Aggressive vs Non-Aggressive Features & Pattern Recognition
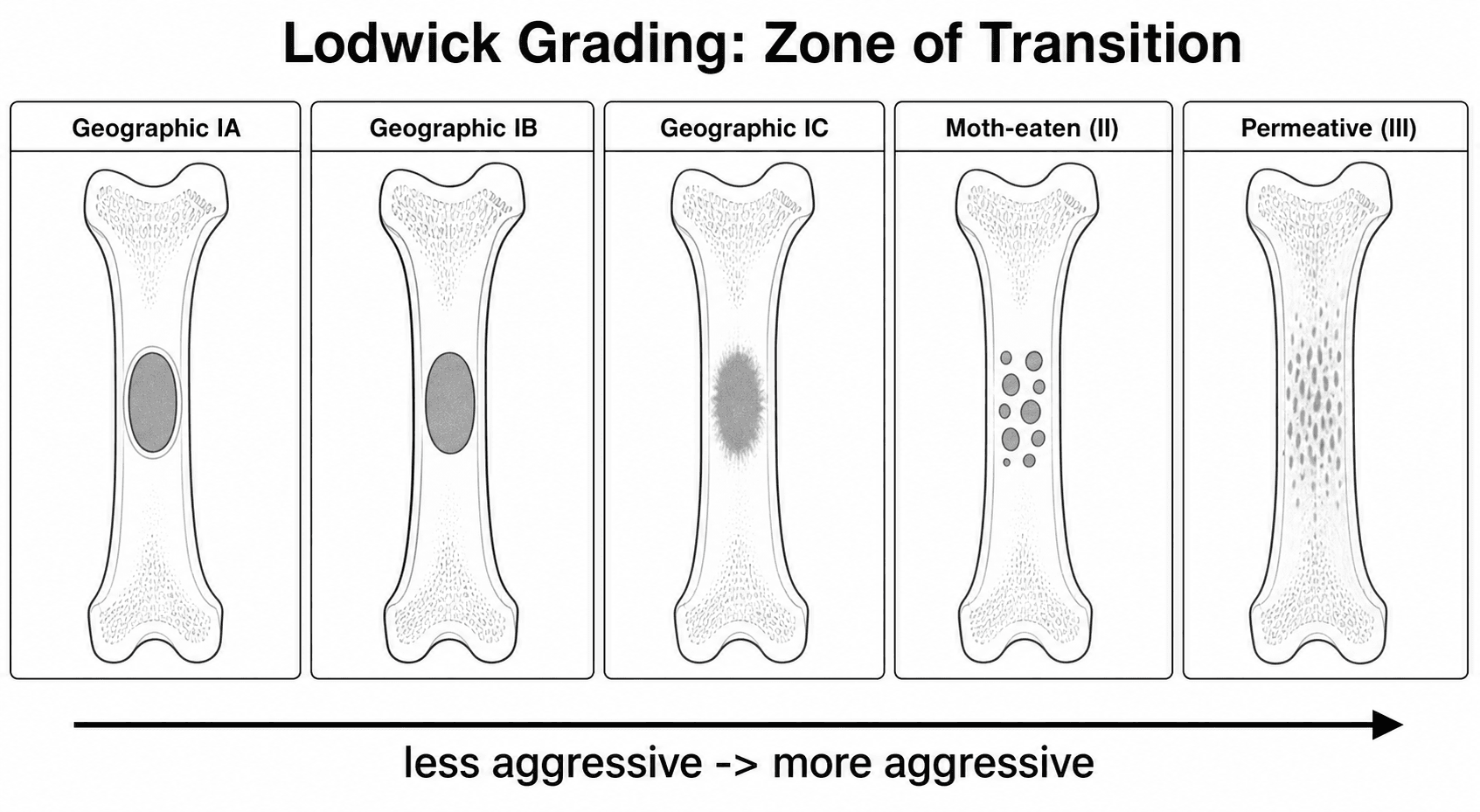
Type IA: Geographic, well-defined sclerotic margin = benign (NOF, enchondroma, SBC)
Type IB: Geographic, well-defined NO sclerotic margin = low-grade malignant or aggressive benign
Type IC: Geographic, ill-defined margin = intermediate aggressiveness
Type II: Moth-eaten (multiple small lytic areas) = moderately aggressive malignancy
Type III: Permeative (cortical destruction, no defined margin) = highly aggressive malignancy
Key: The more well-defined and sclerotic the margin, the less aggressive the lesion
- Lodwick classification determines aggressiveness: geographic (I) = slow-growing, moth-eaten (II) = moderately aggressive, permeative (III) = highly aggressive.
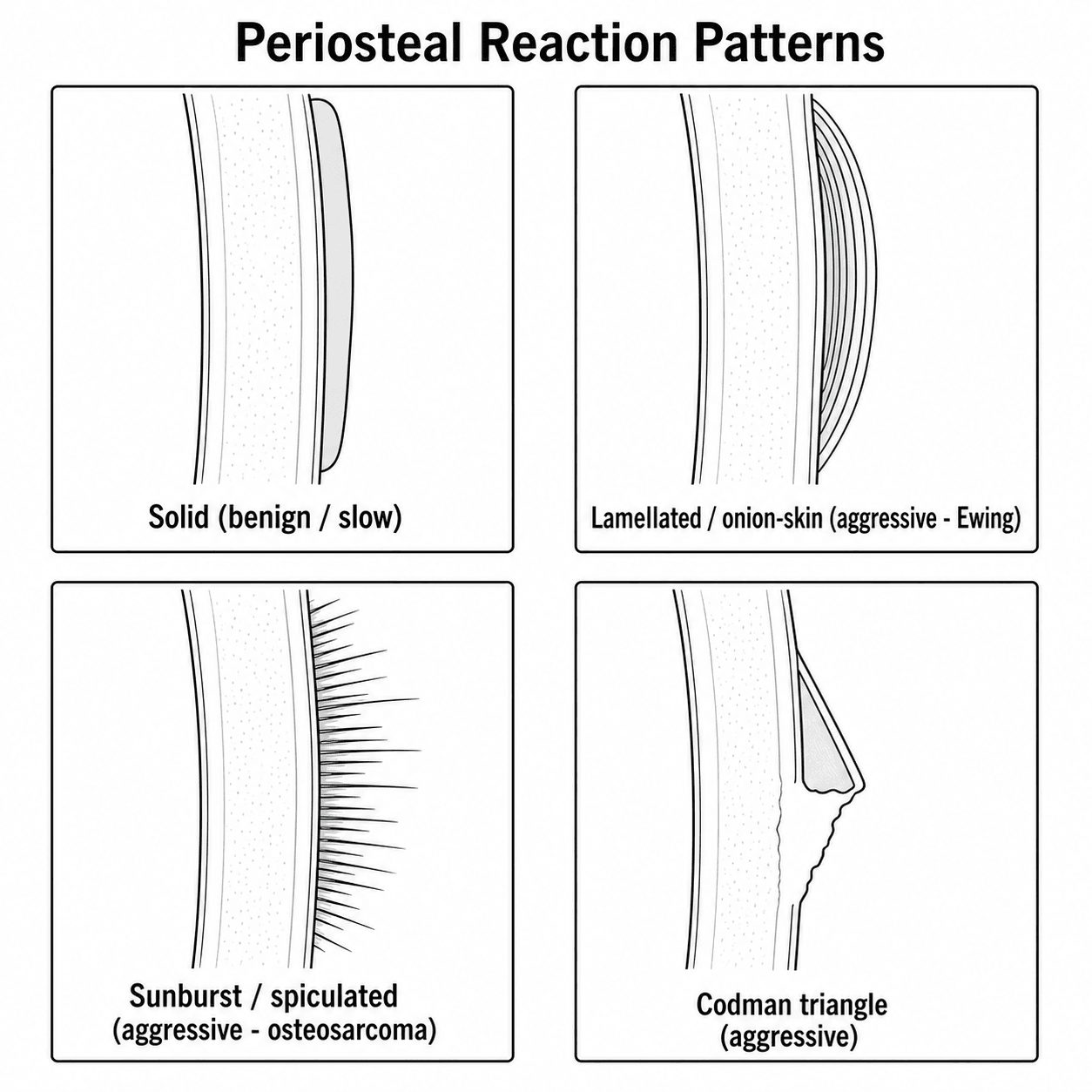
- Codman triangle: periosteum lifted by tumour with reactive bone at the margin — does NOT represent tumour tissue itself (do not biopsy the Codman triangle).
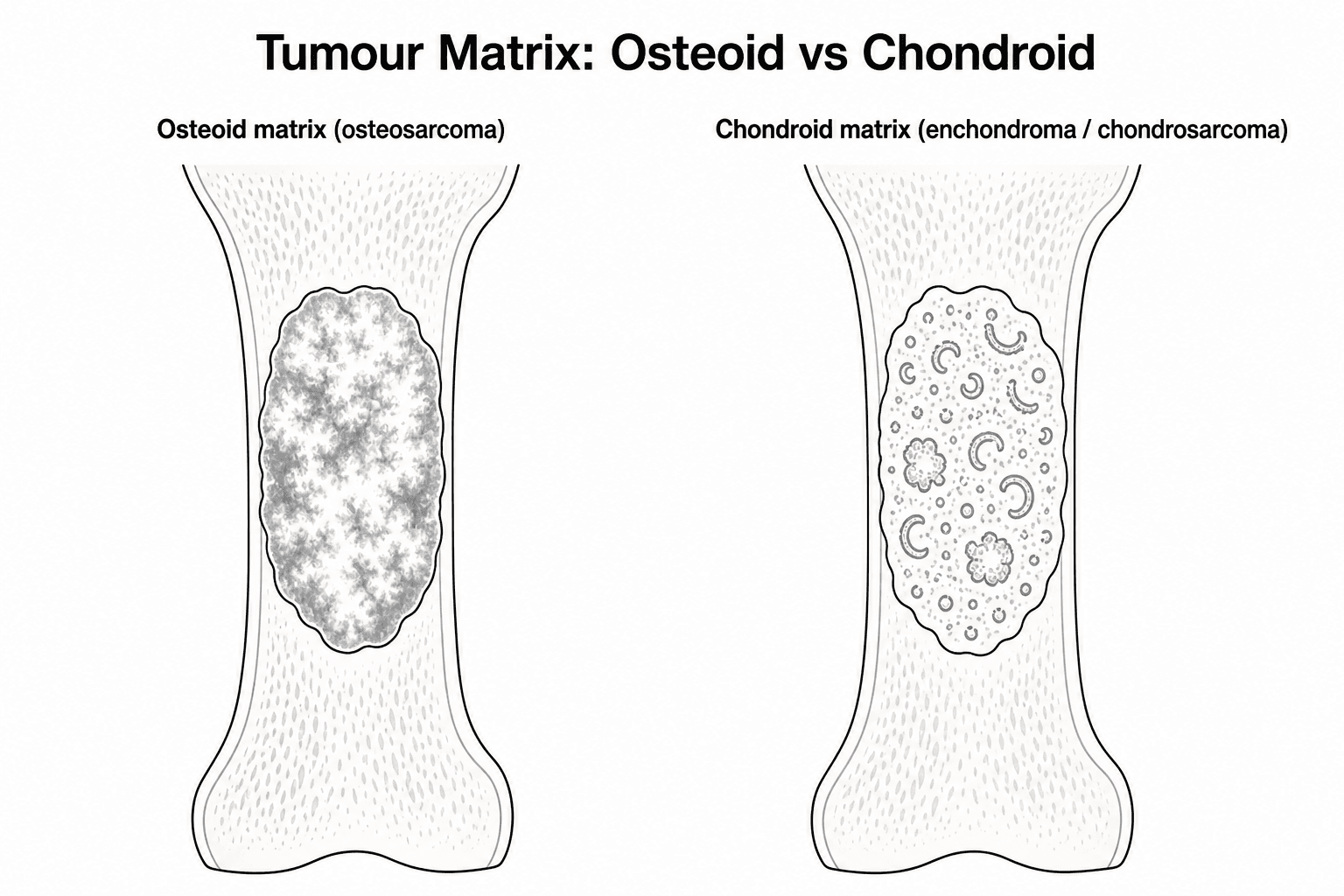
- Matrix mineralisation pattern: chondroid (rings and arcs, stippled) vs osteoid (cloud-like, dense) — helps narrow the differential.
- Tumour location within the bone: epiphysis (GCT, chondroblastoma), metaphysis (osteosarcoma, chondrosarcoma), diaphysis (Ewing, lymphoma, fibrous dysplasia).
- MRI is essential for local staging: intramedullary extent, soft tissue mass, skip lesions, neurovascular involvement.
- “GCT: subarticular (epiphysis touching articular surface), eccentric, lytic, NO matrix mineralisation. Peak age 20-40. Knee region most common.
- “Osteosarcoma: metaphyseal, mixed lytic/scite, cloud-like osteoid matrix, Codman triangle, sunburst periosteal reaction. Peak age 10-25.
- “Ewing sarcoma: diaphyseal in children, permeative, lamellated (onion-skin) periosteal reaction, large soft tissue mass. Peak age 5-15.
- “Chondrosarcoma: medullary, rings and arcs calcification, endosteal scalloping more than two-thirds cortex, NO periosteal reaction (slow-growing).
- “Metastases are the MOST COMMON malignant bone tumour in adults over 40 (primary malignant tumours are rare at this age).
Bone tumour radiological assessment is one of the highest-yield examination topics. You must be able to: classify aggressiveness using Lodwick criteria, identify periosteal reaction patterns, recognise matrix mineralisation, describe tumour location within bone, and outline the staging imaging pathway. Classic traps: not considering metastases as the most common malignant bone tumour in adults over 40, and confusing the Codman triangle with tumour tissue (it is reactive periosteum — do not biopsy it).
MAPLESBone Tumour Aggressiveness Assessment
Hook:MAPLES: the systematic approach to bone tumour radiograph assessment — Margin, Age, Periosteal reaction, Location, Expansion, Struck-through matrix.
SCOLHPeriosteal Reaction Patterns
Hook:SCOLH: periosteal reactions from most aggressive to least — Sunburst, Codman, Onion-skin, Lobulated, Hair-on-end.
EpiMeDiCommon Tumours by Location in Bone
Hook:EpiMeDi: Epiphysis-Metaphysis-Diaphysis — know which tumours favour which location.
Overview
Radiological assessment of bone tumours requires a systematic approach that integrates multiple imaging features to narrow the differential diagnosis and determine aggressiveness. The key principles are: (1) assess the margin of the lesion (Lodwick classification), (2) evaluate the periosteal reaction pattern, (3) identify the matrix mineralisation, (4) note the location within the bone and the skeleton, and (5) consider the patient's age. These five features, assessed together, significantly narrow the differential diagnosis and guide further investigation.
The single most important radiographic feature is the MARGIN of the lesion, classified by Lodwick: Type IA — geographic destruction with a well-defined sclerotic rim. This is the classic appearance of benign lesions (non-ossifying fibroma, enchondroma, simple bone cyst). The sclerotic rim indicates the host bone is keeping pace with the lesion's growth. Type IB — geographic destruction with a well-defined margin but NO sclerotic rim. This suggests a low-grade malignancy or aggressive benign lesion (GCT, chondrosarcoma). Type IC — geographic with an ill-defined margin. Intermediate aggressiveness. Type II — moth-eaten pattern (multiple small lytic areas without defined margins). Moderately aggressive malignancy. Type III — permeative pattern (cortical destruction without any defined lesion margin). Highly aggressive — Ewing sarcoma, osteosarcoma, lymphoma, metastases.
When a bone tumour is suspected: (1) Plain radiograph: ALWAYS the first investigation. Provides the most diagnostic information for pattern recognition. (2) MRI of the ENTIRE involved bone (including the joint above and below): shows intramedullary extent, soft tissue mass size, skip lesions, and neurovascular relationship. Essential for surgical planning. (3) CT chest: MUST be performed for pulmonary metastasis staging (the lungs are the most common site of metastasis for primary bone tumours). (4) Bone scan or PET-CT: for skeletal staging (detecting other skeletal lesions). (5) CT-guided biopsy: for histological diagnosis. CRITICAL: the biopsy tract must be planned with the surgeon who will perform the definitive surgery — a poorly placed biopsy contaminates tissue planes and may compromise limb salvage surgery.
From Imaging to Staging: Enneking System and Surgical Margins
Radiological assessment does not end at a diagnosis — it feeds directly into surgical staging, which determines the resection required. The Enneking (Musculoskeletal Tumor Society) system stages MALIGNANT lesions on three variables, each supplied largely by imaging and biopsy: histological Grade (G), anatomic site or compartment (T) and Metastasis (M). MRI of the whole bone defines T (intra- versus extra-compartmental), CT chest with bone scan or PET-CT defines M, and the biopsy supplies G.
- Grade (G) / Site (T) / Metastasis (M)
- G1 (low) · T1 (intracompartmental) · M0
- Meaning
- Low-grade, confined within a compartment, no metastasis
- Grade (G) / Site (T) / Metastasis (M)
- G1 (low) · T2 (extracompartmental) · M0
- Meaning
- Low-grade but breached the compartment (e.g. cortex/soft tissue)
- Grade (G) / Site (T) / Metastasis (M)
- G2 (high) · T1 (intracompartmental) · M0
- Meaning
- High-grade, still intracompartmental
- Grade (G) / Site (T) / Metastasis (M)
- G2 (high) · T2 (extracompartmental) · M0
- Meaning
- High-grade and extracompartmental — the commonest presenting stage of high-grade sarcoma
- Grade (G) / Site (T) / Metastasis (M)
- Any G · any T · M1
- Meaning
- Regional or distant metastasis (including skip lesions or nodes) — worst prognosis
A separate Enneking scheme grades BENIGN lesions by aggression: Stage 1 latent (e.g. non-ossifying fibroma — self-limiting, observe), Stage 2 active (e.g. aneurysmal bone cyst — grows, treated with extended curettage) and Stage 3 aggressive (e.g. many giant cell tumours — locally destructive, may breach cortex). The newer AJCC system stages bone sarcoma instead on grade plus tumour SIZE (with an 8 cm threshold) and the presence of skip or distant metastases, which is why both can be quoted in a viva.
The stage then dictates the surgical MARGIN — the four Enneking margins describe the plane of excision relative to the tumour and its reactive zone, and each carries a characteristic local recurrence risk:
- Plane of dissection
- Through the tumour itself (piecemeal / curettage)
- Typical use & local recurrence risk
- Benign active/aggressive lesions (e.g. GCT curettage with adjuvant); leaves macroscopic disease — high recurrence if used for sarcoma
- Plane of dissection
- Through the reactive pseudocapsule
- Typical use & local recurrence risk
- May leave satellite nodules within the reactive zone; adequate for many benign lesions, inadequate alone for high-grade sarcoma
- Plane of dissection
- En bloc with a cuff of normal tissue, within the compartment
- Typical use & local recurrence risk
- Standard limb-salvage margin for sarcoma; leaves skip lesions if they lie beyond the resection — hence whole-bone MRI
- Plane of dissection
- Removes the entire compartment(s)
- Typical use & local recurrence risk
- Highest local control, greatest morbidity; reserved for extensive disease where a wide margin is not achievable
Imaging, staging and margin are one continuous decision. The whole-bone MRI that you request to "stage T" is the same scan that detects the skip lesion which would render a planned wide margin inadequate — and the biopsy that supplies G must be placed in the line of the future wide-margin excision. This is why a poorly planned biopsy (Mankin) and an under-staged tumour both end in the same place: an inadequate margin and local recurrence.
Systematic Approach
Bone Tumour Pattern Recognition
- Radiographic Features
- Metaphyseal, mixed lytic/sclerotic, cloud-like osteoid matrix, Codman triangle, sunburst periosteal reaction
- Key Distinguishing Feature
- Cloud-like mineralisation + aggressive periosteal reaction. Peak age 10-25. Around knee (60%)
- Radiographic Features
- Diaphyseal (in children), permeative, lamellated (onion-skin) periosteal reaction, LARGE soft tissue mass
- Key Distinguishing Feature
- Permeative destruction + large soft tissue mass disproportionate to bone lesion. Peak age 5-15
- Radiographic Features
- Medullary, rings and arcs calcification, endosteal scalloping more than two-thirds cortex, NO periosteal reaction
- Key Distinguishing Feature
- Rings and arcs matrix + endosteal scalloping. Peak age 40-60. Slow-growing, rarely metastasises
- Radiographic Features
- Subarticular (epiphyseal), eccentric, well-defined lytic, NO matrix, NO sclerotic rim (Lodwick IB)
- Key Distinguishing Feature
- Epiphyseal location touching articular surface in CLOSED physis. Peak age 20-40. Knee region
- Radiographic Features
- Central metaphyseal, well-defined lytic, thin sclerotic rim, fallen fragment sign (pathological fracture)
- Key Distinguishing Feature
- Central location. Fallen fragment sign = fragment falls to dependent portion of cyst. Age 5-15
- Radiographic Features
- Eccentric metaphyseal, well-defined scalloped sclerotic rim, cortically based (bubbly)
- Key Distinguishing Feature
- Most common incidental bone lesion. Lodwick IA. Cortical thinning without breach. Age 10-20. No treatment
- Radiographic Features
- Central, well-defined lytic with rings and arcs calcification, NO periosteal reaction, hands most common
- Key Distinguishing Feature
- Chondroid matrix (rings and arcs) in a small bone of the hand = virtually diagnostic. No treatment unless symptomatic
- Radiographic Features
- Over 40 years. Lytic (most), blastic (prostate, breast), or mixed. Pedicle destruction on spine (winking owl)
- Key Distinguishing Feature
- MOST COMMON malignant bone tumour in adults over 40. Usually multiple. Common primary: lung, breast, kidney, thyroid, prostate
Differential Diagnosis of the Lytic Bone Lesion
A purely lytic lesion with no matrix is one of the commonest exam challenges. Use age and location to narrow the list, then apply the MAPLES aggressiveness features. The mnemonic FEGNOMASHIC (Fibrous dysplasia, Enchondroma, Giant cell tumour, Non-ossifying fibroma, Osteoblastoma, Metastases/Myeloma, ABC, Solitary bone cyst, Hyperparathyroidism/brown tumour, Infection, Chondroblastoma) lists the classic causes; the table below distils the high-yield discriminators.
- Typical age & location
- 20-40, epiphysis-metaphysis to subarticular surface (closed physis)
- Discriminating feature(s)
- Eccentric, no sclerotic rim, no matrix; reaches articular surface
- Typical age & location
- Under 20, eccentric metaphysis
- Discriminating feature(s)
- Expansile blown-out shell; fluid-fluid levels on MRI (non-specific — exclude telangiectatic osteosarcoma)
- Typical age & location
- 5-15, central proximal humerus/femur metaphysis
- Discriminating feature(s)
- Central, mildly expansile, fallen-fragment sign after fracture
- Typical age & location
- Any adult, often multiple
- Discriminating feature(s)
- Subperiosteal resorption, raised calcium/PTH — biochemistry is the clue
- Typical age & location
- Over 40, axial and proximal long bones
- Discriminating feature(s)
- Multiple lesions; myeloma classically cold on bone scan; known primary
- Typical age & location
- Children/young adults, metaphysis
- Discriminating feature(s)
- Penumbra sign on T1 MRI, clinical sepsis/raised inflammatory markers
- Typical age & location
- 10-25, epiphysis in OPEN physis
- Discriminating feature(s)
- Stippled chondroid calcification, surrounding marrow oedema
A solitary lytic lesion in a patient over 40 is a metastasis or myeloma until proven otherwise — but never assume. A single destructive lesion with no known primary must still be staged and biopsied through a sarcoma pathway, because a solitary primary sarcoma can masquerade as a metastasis, and biopsying it incorrectly can compromise limb salvage.
Differential Diagnosis of the Sclerotic (Blastic) Bone Lesion
The lytic lesion gets most of the attention, but a focally DENSE (sclerotic) lesion is an equally common examiner challenge — and the same MAPLES discipline applies (margin, age, periosteal reaction, location, matrix). Sclerosis can be the lesion's own matrix (osteoid in osteosarcoma, reactive bone around an osteoid osteoma nidus), reactive host bone walling off a slow lesion, or the healing phase of a previously lytic lesion (fibrous dysplasia, non-ossifying fibroma, treated bone cyst). The single most important step is to decide whether a solitary dense focus is a harmless bone island or an osteoblastic metastasis.
- Typical setting
- Incidental, any age
- Discriminating feature(s)
- Ovoid dense focus with a spiculated 'brush border' blending into trabeculae; cold or only mildly warm on bone scan; stable over time
- Typical setting
- Over 40; prostate and breast classically blastic
- Discriminating feature(s)
- Often multiple, ill-defined; usually HOT on bone scan; known or sought primary; pedicle sclerosis or an 'ivory' vertebra
- Typical setting
- Adolescent / young adult; night pain relieved by NSAIDs
- Discriminating feature(s)
- Small lucent nidus (under 1.5 cm) with surrounding reactive sclerosis; intense focal uptake (double-density sign)
- Typical setting
- 10-25; metaphysis around the knee
- Discriminating feature(s)
- Cloud-like osteoid matrix, cortical destruction, aggressive periosteal reaction (sunburst, Codman) — sclerosis here is tumour bone, not reactive
- Typical setting
- Steroids, alcohol, sickle cell, caisson disease
- Discriminating feature(s)
- Serpiginous sclerotic rim around a lucent centre; medullary; no soft-tissue mass (sarcomatous change is rare but a red flag)
- Typical setting
- Over 55; pelvis, spine, skull, femur
- Discriminating feature(s)
- Cortical and trabecular thickening with bone ENLARGEMENT; 'flame / blade-of-grass' advancing front; raised alkaline phosphatase
- Typical setting
- Adult; can be lytic, sclerotic or mixed
- Discriminating feature(s)
- Permeative destruction with a disproportionately large soft-tissue mass; sclerosis may follow treatment
A solitary dense focus is a bone island until the bone scan, serial films or cross-sectional imaging suggest otherwise; a cold, stable, brush-border lesion needs no further action. The trap is the OPPOSITE error — calling an early osteoblastic metastasis or a sclerotic osteosarcoma a bone island. Multiplicity, ill-defined margins, intense uptake, cortical destruction or a soft-tissue mass move the lesion out of the benign box and into the staging and biopsy pathway.
Guidelines, Registries & Global Practice
Primary bone sarcomas are rare worldwide (roughly 0.8 to 1 per 100,000 per year), so the diagnostic challenge is recognising the aggressive radiological signs early and referring before any intervention. By contrast, metastases, myeloma and lymphoma are far more common bone malignancies in adults over 40 and dominate the differential at that age. Across every major health system the principle is identical: image first with a plain radiograph, characterise the lesion, then stage and refer to a specialist sarcoma multidisciplinary team (MDT) BEFORE biopsy.
- Imaging & staging emphasis
- Plain radiograph first-line; whole-bone MRI for local staging; CT chest for pulmonary staging
- Referral / biopsy stance
- Suspected primary bone sarcoma referred to a recognised bone sarcoma diagnostic centre; biopsy at (or directed by) the treating centre
- Imaging & staging emphasis
- MRI of whole compartment plus chest CT; biopsy planned along the future resection line
- Referral / biopsy stance
- Diagnosis, biopsy and treatment in a reference sarcoma centre or expert network
- Imaging & staging emphasis
- MRI with/without contrast of primary site; chest CT; PET-CT or bone scan for systemic staging
- Referral / biopsy stance
- Image-guided or open biopsy at the institution that will deliver definitive treatment
- Imaging & staging emphasis
- Cross-sectional staging before any intervention
- Referral / biopsy stance
- Biopsy tract must be excisable en bloc; refer before biopsy (basis: Mankin hazards-of-biopsy data)
Registry and outcome data reinforce a single global standard of care: centralised, MDT-based treatment improves limb-salvage and survival, and poorly planned biopsy outside a specialist centre measurably increases amputation and complication rates (Musculoskeletal Tumor Society data). National sarcoma registries and reference networks (for example in the UK, the Scandinavian Sarcoma Group, and European reference networks such as EURACAN) collect implant, margin and survival outcomes that underpin these recommendations.
In high-resource settings whole-bone MRI, chest CT and PET-CT are routine and biopsy is typically image-guided at the treating centre. In limited-resource settings where MRI or PET access is constrained, plain radiography and the systematic MAPLES assessment carry even greater weight for triage, ultrasound may guide biopsy, and the priority becomes early recognition of aggressive signs and timely referral to the nearest sarcoma unit rather than local biopsy. The diagnostic reasoning does not change with geography — only the available tools do.
Controversies & Areas of Uncertainty
The single most contentious area in bone tumour imaging. There is no fully reliable radiological or even histological boundary between an enchondroma and a low-grade cartilage tumour. Deep endosteal scalloping (over two-thirds of cortical thickness), lesion length, lesion-related pain, cortical destruction and a soft-tissue mass favour an atypical cartilaginous tumour / grade 1 chondrosarcoma, but each sign is less sensitive for low-grade than high-grade disease (Douis 2017). Dynamic contrast-enhanced MRI has NOT proven discriminatory. Many incidental small asymptomatic chondroid lesions in long bones are now followed rather than biopsied.
Peritumoural high T2 signal may represent oedema rather than infiltrating tumour, so MRI can overestimate intramedullary extent (a recognised limitation of the Bloem staging data). This matters for planning resection margins; surgeons correlate MRI with the histology of the resected specimen and increasingly use the marrow signal interface rather than the oedema edge to define the margin.
Technetium-99m bone scintigraphy remains widely used for skeletal staging, but FDG PET-CT offers better characterisation of metabolic activity, response assessment and detection of soft-tissue and nodal disease. Access, cost and local protocol drive the choice, and guidelines differ on whether PET-CT is routine or selective. Myeloma is a key caveat — it is frequently photopenic ("cold") on bone scan, so skeletal survey, whole-body MRI or PET-CT is preferred.
Open biopsy was historically the reference standard, but CT- or ultrasound-guided core needle biopsy at a specialist centre now achieves comparable diagnostic yield with lower morbidity for most lesions. The non-negotiable principle from the Mankin data is unchanged: whoever performs the biopsy must place the tract so it can be excised en bloc with the definitive resection, ideally planned by the operating surgeon.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“An examiner shows you a radiograph of the distal femur in a 16-year-old boy with knee pain. The radiograph shows a mixed lytic and sclerotic lesion in the metaphysis with cloud-like mineralisation, cortical destruction, and a Codman triangle.”
“A 30-year-old woman presents with a lytic lesion in the proximal tibial epiphysis that extends to the articular surface. There is no matrix mineralisation.”
“An examiner asks you to describe the systematic approach to assessing a bone tumour on a plain radiograph.”
MAPLES Systematic Assessment
- Margin (Lodwick): IA (sclerotic = benign), IB-IC (no sclerosis), II (moth-eaten), III (permeative)
- Age: under 5 (LCH, neuroblastoma), 5-25 (Ewing, OS), 20-40 (GCT), over 40 (METASTASES)
- Periosteal: solid (benign), onion-skin (Ewing), sunburst (OS), Codman triangle (aggressive)
- Location: epi (GCT), meta (OS, SBC), dia (Ewing). Position: central vs eccentric
- Matrix: cloud-like = osteoid (OS), rings/arcs = chondroid (enchondroma/CS), none = GCT/mets
Classic Tumour Patterns
- Osteosarcoma: metaphyseal, cloud-like matrix, sunburst, Codman, age 10-25, around knee
- Ewing: diaphyseal, permeative, onion-skin, LARGE soft tissue mass, age 5-15
- GCT: subarticular epiphyseal, eccentric, lytic, NO matrix, Lodwick IB, age 20-40
- Enchondroma: central, rings/arcs, hands. Chondrosarcoma: same matrix but endosteal scalloping
- Metastases: most common malignant tumour over 40. Lytic (most), blastic (prostate/breast)
Staging Protocol
- MRI: entire involved bone (skip lesions), soft tissue extent, NV bundle
- CT chest: ESSENTIAL (pulmonary mets = most common site for primary bone tumours)
- Bone scan/PET-CT: skeletal staging (other bone lesions)
- Biopsy: REFER to sarcoma centre FIRST. Tract must be excisable en bloc
- Codman triangle = reactive periosteum — do NOT biopsy it
Evidence Base
MRI is the Modality of Choice for Local Staging of Primary Bone Sarcoma
- Prospective comparison of MRI, CT, technetium-99m bone scintigraphy and angiography against pathological examination of resected specimens in 56 patients with primary bone sarcoma.
- MRI was significantly superior to CT and scintigraphy in defining intraosseous tumour length, and significantly superior to CT in demonstrating muscle compartment involvement.
- MRI was as accurate as CT for cortical and joint involvement and was the best modality for displaying the relationship between tumour and major neurovascular bundles.
Lodwick Grading of Bone Lesion Growth Rate from Radiographs
- Established that the radiographic rate of growth divides focal bone lesions into two largely mutually exclusive classes — slow-growing (likely benign) and rapidly growing (likely malignant).
- Defined a five-grade system based on the pattern and margin of bone destruction (geographic, moth-eaten, permeative) with statistical validation of grading as an expression of growth rate.
- Grading helps decide which lesions require biopsy and which may be safely observed.
Staging imaging evidence guides the assessment of bone tumours.