From Fat Pad Signs to Advanced MRI Assessment
Radiography: First-line for ALL elbow presentations. AP + lateral minimum in trauma
Ultrasound: Dynamic ligament assessment, effusion detection, guided injection
MRI: Gold standard for ligaments (UCL/LCL), tendons, OCD, bone marrow oedema
CT: Complex fracture characterisation (coronoid, radial head comminution), terrible triad planning
MR Arthrography: Osteochondral lesion staging, intra-articular loose bodies
Key: Start with radiographs. CT for fracture detail. MRI for soft tissue pathology.
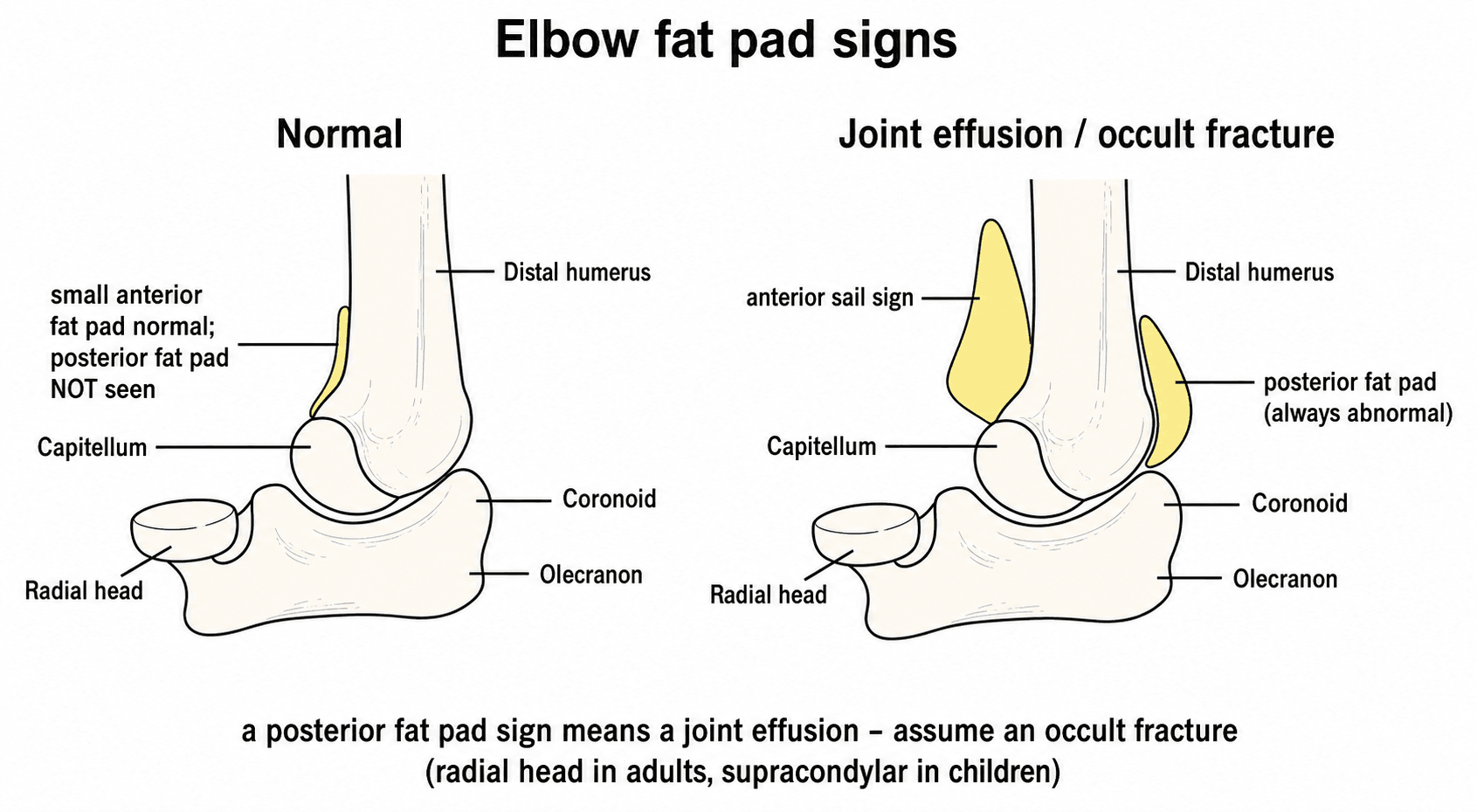
- The posterior fat pad sign on lateral radiograph indicates an intra-articular effusion and, in the setting of trauma, represents an OCCULT FRACTURE until proven otherwise.
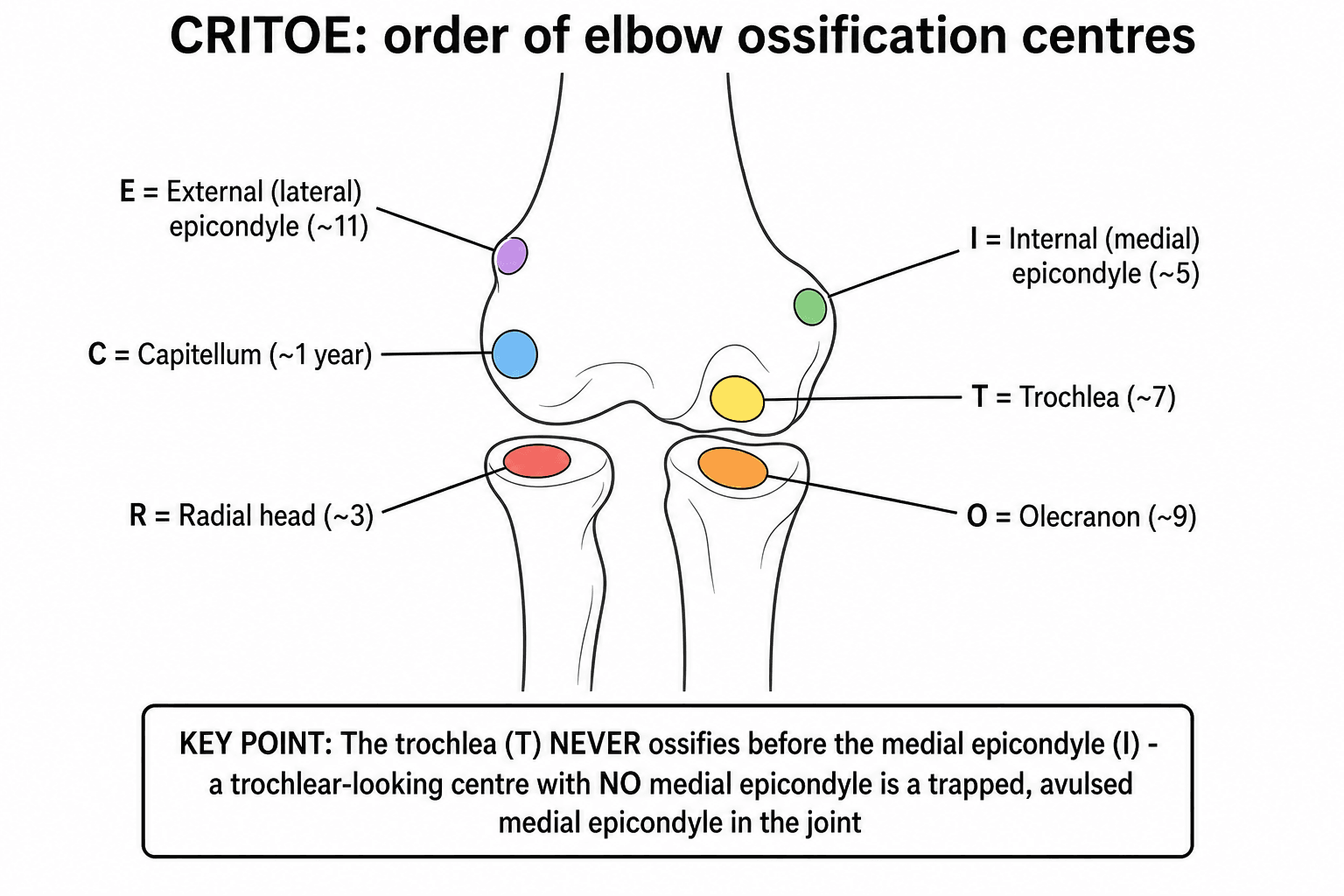
- CRITOE: the sequence of ossification centre appearance — Capitellum (1yr), Radial head (3yr), Internal (medial) epicondyle (5yr), Trochlea (7yr), Olecranon (9yr), External (lateral) epicondyle (11yr).
- Two views are the MINIMUM for elbow trauma: AP and lateral. Oblique views may be added for specific indications.
- MRI is the gold standard for assessment of collateral ligaments (UCL, LCL complex), tendon pathology, and osteochondral lesions.
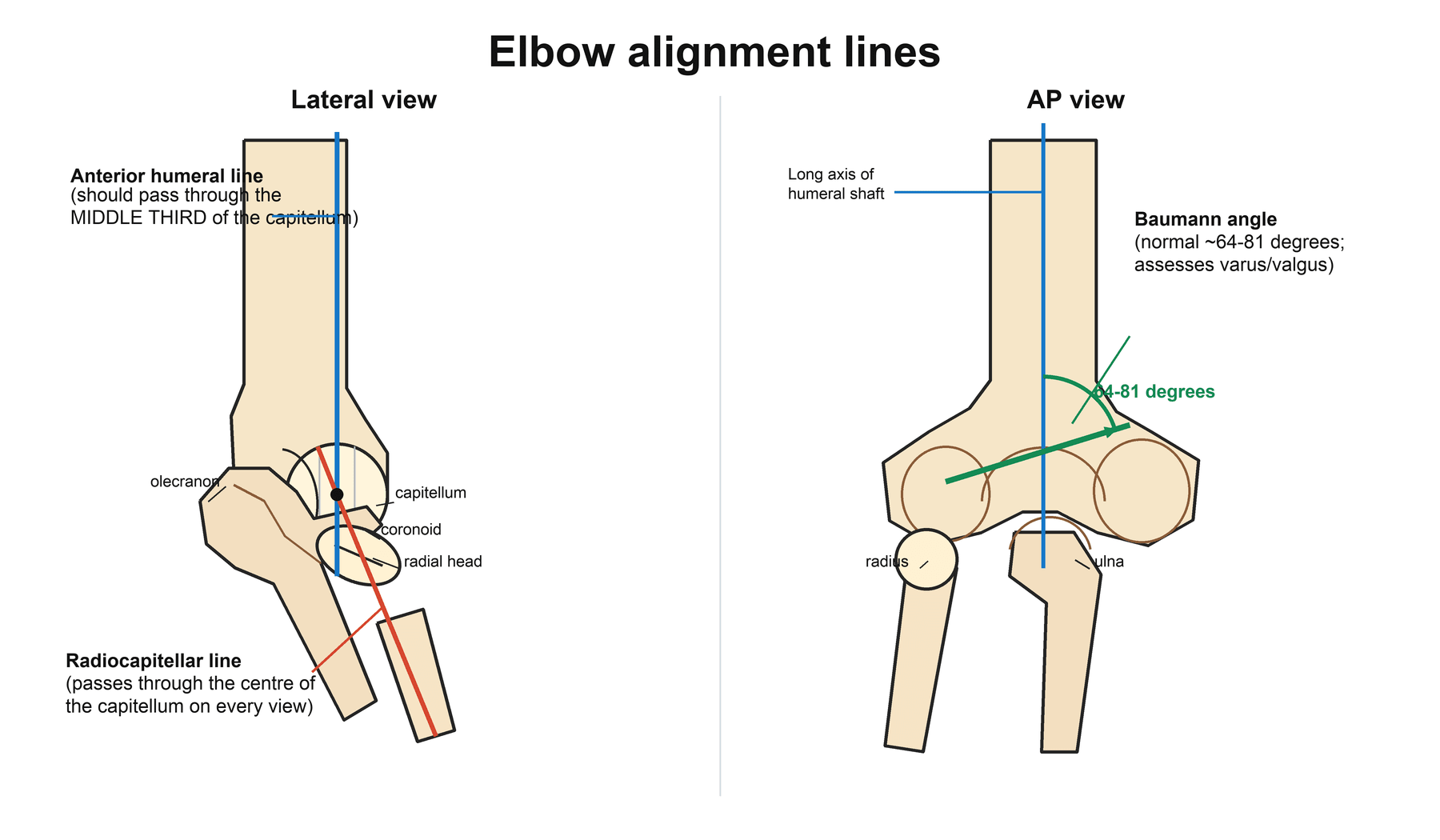
- The anterior humeral line on a true lateral should pass through the middle third of the capitellum — posterior displacement indicates a supracondylar fracture with posterior angulation.
- “Posterior fat pad sign + no visible fracture = radial head fracture (most common occult elbow fracture in adults) or supracondylar fracture (in children).
- “The radiocapitellar line: a line drawn through the radial shaft should bisect the capitellum on ALL views — failure indicates radial head subluxation/dislocation (Monteggia).
- “The carrying angle (normal 5-15 degrees valgus) is measured on the AP view — increased after malunited lateral condyle fracture (cubitus valgus).
- “UCL injury (Tommy John): MRI shows high T2 signal or disruption of the anterior bundle of the medial UCL at its sublime tubercle insertion.
- “Olecranon stress fractures in throwing athletes show focal uptake on bone scan and subtle lucency on CT — MRI shows marrow oedema.
Elbow imaging is very commonly tested, particularly in the context of paediatric trauma (supracondylar fractures, ossification centres), the posterior fat pad sign, and the radiocapitellar line. You must be able to: identify all ossification centres (CRITOE), recognise fat pad signs, assess the anterior humeral line, and apply the radiocapitellar line on all views. Classic traps: dismissing a posterior fat pad sign as normal, confusing ossification centres with avulsion fractures, and not recognising a Monteggia fracture-dislocation.
POSTFat Pad Signs
Hook:POST: the Posterior fat pad sign is the most important — ALWAYS abnormal and indicates occult fracture in trauma.
Overview
Systematic elbow imaging is a critical examination skill, particularly in the context of trauma assessment in both adults and children. The elbow's complex anatomy — three articulations (ulnohumeral, radiocapitellar, proximal radioulnar), six ossification centres in children, and close proximity of neurovascular structures — makes systematic radiographic assessment essential.
The key principle is that elbow radiographs must be read systematically, paying particular attention to the fat pad signs (the most sensitive radiographic indicator of intra-articular pathology), alignment lines (anterior humeral line, radiocapitellar line), and ossification centres in children.
The elbow is challenging to image because: (1) complex overlapping bony anatomy requires precise positioning for true AP and lateral views, (2) paediatric ossification centres appear sequentially and can mimic fractures, (3) subtle fractures (radial head, coronoid) are easily missed, (4) the fat pad signs provide indirect evidence of fracture when direct visualisation fails, (5) ligament injuries (UCL, LCL complex) require MRI and are not visible on radiographs, (6) the terrible triad (dislocation + radial head fracture + coronoid fracture) requires CT for full characterisation and surgical planning.
The posterior fat pad sign is the single most important radiographic sign in elbow trauma. The posterior fat pad is tucked into the olecranon fossa and is normally NOT visible on a true lateral radiograph. When joint distension (effusion or haemarthrosis) pushes the fat pad out of the fossa, it becomes visible as a small lucent line behind the distal humerus. In the context of trauma, this sign indicates an intra-articular fracture even when no fracture line is visible — most commonly a radial head fracture in adults or a supracondylar fracture in children. Management: treat the patient as having a fracture (immobilisation, follow-up radiographs at 7-10 days, or CT/MRI if clinical concern persists).
Systematic Approach
Systematic Elbow Imaging Assessment
- First-Line Imaging
- AP + true lateral radiographs. Assess fat pads, radiocapitellar line, visible fractures
- Advanced Imaging
- CT for complex fractures (radial head comminution, coronoid, terrible triad planning). MRI for occult fracture, ligament injury
- First-Line Imaging
- AP + lateral radiographs. Compare with contralateral side if uncertain
- Advanced Imaging
- MRI (without contrast) for clinically significant injury with normal radiographs. Ultrasound for supracondylar fracture effusion
- First-Line Imaging
- AP radiograph (medial joint space widening under stress)
- Advanced Imaging
- MRI: gold standard for UCL assessment (anterior bundle at sublime tubercle). MR arthrography for partial tears
- First-Line Imaging
- Radiographs usually normal (calcification occasionally)
- Advanced Imaging
- Ultrasound: hypoechoic tendon, neovascularisation, tears. MRI if USS equivocal or pre-surgical planning
- First-Line Imaging
- AP radiograph: lucency or irregularity of capitellum
- Advanced Imaging
- MRI: gold standard for staging (intact cartilage cap vs unstable fragment). MR arthrography for loose body detection
- First-Line Imaging
- Lateral + oblique radiographs (extent of HO, joint congruence)
- Advanced Imaging
- CT for surgical planning of HO excision. 3D reconstruction for complex anatomy
FABLESystematic Elbow Radiograph Assessment
Hook:FABLE: the five-point systematic elbow radiograph assessment for trauma.
Radiographic Assessment
Key Alignment Lines and Angles
Anterior humeral line: Drawn along the anterior cortex of the distal humerus on the TRUE lateral view. This line should pass through the MIDDLE THIRD of the capitellum. If the line passes through the anterior third or misses the capitellum entirely, this indicates posterior displacement of the capitellum relative to the humeral shaft — consistent with a posteriorly displaced supracondylar fracture. This is the most important line for assessing supracondylar fracture reduction.
Radiocapitellar line: A line drawn through the centre of the radial shaft and proximal radius should pass through the centre of the capitellum on ALL views (AP, lateral, and oblique). If this line does not bisect the capitellum on ANY view, the radial head is dislocated. This is the key to diagnosing Monteggia fracture-dislocation: an ulnar shaft fracture with an associated radial head dislocation (the ulnar fracture may be subtle, and the dislocation may only be apparent on one view).
Baumann angle: Measured on the AP view between the lateral condylar physis and the long axis of the humeral shaft. Normal range: 64-81 degrees (average approximately 75 degrees). Used to assess varus/valgus alignment after supracondylar fracture reduction. A decrease in the Baumann angle compared to the contralateral side suggests varus malreduction (cubitus varus or 'gunstock deformity').
Carrying angle: Measured on the AP view between the long axis of the humerus and the long axis of the forearm (ulna). Normal: 5-15 degrees of valgus (slightly higher in females). Increased carrying angle (cubitus valgus) is associated with malunited lateral condyle fractures and may cause delayed ulnar nerve palsy.
Radiographic Differential of the Painful/Injured Elbow
A positive fat pad sign or abnormal alignment line is a starting point, not a diagnosis. The table below maps the common radiographic appearances to their differentials and the discriminating feature that resolves them.
- Key differentials
- Radial head/neck fracture; coronoid fracture; capitellar fracture; non-traumatic effusion (septic/inflammatory arthritis)
- Discriminating feature / next step
- Mechanism + focal tenderness. Radial head fracture most likely; if non-traumatic consider aspiration. CT or MRI if management depends on confirmation
- Key differentials
- Supracondylar fracture; lateral condyle fracture; radial neck fracture; proximal ulna fracture
- Discriminating feature / next step
- Check anterior humeral line (supracondylar) and lateral column (lateral condyle). Treat as occult fracture; review at 7-10 days
- Key differentials
- Monteggia fracture-dislocation; congenital radial head dislocation; chronic/missed dislocation
- Discriminating feature / next step
- Congenital/chronic shows a dome-shaped (convex) radial head and hypoplastic capitellum; acute Monteggia has an ulnar fracture or plastic bow
- Key differentials
- Trapped medial epicondyle; normal trochlear ossification centre; intra-articular loose body
- Discriminating feature / next step
- Apply CRITOE: trochlea cannot ossify before the medial epicondyle — if the epicondyle is absent, the fragment IS the epicondyle (intra-articular)
- Key differentials
- OCD of capitellum; Panner disease (osteochondrosis); pseudodefect of the capitellum (normal posterolateral notch)
- Discriminating feature / next step
- Panner is younger (under 10) and self-limiting; pseudodefect is a constant posterolateral location on a normal surface; OCD shows focal subchondral change — stage with MRI
- Key differentials
- Lateral epicondylitis (common extensor origin); radiocapitellar plica; PIN/radial tunnel syndrome; early OCD
- Discriminating feature / next step
- Ultrasound shows hypoechoic, thickened common extensor origin with neovascularity in epicondylitis; MRI for plica/cartilage; nerve studies for PIN
CRITOEElbow Ossification Centre Sequence
Hook:CRITOE: ages 1-3-5-7-9-11 (odd numbers). The internal (medial) epicondyle is the KEY pitfall — it can be trapped in the joint after dislocation.
Guidelines, Registries & Global Practice
Across all major training systems (FRCS Tr & Orth, FRACS, EBOT/FEBOT, ABOS, DNB/MS, MRCS, SICOT), elbow imaging follows the same evidence-based, stepwise logic: plain radiographs first, CT for fracture detail, and MRI or ultrasound for soft tissue. Differences between societies are largely about access and the threshold for advanced imaging rather than the fundamental algorithm.
- Position
- Radiographs first-line for acute elbow trauma; CT for complex/comminuted intra-articular fractures; MRI for suspected ligament, tendon or occult osseous injury
- Practical implication
- Provides the most explicit modality-by-indication framework; widely referenced internationally
- Position
- Emphasises AP + lateral radiographs as the baseline; advanced imaging reserved for surgical planning or soft-tissue diagnosis
- Practical implication
- Aligns with stepwise escalation; no routine cross-sectional imaging for simple trauma
- Position
- Two orthogonal radiographs; neurovascular documentation; comparison views discouraged as routine but acceptable when ossification assessment is uncertain
- Practical implication
- Stresses clinical assessment and timely senior review over extra imaging
- Position
- Promotes CT (with 3D reconstruction) for articular fracture mapping — coronoid, radial head, distal humerus — to plan fixation vs replacement
- Practical implication
- Underpins terrible-triad and distal humerus planning worldwide
- Position
- Ultrasound endorsed as first-line for epicondylitis and dynamic UCL assessment; MR arthrography for partial UCL tears and OCD stability
- Practical implication
- Ultrasound used more readily where MSK sonography expertise is embedded
Global epidemiology. Radial head/neck fractures are the most common adult elbow fracture (roughly a third of elbow fractures) and the most common occult fracture behind a positive fat pad sign. Supracondylar humerus fractures are the most common paediatric elbow fracture and the leading operatively-treated fracture in children, peaking at ages 5-7 — exactly the cohort where ossification-centre interpretation is hardest. Osteochondritis dissecans of the capitellum and UCL injury cluster in adolescent and adult overhead/throwing athletes.
Registry note. Unlike hip and knee arthroplasty, elbow imaging is not tracked by joint registries; the comparative evidence base is radiology and trauma cohort literature rather than implant-survival data. Where total elbow replacement is performed (e.g. for distal humerus fractures in low-demand elderly patients), national registries such as the NJR (UK), AOANJRR (Australia) and the Norwegian Arthroplasty Register report on implant outcomes, but pre-operative characterisation still rests on CT.
High- vs limited-resource practice variation. In well-resourced settings CT and MRI are obtained promptly for complex fractures and soft-tissue diagnosis. In limited-resource settings the diagnosis frequently rests on radiographs plus disciplined clinical examination and contralateral comparison views; ultrasound — portable, inexpensive and radiation-free — is an especially valuable substitute for MRI in assessing effusion, the UCL and the common extensor/flexor origins. The systematic radiograph (fat pads, anterior humeral line, radiocapitellar line, CRITOE) is therefore the one universal, resource-independent skill every candidate must master.
Controversies & Areas of Uncertainty
Contralateral comparison radiographs can help when ossification-centre interpretation is genuinely uncertain, but routine bilateral imaging doubles radiation and rarely changes management in straightforward cases. Most guidance (including BOAST) discourages reflex comparison views in favour of disciplined CRITOE assessment and selective use only when there is real diagnostic doubt.
A positive posterior fat pad sign after trauma reliably predicts an occult fracture, yet MRI confirmation rarely alters acute management because most occult fractures are stable radial head injuries treated symptomatically. The pragmatic, evidence-aligned approach is to treat as a fracture and reserve CT/MRI for cases where confirmation would change the plan (suspected displacement, mechanical block, athlete needing prognosis).
MRI (or MR arthrography for partial tears) is the reference standard for UCL anatomy, but dynamic stress ultrasound assesses functional valgus laxity in real time and is radiation-free and repeatable. Throwing-arm thickening, hypoechoic foci and increased gapping are normal adaptive findings, so ultrasound must be interpreted against the contralateral side and symptoms — a single study does not predict who will tear the ligament.
For coronoid and radial-head fragments, CT consistently reveals anatomy underestimated by radiographs, and 3D reconstruction improves appreciation of fragment size and pattern. Whether 3D meaningfully changes the operative plan over good 2D multiplanar CT remains debated, but CT in some form is now standard for terrible-triad and complex distal humerus planning.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 7-year-old child falls on an outstretched hand. The lateral elbow radiograph shows a positive posterior fat pad sign but no visible fracture. The AP view appears normal.”
“A 12-year-old child has an elbow dislocation that is reduced in the emergency department. Post-reduction radiographs show the joint is congruent, but you notice that the medial epicondyle is not visible.”
“An examiner asks you to explain the systematic approach to assessing a lateral elbow radiograph in trauma, using alignment lines.”
CRITOE Ossification Centres
- Capitellum (1yr), Radial head (3yr), Internal epicondyle (5yr)
- Trochlea (7yr), Olecranon (9yr), External epicondyle (11yr)
- Ages 1-3-5-7-9-11 (odd numbers)
- KEY: Internal (medial) epicondyle MUST appear BEFORE trochlea
- Missing medial epicondyle after dislocation = trapped in joint (surgical emergency)
Fat Pad Signs
- Posterior fat pad: ALWAYS abnormal when visible = intra-articular effusion
- In trauma: posterior fat pad = occult fracture until proven otherwise
- Most common occult fracture: radial head (adults), supracondylar (children)
- Anterior fat pad (sail sign): less specific — can be normal if small
Alignment Lines (FABLE)
- Anterior humeral line: middle third of capitellum on true lateral
- Radiocapitellar line: must bisect capitellum on ALL views (Monteggia diagnosis)
- Baumann angle: approximately 75 degrees on AP (varus/valgus alignment)
- Carrying angle: 5-15 degrees valgus (cubitus valgus = lateral condyle malunion)
Advanced Imaging Selection
- CT: complex fractures (terrible triad, comminuted radial head) — changes plan in 43%
- MRI: ligaments (UCL sensitivity 92%), OCD staging, bone marrow oedema
- MR arthrography: partial UCL tears, OCD stability, loose body detection
- Ultrasound: dynamic UCL assessment, tendon pathology, guided injection
Evidence Base
Fat Pad Sign and MRI-Confirmed Occult Fracture in Adults
- In 20 adults with a post-trauma elbow effusion (fat pad elevation) but no visible fracture on radiographs, MRI revealed a radiographically occult fracture in 75% (15 of 20).
- Of the occult fractures, 86.6% involved the radial head, with the remainder in the lateral epicondyle (6.7%) and olecranon (6.7%); 90% showed bone marrow oedema on MRI.
- Neither the size of the effusion nor the degree of anterior/posterior fat pad elevation predicted the likelihood of an underlying fracture.
Posterior Fat Pad Sign and Occult Fracture in Children
- In 45 children (mean age 4.5 years) with an elevated posterior fat pad and no other radiographic evidence of fracture, 76% (34 of 45) had a confirmed occult fracture on follow-up radiographs showing new-bone formation.
- The occult fractures were supracondylar in 53%, proximal ulna in 26%, lateral condyle in 12% and radial neck in 9%.
- This far exceeded the previously reported fracture prevalence (6-29%), supporting management as a non-displaced fracture whenever the posterior fat pad is elevated after trauma.
Fat pad signs are the most sensitive radiographic indicator of elbow fracture.