From Weight-Bearing Radiographs to Advanced MRI Assessment
Radiography: First-line for ALL knee presentations. Weight-bearing AP + lateral minimum
Rosenberg view: PA flexion weight-bearing for posterior condylar cartilage assessment
Skyline view: Patellofemoral assessment (tilt, subluxation, OA)
MRI: Gold standard for internal derangement (menisci, ACL, PCL, cartilage)
CT: Fracture characterisation (tibial plateau), malalignment assessment
Ultrasound: Effusion assessment, popliteal cyst (Baker cyst), guided injection
Key: Weight-bearing views are mandatory for OA assessment — non-weight-bearing views are inadequate
- Weight-bearing radiographs are ESSENTIAL for knee OA assessment — non-weight-bearing views OVERESTIMATE joint space width.
- Rosenberg view (PA flexion weight-bearing) detects posterior condylar cartilage loss missed on standard AP views.
- MRI is the gold standard for internal derangement: meniscal tears, ligament injuries, osteochondral lesions, and bone marrow oedema.
- The Segond fracture (avulsion of the anterolateral tibial plateau) is highly associated with ACL tear in adults — treat as an ACL tear until proven otherwise (in children it may occur with an intact ACL).
- Ottawa Knee Rules determine the need for radiography in acute knee injury — not all injured knees require X-ray.
- “A lipohaeamarthrosis (fat-fluid level on horizontal beam lateral) = intra-articular fracture with marrow fat leaking into the joint.
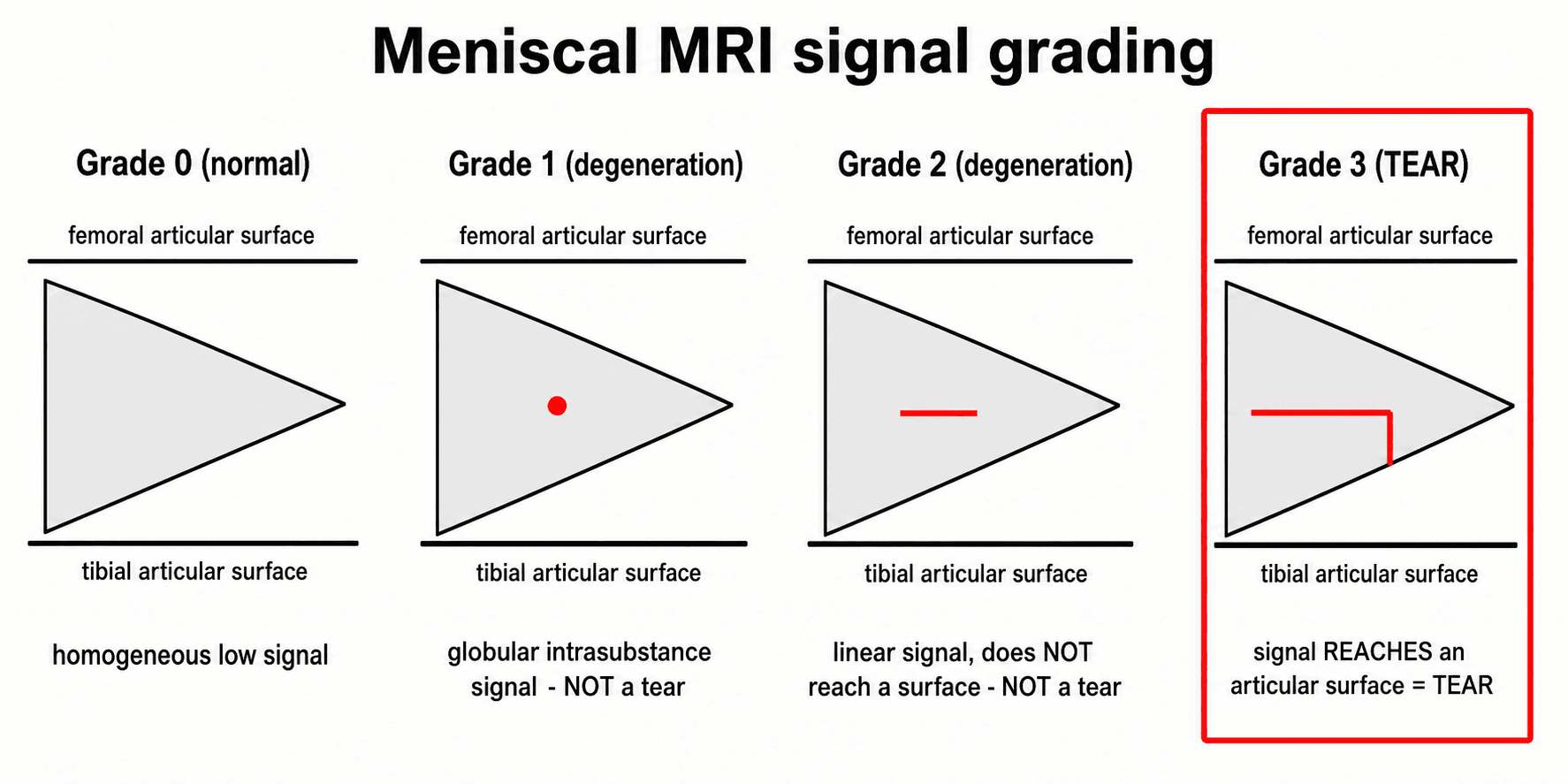
- “Meniscal tear on MRI: high signal on T2 extending to the articular surface (Grade 3). Grade 1-2 intrasubstance signal WITHOUT surface extension is degeneration, NOT tear.
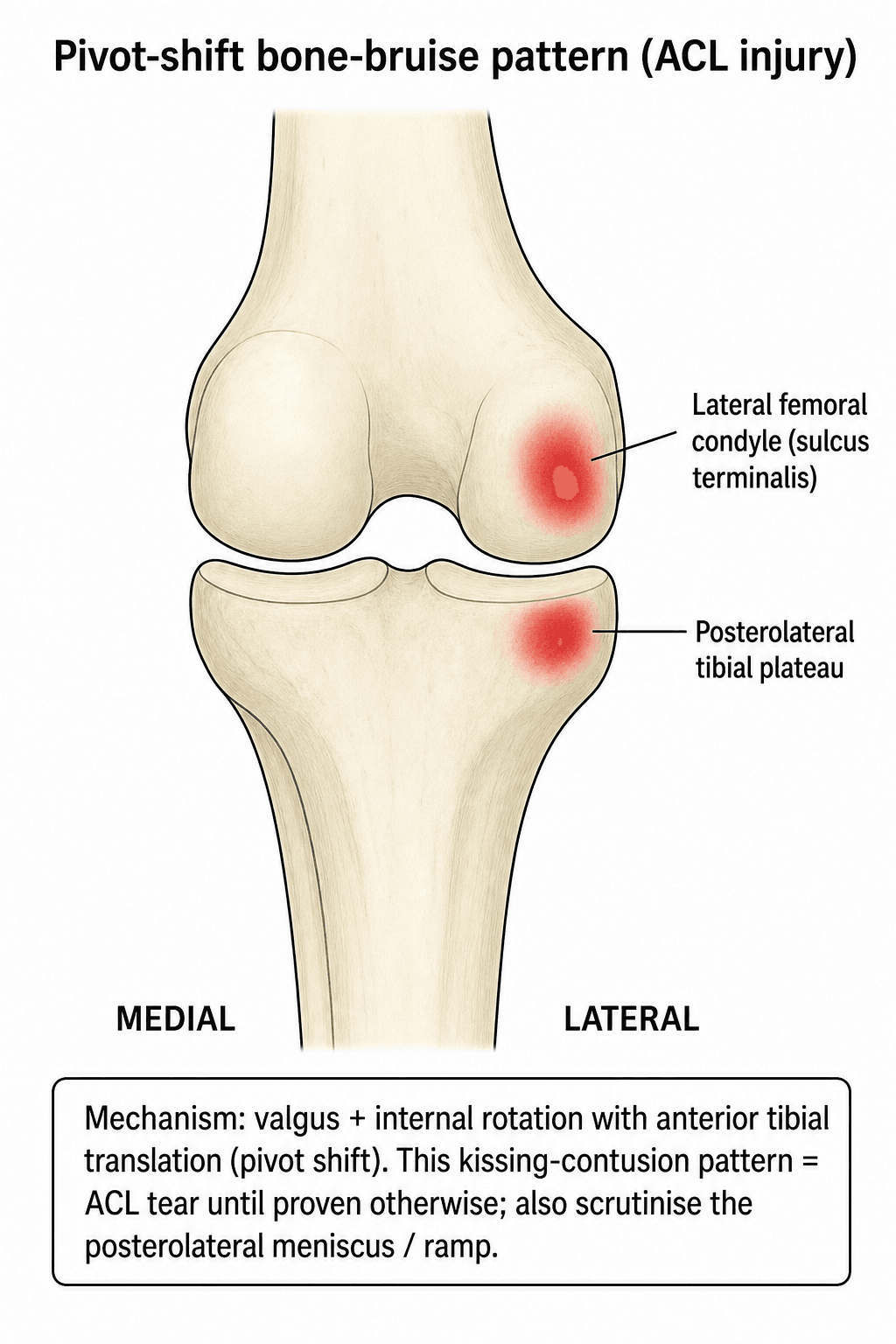
- “ACL tear MRI signs: non-visualisation of the ACL, horizontal/wavy course (loss of normal taut appearance), associated bone bruises (lateral femoral condyle + posterolateral tibial plateau).
- “Pellegrini-Stieda lesion: calcification at the MCL origin (medial femoral condyle) = old MCL avulsion injury.
- “PCL injuries: associated with dashboard mechanism. MRI shows increased signal or disruption of the normally dark, uniform PCL.
Knee imaging is one of the most frequently tested radiology topics. You must know: the importance of WEIGHT-BEARING views for OA assessment, the Rosenberg view, the significance of lipohaeamarthrosis, the Segond fracture (anterolateral tibial avulsion, strongly associated with ACL tear), MRI criteria for meniscal tears (Grade 3 = surface extension), ACL tear signs including bone bruise pattern, and the Ottawa Knee Rules. Classic traps: ordering non-weight-bearing views for OA assessment and calling intrasubstance meniscal signal (Grade 2) a tear.
BLANDACL Tear MRI Signs
Hook:BLAND: the five MRI signs of ACL tear — any one raises suspicion, multiple confirm the diagnosis.
Overview
The knee is the most frequently imaged lower limb joint and one of the most commonly tested imaging assessment topics in fellowship examinations. The key principles of systematic knee imaging are: (1) appropriate view selection (weight-bearing views for OA, Ottawa Rules for trauma), (2) systematic radiograph reading, (3) understanding when advanced imaging (MRI, CT) adds value, and (4) accurate interpretation of MRI findings for internal derangement.
The single most important concept in knee imaging is the requirement for WEIGHT-BEARING views when assessing osteoarthritis. Non-weight-bearing radiographs significantly overestimate the remaining joint space because the cartilage surfaces are not compressed under load. This fundamental error can lead to underestimation of OA severity and inappropriate surgical decision-making.
Radiographs are indicated after acute knee injury ONLY if any of the following are present: (1) Age 55 or older. (2) Tenderness at the fibula head. (3) Isolated tenderness of the patella. (4) Inability to flex the knee to 90 degrees. (5) Inability to weight-bear for 4 steps immediately after injury AND in the emergency department. If NONE of these criteria are met, the probability of a clinically significant fracture is very low (95% CI 0%-0.4% in the validation cohort), and radiographs can be safely deferred. In prospective validation the rule was 100% sensitive for clinically important fractures while cutting radiograph use by about 28%.
The standard AP weight-bearing view may MISS early to moderate OA because: cartilage wear often begins posteriorly on the femoral condyles, and the standard AP view projects through the anterior (thicker) cartilage, obscuring posterior wear. The Rosenberg view (PA projection with knees flexed 45 degrees) shifts the beam to project through the posterior condylar surface — where early cartilage loss occurs. In the original validation it was more accurate, more sensitive and more specific than conventional extension AP views for grade III-IV cartilage loss (correlated against intra-operative findings). This view is essential for assessing OA severity before osteotomy or arthroplasty.
Systematic Approach
Systematic Knee Imaging Assessment
- First-Line Imaging
- Radiographs (if Ottawa Rules positive): AP + lateral
- Advanced Imaging
- MRI for suspected internal derangement (ACL, meniscus). CT for tibial plateau fracture characterisation
- First-Line Imaging
- Weight-bearing AP + lateral + Rosenberg + skyline
- Advanced Imaging
- Full-length alignment (HKA) for osteotomy or arthroplasty planning. MRI only if diagnostic uncertainty
- First-Line Imaging
- AP + lateral radiographs (Segond fracture, effusion, tibial spine avulsion)
- Advanced Imaging
- MRI: gold standard, highly accurate. Assess associated meniscal (including ramp lesions) and collateral injuries
- First-Line Imaging
- Radiographs usually normal (may show degenerative changes)
- Advanced Imaging
- MRI: gold standard. Grade 3 signal (extends to surface) = tear. Root tears are critical to identify
- First-Line Imaging
- Skyline view (tilt, subluxation, OA)
- Advanced Imaging
- MRI for cartilage assessment, MPFL integrity. CT for TT-TG distance measurement (more than 20mm = abnormal)
- First-Line Imaging
- AP + lateral radiographs (lipohaeamarthrosis on lateral)
- Advanced Imaging
- CT with 3D reconstruction: essential for Schatzker classification, fracture morphology, and surgical planning

ABCSSSystematic Knee Radiograph Assessment
Hook:ABCSS: the systematic approach ensuring complete knee radiograph assessment.
Radiographic and MRI Assessment
Essential Radiographic Signs
Lipohaeamarthrosis: A fat-fluid level seen on a HORIZONTAL BEAM lateral radiograph. The fat (less dense) floats on top of the haemarthrosis (blood). This sign indicates an intra-articular fracture with marrow fat leaking into the joint through the fracture site. The most common cause is a tibial plateau fracture, but any intra-articular fracture can produce it. This is a pathognomonic sign and requires CT for full characterisation of the fracture.
Segond fracture: A small avulsion fracture of the anterolateral tibial plateau caused by traction on the anterolateral capsular/ligamentous complex (the anterolateral ligament and capsulo-osseous attachments) during an internal-rotation pivot mechanism. The fragment is a thin vertical sliver of cortical bone off the anterolateral tibial rim, immediately below the articular surface. In adults it is STRONGLY associated with ACL rupture and should be treated as an ACL tear until proven otherwise; it also signals a high rate of concomitant meniscal injury (including ramp lesions). Caution: in skeletally immature patients a Segond-type avulsion can occur with an intact ACL, so MRI is required to define the full injury pattern.
Pellegrini-Stieda lesion: Calcification adjacent to the medial femoral condyle, representing ossification at the origin of the MCL. This indicates a previous (usually chronic) MCL avulsion injury. It may be seen incidentally and is usually asymptomatic, but can occasionally cause medial knee pain.
Tibial spine avulsion: An avulsion fracture of the tibial eminence (ACL footprint). Most common in children and adolescents (8-14 years). Meyers and McKeever classification: Type I (non-displaced), Type II (hinged with anterior elevation), Type III (completely displaced), Type IV (comminuted). Types III and IV require surgical fixation.
Joint space assessment: Kellgren-Lawrence grading on weight-bearing views: Grade 0 (normal), Grade 1 (possible osteophytes), Grade 2 (definite osteophytes, possible JSN), Grade 3 (moderate osteophytes, definite JSN), Grade 4 (large osteophytes, severe JSN, subchondral sclerosis, cyst formation).
Bone Bruise Patterns and the Mechanism
Bone marrow oedema (contusion) on fluid-sensitive MRI is a fingerprint of the injury mechanism: the location of the "kissing" bruises tells you which structure was loaded and which ligament to scrutinise. Recognising the pattern is a recurring exam favourite beyond the single ACL pivot-shift bruise already noted.
- Bruise location
- Lateral femoral condyle (sulcus terminalis) plus posterolateral tibial plateau
- What it points to
- ACL tear - the classic pattern; also raises suspicion of a posterolateral meniscal/ramp injury
- Bruise location
- Anterior proximal tibia
- What it points to
- Posterior force on the flexed knee - PCL injury
- Bruise location
- Lateral femoral condyle and lateral tibial plateau (impaction side), with medial-sided soft-tissue injury
- What it points to
- MCL injury - the bone is bruised laterally while the medial restraint fails
- Bruise location
- Medial patellar facet plus the anterolateral/lateral femoral condyle
- What it points to
- Transient lateral patellar dislocation with MPFL injury - look for an osteochondral fragment
- Bruise location
- 'Kissing' contusions of the anterior femur and anterior tibia
- What it points to
- Hyperextension injury threatening the cruciates (and posterior structures)
The contusion pattern is a clue, not the diagnosis: a pivot-shift bruise should send you to scrutinise the ACL and the posteromedial meniscocapsular junction (ramp lesion); a medial-patellar-facet plus lateral-femoral-condyle bruise should send you to the MPFL and the lateral trochlear/patellar cartilage for an osteochondral fragment. Bone marrow oedema also has non-traumatic mimics (red-marrow reconversion, insufficiency fracture, SIFK), so always correlate the pattern with the clinical mechanism.
Differential Diagnosis & Imaging Pitfalls
Several normal variants and degenerative findings are commonly over-called as significant pathology. Distinguishing a true tear from a mimic is a recurring exam theme.
- True pathology (when to call it)
- Grade 3: linear high signal reaching an articular surface = tear
- Mimic / pitfall (do NOT over-call)
- Grade 1-2 intrasubstance signal (no surface contact) = degeneration, not a tear
- True pathology (when to call it)
- True radial or flap tear with surface extension
- Mimic / pitfall (do NOT over-call)
- Transverse (intermeniscal) ligament insertion and popliteus hiatus mimic anterior horn / posterolateral tears
- True pathology (when to call it)
- Genuine narrowing on a weight-bearing or Rosenberg view
- Mimic / pitfall (do NOT over-call)
- Apparent preservation on a non-weight-bearing film (overestimates joint space)
- True pathology (when to call it)
- Non-visualisation, horizontal course, plus pivot-shift bone bruise
- Mimic / pitfall (do NOT over-call)
- Mucoid degeneration / ganglion of the ACL (celery-stalk appearance, ligament intact)
- True pathology (when to call it)
- Pivot-shift bruise pattern, insufficiency/stress fracture, SIFK
- Mimic / pitfall (do NOT over-call)
- Normal red-marrow reconversion or post-exercise oedema in athletes
- True pathology (when to call it)
- True lateral meniscal or chondral lesion
- Mimic / pitfall (do NOT over-call)
- Iliotibial band friction signal and a discoid lateral meniscus (a variant, not a tear unless it tears)
The single most common reportable error in knee MRI is calling Grade 1-2 intrasubstance meniscal signal a "tear." Only signal that unequivocally reaches an articular surface (Grade 3) is a tear. Over-calling degeneration drives inappropriate arthroscopy, particularly in middle-aged and older patients where degenerate meniscal tears respond no better to surgery than to structured exercise.
Ultrasound of the Knee
The topic lists ultrasound as a knee modality but never sets out its uses. Ultrasound is cheap, dynamic and radiation-free but operator-dependent, and it is especially valuable where MRI is scarce - so its specific roles (and blind spots) are examinable.
- What it shows
- Fluid and synovial thickening in the suprapatellar pouch
- Note
- Sensitive for small effusions; guides aspiration
- What it shows
- Fluid in the gastrocnemio-semimembranosus bursa with its characteristic neck; can show rupture tracking down the calf
- Note
- A common cause of posterior knee swelling and a DVT mimic when ruptured
- What it shows
- Quadriceps and patellar tendon (tendinopathy, tears), MCL, iliotibial band
- Note
- Excellent for superficial structures; dynamic stress assessment is possible
- What it shows
- Real-time needle guidance for aspiration and injection
- Note
- Improves accuracy of joint and soft-tissue injections
- What it shows
- Limited - the cruciates, menisci and articular cartilage are largely inaccessible
- Note
- Ultrasound does NOT replace MRI for internal derangement
Ultrasound is the right first tool for an effusion, a suspected Baker cyst, a superficial tendon problem or a guided injection, and it carries more diagnostic weight where MRI is scarce. But it cannot reliably assess the cruciate ligaments, the menisci or the articular cartilage, so it does not replace MRI for suspected internal derangement - a haemarthrosis with a positive Lachman still needs an MRI, not just an ultrasound.
WARSWeight-Bearing Knee Views
Hook:WARS: Weight-bearing, Alignment, Rosenberg, Skyline — the four key views for comprehensive knee assessment.
Guidelines, Registries & Global Practice
Knee imaging follows a broadly consistent evidence-based algorithm worldwide: plain radiographs first (weight-bearing for any osteoarthritis question), a validated decision rule to ration radiographs after acute trauma, MRI for internal derangement, and CT for fracture morphology. The differences between societies are mostly of emphasis and access rather than of principle.
Global epidemiology. Symptomatic knee OA affects an increasing share of the adult population worldwide and is a leading cause of disability in the Global Burden of Disease estimates, driven by ageing and rising obesity. ACL injuries occur most commonly in young athletes (pivoting/contact sports), and meniscal tears span a bimodal pattern — traumatic tears in the young and degenerate tears in middle age and older. Tibial plateau fractures cluster bimodally too (high-energy injury in the young, low-energy fragility fractures in older adults).
- Acute knee trauma
- Radiographs first; apply a decision rule; MRI for suspected ligament/meniscal injury once fracture excluded
- OA assessment
- Weight-bearing radiographs are the appropriate first test; MRI not routinely indicated
- Suspected internal derangement
- MRI is the preferred advanced test
- Acute knee trauma
- Selective radiography (Ottawa-type rule); avoid routine knee MRI in primary care
- OA assessment
- Weight-bearing radiographs; clinical diagnosis of OA may not need imaging at all
- Suspected internal derangement
- MRI where the result will change management, usually via secondary care
- Acute knee trauma
- Radiographs then CT for articular fractures (tibial plateau) to plan fixation
- OA assessment
- Not the focus; alignment views for deformity planning
- Suspected internal derangement
- MRI to characterise associated ligament/meniscal injury
- Acute knee trauma
- Decision-rule-guided radiography; early MRI in young athletes with a haemarthrosis
- OA assessment
- Weight-bearing plus skyline and alignment views before surgery
- Suspected internal derangement
- MRI gold standard; actively look for ramp and root tears
Registry and audit context. There is no dedicated imaging registry, but national arthroplasty registries (NJR for England/Wales, AJRR in the US, AOANJRR in Australia, the Swedish and Norwegian registries, NZJR) rely on standardised weight-bearing and full-length alignment radiographs for pre-operative planning and outcome audit, reinforcing weight-bearing imaging as the global standard for OA workup.
High- versus limited-resource practice variation. Where MRI is scarce or expensive, ultrasound (effusion, Baker cyst, dynamic patellar tracking, guided injection) and careful clinical examination carry more diagnostic weight, and diagnostic arthroscopy may still be used selectively. In well-resourced settings, pre-operative MRI before arthroscopy is routine and purely diagnostic arthroscopy has largely been abandoned. Decision rules such as the Ottawa Knee Rule are especially valuable in high-volume or resource-limited emergency settings to ration radiography safely.
Controversies & Areas of Uncertainty
In middle-aged and older patients with knee pain, MRI frequently shows a degenerate meniscal tear — but such tears are also highly prevalent in asymptomatic knees. Multiple trials show arthroscopic partial meniscectomy offers little benefit over exercise therapy for degenerate tears without mechanical locking. The controversy is how much weight to give an MRI tear when the same finding is so common in pain-free knees.
Early MRI can drive over-treatment by surfacing incidental degeneration, marrow oedema, or chondral changes of uncertain significance. Decision rules (Ottawa) and a weight-bearing-first radiograph strategy exist precisely to limit low-value imaging — yet practice variation in MRI access and referral thresholds remains wide between health systems.
The structure avulsed in a Segond fracture has been debated (lateral capsule, anterolateral ligament, or capsulo-osseous iliotibial band). The clinical message is stable: in adults it signals ACL-complex injury and a high rate of meniscal ramp lesions, but in children it can occur with an intact ACL — so MRI, not the radiograph alone, defines management.
Higher field strength (3T) improves signal-to-noise and small-structure depiction (cartilage, small meniscal and ligament tears), but 1.5T remains diagnostically adequate for most internal derangement. The incremental value of 3T over a well-performed 1.5T study for routine reporting is real but modest, and access varies globally.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 65-year-old woman is being assessed for knee osteoarthritis. She brings non-weight-bearing AP and lateral knee radiographs that show mild changes. Her clinical symptoms suggest more severe disease.”
“A 25-year-old footballer presents with acute knee injury after a twisting mechanism. The lateral radiograph shows a fat-fluid level in the suprapatellar pouch.”
“An examiner shows you a knee MRI and asks you to systematically describe your assessment of the menisci and cruciate ligaments.”
Weight-Bearing Views (WARS)
- Weight-bearing AP: mandatory for OA assessment (non-WB overestimates JSW)
- Alignment (HKA): full-length for mechanical axis, surgical planning
- Rosenberg: PA flexion 45 degrees — detects posterior condylar wear missed on AP
- Skyline: patellofemoral assessment (tilt, subluxation, PFJOA)
Key Radiographic Signs
- Lipohaemarthrosis: fat-fluid level on horizontal beam lateral = intra-articular fracture
- Segond fracture: anterolateral tibial avulsion = strongly associated with ACL tear (treat as ACL tear; check for ramp lesion)
- Pellegrini-Stieda: medial epicondylar calcification = old MCL injury
- Tibial spine avulsion: ACL footprint avulsion (children), Meyers-McKeever classification
Meniscal MRI Assessment
- Grade 3 (signal to articular surface) = TEAR. Grade 1-2 = degeneration (NOT tear)
- Absent bow-tie sign: suggests bucket-handle (displaced) tear
- Double PCL sign: displaced bucket-handle fragment lies by PCL
- Root tear: absent root on coronal MRI + extrusion more than 3mm = functional meniscectomy
ACL Tear MRI Signs (BLAND)
- Bone bruise: lateral femoral condyle + posterolateral tibial plateau (pivot shift)
- Lax/horizontal ACL course (loss of normal taut appearance)
- Anterior tibial translation more than 7mm (sagittal images)
- Non-visualisation of ligament (most specific sign)
- Deep lateral femoral notch sign (more than 1.5mm)
Evidence Base
MRI vs Arthroscopy for Internal Derangement of the Knee
- Systematic review (arthroscopy as the reference standard) found MRI highly accurate for meniscal and ACL tears, and the most appropriate screening tool before therapeutic arthroscopy.
- Diagnostic performance differed by structure, with accuracy of approximately 85% across medial meniscus, lateral meniscus and ACL.
- MRI is preferable to diagnostic arthroscopy in most patients because it avoids the surgical risks of an operative procedure.
Ottawa Knee Rule — Prospective Validation
- In 1096 adults with acute knee injury, the rule was 100% sensitive (95% CI 0.94-1.0) for the 63 clinically important fractures.
- If the rule was negative, the estimated probability of fracture was 0% (95% CI 0%-0.4%).
- Applying the rule could reduce radiograph use by an estimated 28%, and physicians interpreted it correctly in 96% of cases.
MRI and clinical rules provide evidence-based imaging pathways.