray shows a periprosthetic femoral fracture at the level of the stem.”
“A patient 2 years post TKR presents with anterior knee pain and difficulty with stairs. X-rays including skyline view are shown.”
Optimal Component Position
- Cup inclination: 40° ± 10°
- Cup anteversion: 15° ± 10°
- Combined anteversion: 25-50°
- Stem: Neutral to 3° valgus
- Leg length: Within 10mm
Zone Systems
- Gruen (femur): 7 zones (1-3 lateral, 4 tip, 5-7 medial)
- DeLee-Charnley (acetabulum): 3 zones (I superior, II medial, III inferior)
- All zones lucent = definite loosening
- Zones 1 and 7 = high stress loosening pattern
Loosening Signs
- Progressive lucency greater than 2mm
- Component migration (most specific)
- Cement fracture
- Subsidence greater than 3mm
- Serial films essential
Vancouver Classification (PPF)
- A: Trochanteric (AG/AL) - often non-op
- B1: Stem fixed - ORIF, keep stem
- B2: Stem loose, good bone - revision stem
- B3: Stem loose, poor bone - revision + graft
- C: Below stem - treat as standard fracture
Evidence Base & Landmark Classifications
The radiographic frameworks used at the viva table - Gruen and DeLee-Charnley zones, the Lewinnek safe zone, the Brooker grade and the Vancouver classification - each originate from a specific paper. Knowing the source, the cohort and the modern caveats demonstrates depth.
Gruen Zones - 'Modes of Failure' of Cemented Femoral Stems
- Defined the 7-zone femoral analysis still used today
- Loosening is a zonal, mode-specific process - not random
- Proximal (calcar) and distal (tip) patterns reflect different failure mechanics
- Serial radiographs distinguished progressive from static lucency
DeLee-Charnley Zones - Acetabular Radiolucency
- Established the 3-zone (I superior, II medial, III inferior) acetabular system
- Demarcation is common and usually benign; migration is the worrying sign
- Progressive migration - not the mere presence of a line - predicts failure
- Technical/surgical factors and low-grade sepsis explained most migrating cases
Lewinnek Safe Zone - Cup Orientation and Dislocation
- Origin of the classic 40 deg plus or minus 10 inclination and 15 deg plus or minus 10 anteversion targets
- Roughly four-fold higher dislocation outside the zone
- Greatest dislocation risk in the first 30 days and after prior surgery
- Defined cup orientation as a measurable, modifiable radiographic target
Contemporary Caveat - The Lewinnek 'Safe Zone' Is Not Truly Safe
- The majority of dislocating THAs were inside the 'safe zone'
- Cup position is necessary but not sufficient for stability
- Spinopelvic mobility, soft tissues, head size and approach all contribute
- Targets are a guide, not a guarantee
Brooker Classification - Heterotopic Ossification after THA
- Standard radiographic grading of HO around the hip
- Higher grades correlate with reduced range of motion
- Grade IV (ankylosis) may warrant excision after maturation
- Provides a reproducible language for follow-up films
Imaging Accuracy for Aseptic Femoral Loosening (Meta-analysis)
- Plain radiography performs as well as more invasive tests
- No single modality is clearly superior for femoral loosening
- Plain films plus bone scintigraphy are the preferred first-line work-up
- Specificity is imperfect - correlate with symptoms and serial films
Vancouver Classification - Periprosthetic Femoral Fractures
- Treatment hinges on whether the stem is well-fixed or loose
- B1 - retain stem with ORIF; B2 - revise the stem; B3 - revise plus reconstruct bone
- Radiographic assessment of pre-existing lucency is essential to subtype
- Fractures around loose/malaligned stems do poorly with fixation alone