Classic Signs, Named Fractures & Pattern Recognition
Shoulder: Lightbulb sign, Hill-Sachs, Bankart, sail sign (fat pad)
Elbow: Posterior fat pad, sail sign, radiocapitellar line disruption
Wrist: Terry Thomas (SL dissociation), signet ring (scaphoid rotation), DISI/VISI
Hip/Pelvis: Shenton line, lightbulb sign (femur), Klein line
Knee: Segond, lipohaemarthrosis, deep lateral notch
Foot/Ankle: Boehler angle, Lisfranc fleck, fibular length
Key: Each sign has an anatomical basis — understanding the mechanism helps you recognise and interpret it
- Pattern recognition of classic radiological signs accelerates diagnosis and prevents missed injuries.
- Many eponymous signs are pathognomonic for specific injuries and appear in virtually every fellowship exam.
- The posterior fat pad sign, Segond fracture, and lipohaemarthrosis are the three most commonly tested trauma signs.
- Every named sign has an underlying anatomical or pathological basis — understanding WHY the sign occurs is as important as recognising it.
- Associated injuries MUST be sought when a classic sign is identified — isolated findings are rare in high-energy trauma.
- “Segond fracture: lateral tibial plateau avulsion from the anterolateral ligament/capsular attachment during pivot shift = ACL tear (100% association).
- “Boehler angle: measured on lateral calcaneal radiograph. Normal 25-40 degrees. Less than 20 degrees = calcaneal fracture with subtalar joint involvement.
- “Terry Thomas sign: widened scapholunate gap more than 3mm on PA wrist radiograph = scapholunate ligament dissociation.
- “Fleck sign: small avulsion fragment between 1st and 2nd metatarsal bases = Lisfranc ligament rupture (easily missed).
- “Double density sign (shoulder): humeral head overlapping glenoid on AP = posterior dislocation.
Radiological signs in trauma are among the most tested topics in fellowship examinations. You will be shown radiographs and asked to identify specific signs, explain their anatomical basis, describe associated injuries, and outline management. The most commonly tested signs are: posterior fat pad sign, Segond fracture, Boehler angle, Terry Thomas sign, Lisfranc fleck sign, and lipohaemarthrosis. You MUST know both the sign AND its clinical significance.
SHALLUpper Limb Trauma Signs
Hook:SHALL: the upper limb trauma signs that you SHALL know for the exam.
SABLELower Limb Trauma Signs
Hook:SABLE: five lower limb signs — Segond, Angle (Boehler), Blood (lipohaemarthrosis), Lisfranc, External rotation.
DISI/VISIWrist Instability Signs
Hook:DISI = lunate points Dorsally (extends). VISI = lunate points Ventrally (flexes). Terry Thomas shows the gap.
Overview
Radiological signs in trauma serve as pattern recognition tools that accelerate diagnosis and prevent missed injuries. Each eponymous sign has a specific anatomical and pathological basis that explains why the sign appears. Understanding the mechanism behind the sign is essential for both recognising it and predicting associated injuries.
Musculoskeletal trauma radiographs are often assessed under time pressure (emergency department, trauma assessment). Named radiological signs provide a mental framework for: (1) rapid identification of specific injury patterns, (2) prediction of associated injuries that may not be immediately visible, (3) guiding further imaging (CT, MRI) when a sign is identified, (4) structured viva examination responses. Each sign has THREE components: (a) what it looks like, (b) why it occurs (anatomical mechanism), and (c) what injuries it is associated with.
When a classic trauma sign is identified, ALWAYS look for associated injuries. Key associations: Segond fracture = ACL tear (100%) + meniscal tear (75%). Lipohaemarthrosis = intra-articular fracture (tibial plateau, distal femur, patella). Lisfranc fleck = tarsal-metatarsal instability (weight-bearing stress views needed). Hill-Sachs + Bankart = anterior shoulder dislocation. Monteggia = ulnar fracture + radial head dislocation. Maisonneuve = proximal fibula fracture + syndesmotic disruption + medial ankle injury.
Systematic Approach
Radiological Signs — Comprehensive Reference
- Anatomical Basis
- Posterior fat pad pushed out of olecranon fossa by haemarthrosis
- Clinical Significance
- Occult fracture until proven otherwise. Radial head (adults), supracondylar (children)
- Anatomical Basis
- Anterolateral capsule/ligament avulsion from lateral tibial plateau during pivot shift
- Clinical Significance
- PATHOGNOMONIC for ACL tear (100% association). Also associated with meniscal tears (75%)
- Anatomical Basis
- Bone marrow fat leaks through intra-articular fracture into joint — fat floats on blood
- Clinical Significance
- Intra-articular fracture. Most common: tibial plateau. Requires CT for characterisation
- Anatomical Basis
- Calcaneal body compression fracture flattens angle between posterior tuberosity and posterior facet
- Clinical Significance
- Calcaneal fracture with subtalar involvement. Normal 25-40 degrees, abnormal less than 20 degrees
- Anatomical Basis
- Lisfranc ligament avulsion from base of 2nd MT or medial cuneiform
- Clinical Significance
- Tarsometatarsal joint disruption. EASILY missed. Requires weight-bearing or stress views
- Anatomical Basis
- Humeral head internally rotated (posterior dislocation) appears symmetric/rounded on AP
- Clinical Significance
- POSTERIOR shoulder dislocation. Axillary lateral is ESSENTIAL to confirm
- Anatomical Basis
- Scapholunate gap more than 3mm on PA view from SL ligament rupture
- Clinical Significance
- Scapholunate dissociation (DISI pattern). Progressive arthritis if untreated (SLAC wrist)
- Anatomical Basis
- Normal smooth arc along inferior pubic ramus and medial femoral neck is broken
- Clinical Significance
- NOF fracture or hip dislocation. Trace bilaterally on AP pelvis
Differential Diagnosis — Mimics & Look-alikes
Several normal variants and non-traumatic findings imitate classic trauma signs. The exam favourite is being asked "what else could this be?" — knowing the mimics prevents both over-call and missed injury.
- True traumatic cause
- Occult intra-articular fracture (radial head, supracondylar)
- Mimic to exclude
- Septic or inflammatory effusion; technically non-true-lateral film
- Discriminator
- Trauma history + true lateral with overlapping condyles; aspirate if sepsis suspected
- True traumatic cause
- Anterolateral ligament/capsular avulsion = ACL injury
- Mimic to exclude
- Reverse Segond (medial avulsion, PCL/medial injury); arcuate avulsion (fibular head, posterolateral corner)
- Discriminator
- Location: Segond is lateral tibia; reverse Segond is medial tibia; arcuate is fibular styloid
- True traumatic cause
- Intra-articular fracture leaking marrow fat
- Mimic to exclude
- None benign — always implies fracture, but level only seen on horizontal-beam film
- Discriminator
- Requires cross-table/horizontal beam; absence on AP does not exclude fracture
- True traumatic cause
- Posterior dislocation (locked internal rotation)
- Mimic to exclude
- Normal internally rotated arm; poor positioning
- Discriminator
- Trough line, rim sign, over 6 mm joint widening; confirm with axillary/scapular-Y
- True traumatic cause
- Lisfranc ligament avulsion (fleck sign)
- Mimic to exclude
- Normal physis in children; os intermetatarseum accessory ossicle
- Discriminator
- Smooth corticated ossicle vs jagged avulsion; compare contralateral and weight-bear
- True traumatic cause
- SL ligament rupture (Terry Thomas)
- Mimic to exclude
- Normal in young children; clenched-fist artefact; ulnar-deviation positioning
- Discriminator
- Need over 3 mm on neutral PA, ideally with contralateral comparison; correlate with DISI on lateral
Guidelines, Registries & Global Practice
Recognition of classic radiological trauma signs is a core competency in every major orthopaedic and emergency-medicine curriculum worldwide (FRCS Tr&Orth, FRACS, EBOT/FEBOT, ABOS, DNB/MS, MRCS, SICOT). Missed injuries on trauma radiographs are a leading source of medicolegal claims internationally, which is why structured "search pattern" reading and named-sign checklists are emphasised across systems.
Global Epidemiology
- Missed diagnoses are common and systematic. Posterior shoulder dislocation is misdiagnosed in over 60% of cases at first presentation; Lisfranc injuries and the Segond fracture are repeatedly cited among the most frequently overlooked findings on initial radiographs.
- Mechanism-driven incidence: Segond/ACL injuries cluster in young pivoting athletes; calcaneal and thoracolumbar burst fractures cluster in fall-from-height and road-trauma populations; posterior shoulder dislocation is over-represented in seizure, electrocution and high-energy direct trauma.
Side-by-Side Guidance
- Position relevant to named signs
- Advocate CT for articular fractures (tibial plateau, calcaneus, pilon) once a sign or effusion is seen; Sanders CT classification guides calcaneal management
- Position relevant to named signs
- BOAST standards mandate adequate orthogonal views and senior review; open-fracture and spinal-clearance standards stress not relying on a single inadequate film
- Position relevant to named signs
- Promotes systematic ABCs search pattern (Adequacy, Bone, Cartilage/joints, Soft tissue) and CT for intra-articular extension and pre-operative planning
- Position relevant to named signs
- Trauma imaging guidance favours CT in significant blunt/polytrauma and supports MRI for occult injury where radiographs are equivocal
- Position relevant to named signs
- Appropriateness criteria endorse weight-bearing/stress views for suspected Lisfranc and syndesmotic injury and MRI for radiographically occult fracture
Registry & Practice Variation
- Registry relevance: Implant registries (NJR, AJRR, AOANJRR, Swedish/Norwegian/NZJR) do not catalogue radiological signs directly, but the downstream conditions they track — post-traumatic OA, SLAC-wrist salvage, post-calcaneal arthrodesis, post-traumatic knee arthroplasty — quantify the long-term cost of injuries first announced by these signs (e.g. an unrecognised Segond/ACL injury or a malreduced calcaneus).
- High-resource settings: Ready access to CT and MRI means a positive sign (effusion, fleck, lipohaemarthrosis) is promptly characterised with cross-sectional imaging; weight-bearing and stress views for Lisfranc/syndesmosis are routine.
- Limited-resource settings: Plain radiography may be the only modality available, which raises rather than lowers the value of named-sign recognition; contralateral comparison views, stress views and clinical correlation become the principal tools, and a positive sign is treated as the injury until proven otherwise.
Controversies & Areas of Uncertainty
The Segond fracture itself is rarely fixed — it is treated as a marker injury and management is directed at the ACL and associated meniscal/anterolateral structures. The contested question is whether anterolateral structures (ALL reconstruction or lateral extra-articular tenodesis) should be added to ACL reconstruction in high pivot-shift knees, revisions and young pivoting athletes. Evidence (including the ALL anatomical and clinical literature) increasingly supports lateral augmentation in selected patients, but routine use remains debated.
The landmark Buckley RCT showed equivalent unstratified outcomes but a real surgical benefit in defined subgroups. Modern debate has shifted toward minimally invasive/percutaneous and sinus-tarsi approaches to reduce the high wound-complication rate of the extensile lateral approach, and toward primary subtalar arthrodesis for Sanders IV. There is still no universal consensus on which displaced fracture mandates surgery.
A positive fat pad sign, lipohaemarthrosis or subtle Lisfranc fleck reliably implies fracture, but how aggressively to pursue CT or MRI varies. MRI detects far more bone and soft-tissue injury than radiographs (as in the elbow fat pad data), yet in several series the extra findings did not change management — so routine advanced imaging for every positive sign is not universally accepted.
Several "objective" signs depend on technique and reader. Bohler angle, scapholunate gap and medial clear space all vary with projection, rotation and weight-bearing, and inter-observer agreement is imperfect. Contralateral comparison views and correlation with clinical examination remain essential rather than relying on a single threshold number.
Detailed Sign Analysis
Upper Limb Trauma Signs
Lightbulb sign (posterior shoulder dislocation): The humeral head appears abnormally rounded and symmetric on the AP radiograph because the humerus is locked in internal rotation. The normal external rotation profile (with the greater tuberosity visible laterally) is lost, creating a dome-shaped appearance. This is the only radiographic view in which a posterior dislocation can be suspected — the AP view looks deceptively near-normal. The KEY action when this sign is present is to obtain an axillary lateral view, which will clearly show the posterior position of the humeral head relative to the glenoid. Posterior dislocations are the most commonly missed dislocation in emergency medicine.
Terry Thomas sign (scapholunate dissociation): Named after the British comedian with a gap between his front teeth. A widened space between the scaphoid and lunate more than 3mm on a PA wrist radiograph (measured at the mid-point of the gap) indicates rupture of the scapholunate interosseous ligament (SLIL). This leads to a DISI pattern (lunate extends on lateral view, SL angle more than 70 degrees) and, if untreated, progresses to SLAC (scapholunate advanced collapse) wrist — a predictable pattern of radiocarpal arthritis.
Signet ring sign: On the PA wrist radiograph, the scaphoid appears as a rounded circle (like a signet ring viewed from above) because it has rotated into flexion and is now viewed end-on. This is associated with scapholunate dissociation — the scaphoid flexes when the SL ligament is disrupted, losing its normal elongated oval appearance.
Radiocapitellar line disruption: A line drawn through the centre of the radial shaft must bisect the capitellum on ALL views. If this line fails to pass through the capitellum on ANY view, the radial head is dislocated — this is the key to diagnosing Monteggia fracture-dislocation (ulnar fracture + radial head dislocation).
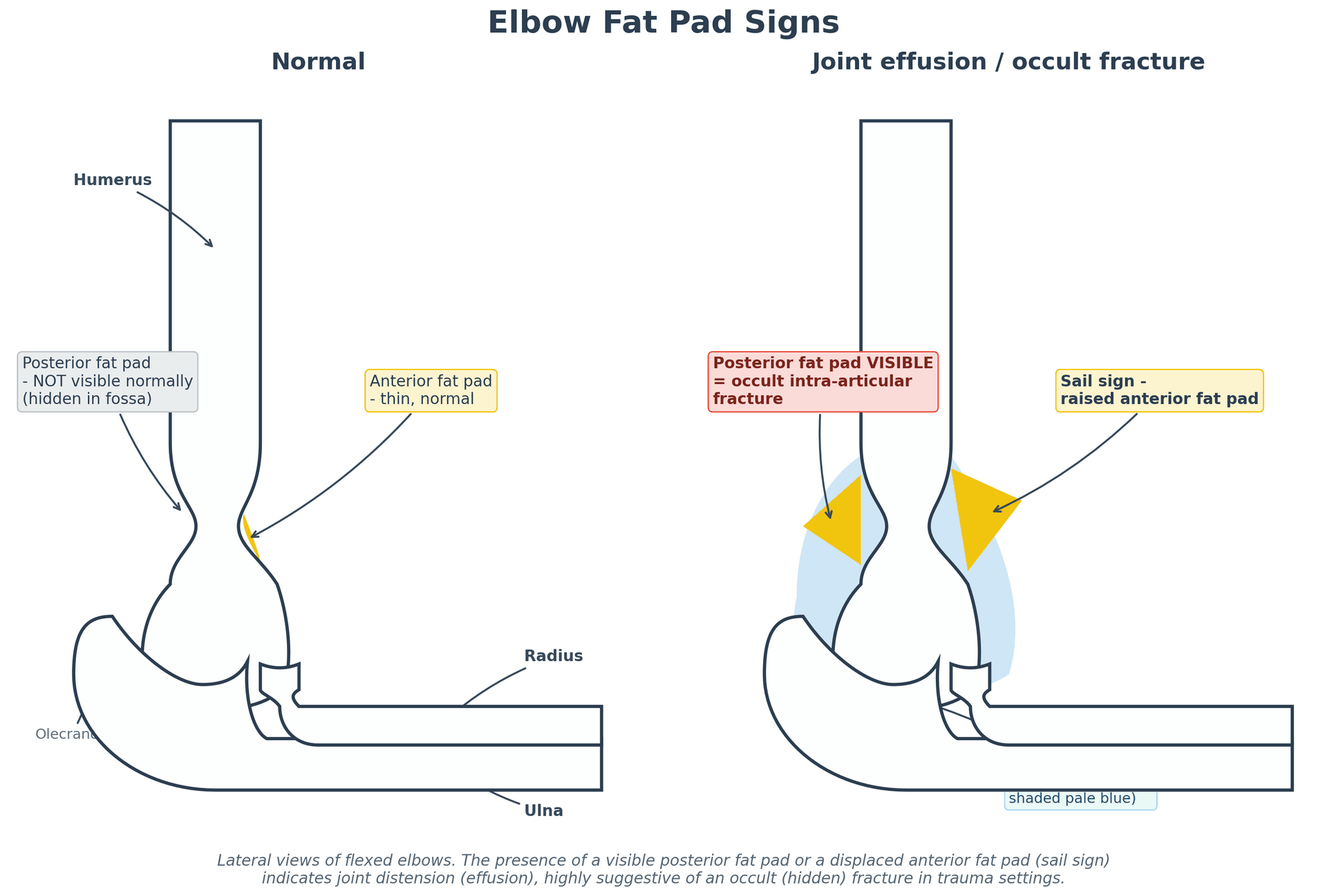
Anterior (sail) vs posterior fat pad — a crucial distinction: On a true lateral elbow (flexed 90 degrees), the two fat pads behave differently and must not be lumped together. The anterior fat pad sits in the coronoid fossa and is normally visible as a thin lucency hugging the cortex; when a joint effusion lifts it, it becomes a raised triangular shape — the "sail sign". The posterior fat pad lies deep in the olecranon fossa and is NEVER visible normally — so any visible posterior fat pad indicates an effusion/haemarthrosis and an occult intra-articular fracture until proven otherwise (radial head in adults, supracondylar in children). In short: an elevated anterior fat pad (sail) is suggestive, but a visible posterior fat pad is the more reliable red flag. (A false-negative occurs if the film is not a true lateral or the elbow is not flexed to 90 degrees.)
Avulsion Fractures as Markers of Injury
A small flake of bone pulled off at a tendon or ligament attachment is a "signpost" injury - the fleck tells you which soft-tissue structure has failed. Beyond the knee avulsions (Segond/reverse Segond/arcuate) covered above, two pelvic/proximal-femoral groups are high-yield.
- Muscle/structure pulled off
- Sartorius (and tensor fasciae latae)
- Typical setting
- Sprinting adolescent athlete
- Muscle/structure pulled off
- Rectus femoris (straight head)
- Typical setting
- Kicking sports in adolescents
- Muscle/structure pulled off
- Hamstrings
- Typical setting
- Hurdling/water-skiing; can become chronic painful non-union
- Muscle/structure pulled off
- Abdominal wall muscles
- Typical setting
- Adolescent sudden trunk twist
- Muscle/structure pulled off
- Iliopsoas
- Typical setting
- Adolescent apophyseal avulsion (see pearl for the adult caveat)
Apophyseal avulsions are normal sporting injuries in skeletally immature athletes. But an isolated avulsion of the lesser trochanter in a skeletally mature adult - especially without significant trauma - is pathological (metastasis or marrow-replacing tumour) until proven otherwise, because the iliopsoas should not be able to pull off normal adult bone. This finding mandates a search for an underlying lytic lesion (further imaging, and a primary-tumour/metastasis work-up). It is a classic, easily-dropped exam mark.


Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“An examiner shows you a lateral calcaneal radiograph and asks you to measure the Boehler angle. The angle is 10 degrees.”
“A 19-year-old rugby player has an acute knee injury. The AP knee radiograph shows a small avulsion fragment from the lateral tibial plateau.”
“An examiner shows you an AP wrist radiograph and asks you to identify and explain the significance of a widened gap between the scaphoid and lunate.”
“A 34-year-old man presents after a seizure with a painful shoulder held in internal rotation. He cannot externally rotate the arm. The AP radiograph shows a humeral head that looks abnormally rounded and symmetric, overlapping the glenoid.”
“A 28-year-old sustains a midfoot crush injury. The non-weight-bearing AP foot radiograph shows a tiny bony fleck between the bases of the first and second metatarsals and you are unsure whether the joint is aligned.”
Upper Limb Signs
- Lightbulb sign: rounded humeral head on AP = posterior dislocation (need axillary view)
- Posterior fat pad (elbow): always abnormal = occult fracture in trauma
- Anterior humeral line: middle third of capitellum = normal (supracondylar fracture check)
- Terry Thomas: SL gap more than 3mm = SL dissociation, DISI pattern
- Signet ring: scaphoid flexed, viewed end-on = associated with SL dissociation
Lower Limb Signs
- Segond fracture: lateral tibial plateau avulsion = PATHOGNOMONIC for ACL tear (100%)
- Lipohaemarthrosis: fat-fluid level = intra-articular fracture (most common: tibial plateau)
- Boehler angle: normal 25-40 degrees, less than 20 = displaced calcaneal fracture
- Lisfranc fleck: avulsion between 1st-2nd MT bases = Lisfranc ligament injury (easily missed)
- Medial clear space more than 4mm = deltoid rupture = unstable ankle
Associations to Remember
- Segond = ACL tear (100%) + meniscal tear (75%)
- Calcaneal fracture: bilateral (10%), lumbar spine (10%), wrist fractures
- Monteggia: ulnar fracture + radial head dislocation (check radiocapitellar line)
- Maisonneuve: proximal fibula fracture + syndesmotic disruption + medial ankle
- Posterior dislocation: missed in up to 60% — lightbulb sign is the clue
Evidence Base
Segond Fracture: Lateral Capsular Ligament Avulsion
- The Segond fragment is a small avulsion from the directly lateral surface of the lateral tibial condyle, produced by excessive tension on the lateral capsular ligament.
- The fragment is remarkably constant: elliptical (about 10 x 3 mm), separated by a longitudinal fracture line, lying roughly 4 mm distal to the subarticular cortex.
- A knee haemarthrosis is consistently visible, and the fracture carries a strong association with anterior cruciate ligament rupture.
Anatomy of the Anterolateral Ligament (Segond Substrate)
- The anterolateral ligament (ALL) was identified as a discrete, well-defined structure in 40 of 41 cadaveric knees (97%), distinct from the joint capsule and iliotibial band.
- It originated at the lateral femoral epicondyle and inserted on the anterolateral tibia midway between Gerdy tubercle and the fibular head — the exact site of the Segond fracture.
- By its location it is hypothesised to control internal tibial rotation and modulate the pivot shift, providing the anatomical basis for the Segond fracture.
Lisfranc Fracture-Dislocation: Outcome Depends on Reduction
- Across 76 tarsometatarsal fracture-dislocations, only 49% achieved an excellent or good result, with quality of initial reduction the major determinant of outcome.
- Open reduction and Kirschner-wire internal fixation yielded the best results; direct crush injuries did poorly (1 of 8 good or excellent).
- More than 2 mm of residual displacement or a talometatarsal angle over 15 degrees after closed reduction mandated open reduction.
Operative vs Nonoperative Displaced Intra-articular Calcaneal Fractures
- Landmark multicentre RCT (424 patients, 471 fractures): without stratification, overall functional outcomes (SF-36, VAS) were equivalent between operative and nonoperative care.
- After excluding Workers' Compensation patients, defined subgroups did significantly better with surgery — younger patients, women, comminuted fractures, and those with a moderately low Bohler angle (0-14 degrees).
- Anatomical reduction or a post-reduction step-off of 2 mm or less predicted significantly higher functional scores after surgery.
Elbow Fat Pad Sign and Radiographically Occult Fracture (MRI)
- In 20 adults with a post-traumatic elbow effusion but no visible fracture, MRI revealed a radiographically occult fracture in 75%.
- Most occult fractures were in the radial head (86.6%), with lateral epicondyle and olecranon each accounting for 6.7%; 90% showed bone marrow oedema.
- Effusion size (anterior or posterior fat pad displacement) did NOT correlate with the likelihood of an underlying fracture.
The Often Overlooked Posterior Shoulder Dislocation
- More than 60% of posterior shoulder dislocations are misdiagnosed at initial presentation, with correct diagnosis often delayed for months or years.
- Triggers (seizure, electric shock, fall onto a flexed adducted arm) plus loss of external rotation and abduction should raise suspicion.
- A radiographic trauma series in the scapular plane (with CT if needed) is required to exclude posterior dislocation.