From AP Pelvis to MRI Hip Assessment
- AP pelvis radiograph is the standard first-line investigation for all hip and pelvic presentations.
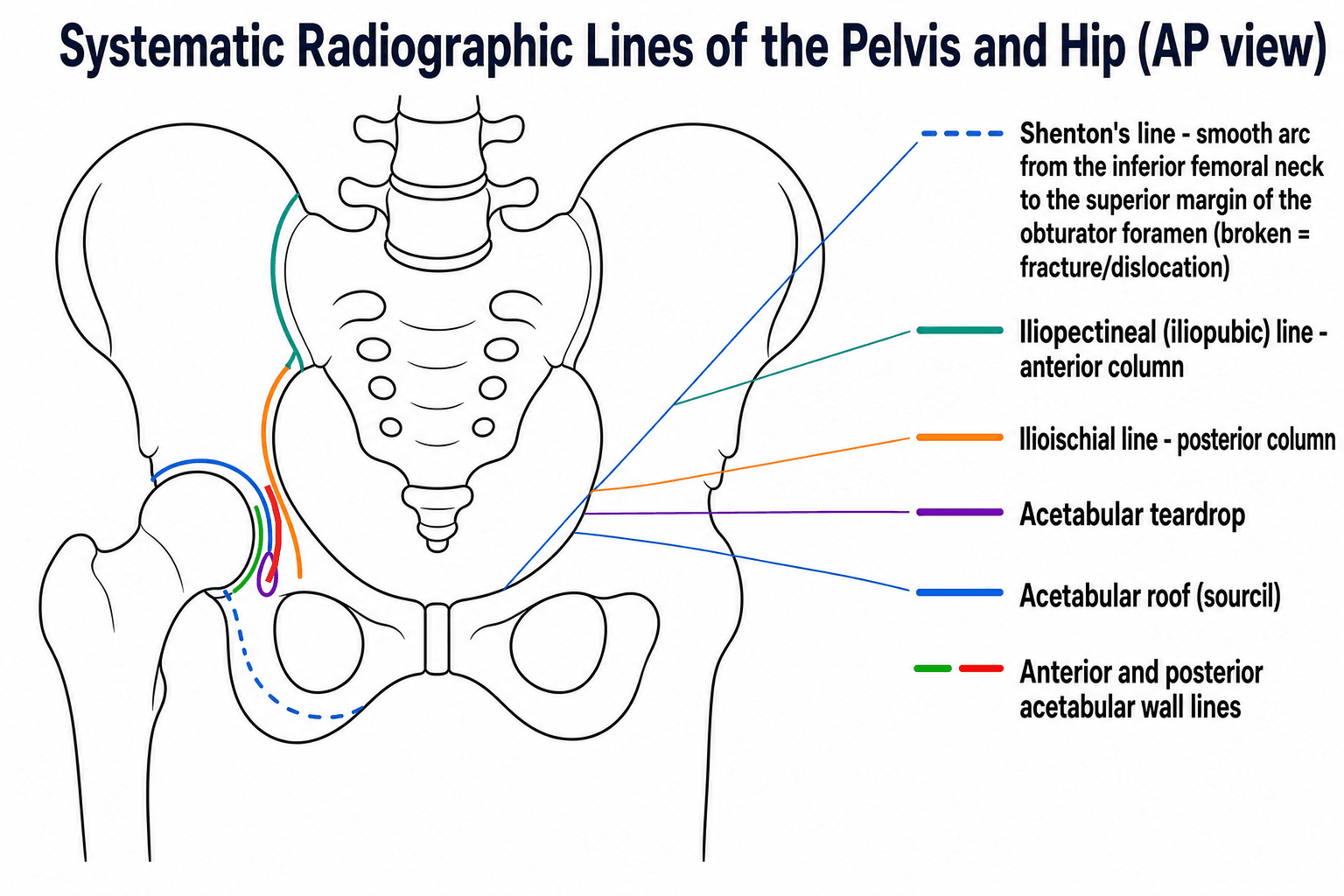
- Shenton line: a smooth arc along the inferior border of the superior pubic ramus and medial femoral neck — disruption indicates fracture or dislocation.
- MRI within 24 hours is the gold standard for occult NOF fracture when radiographs are normal and clinical suspicion persists.
- AVN staging uses Ficat-Arlet or Steinberg classification — MRI detects AVN at Stage I (preclinical), before radiographic changes.
- Femoroacetabular impingement: alpha angle (cam) and lateral centre-edge angle (pincer) are key measured parameters.
- “In elderly patients with hip pain after a fall, if the AP pelvis is normal, 2-5% have an occult NOF fracture — MRI MUST be performed within 24 hours.
- “The Garden classification for NOF fractures: I (incomplete/valgus impacted), II (complete non-displaced), III (complete partially displaced), IV (complete fully displaced). III-IV have highest AVN risk.
- “Acetabular fractures: Judet views (45 degree obliques) assess the anterior and posterior columns and walls. CT with 3D reconstruction is essential for Letournel-Judet classification.
- “Paediatric hip imaging: USS is the primary modality before 6 months (Barlow/Ortolani), AP pelvis radiograph after 6 months (Perkins and Hilgenreiner lines for DDH).
- “Perthes disease: MRI shows extent of epiphyseal involvement (Catterall, Herring lateral pillar classification) better than radiographs.
Pelvis and hip imaging is tested extensively in both written and viva formats. You must know: systematic AP pelvis reading, Shenton line, Garden classification for NOF fractures, the occult NOF fracture pathway (MRI within 24 hours), AVN staging on MRI, acetabular fracture assessment (Judet views, Letournel-Judet classification), paediatric hip imaging (DDH lines, Perthes staging), and FAI imaging (alpha angle, LCEA). Classic traps: discharging an elderly patient with hip pain and normal radiographs without arranging urgent MRI.
Overview
Systematic pelvis and hip imaging encompasses a broad spectrum of pathology from acute trauma (NOF fracture, acetabular fracture, pelvic ring disruption) to chronic conditions (OA, AVN, FAI, DDH). The AP pelvis radiograph is the essential first-line investigation, with advanced imaging selected based on the clinical question.
The most important clinical scenario is the elderly patient with hip pain after a fall and normal radiographs — this requires urgent MRI to exclude an occult NOF fracture. Delayed diagnosis is one of the most common causes of medicolegal claims in orthopaedic practice.
On the AP pelvis: (1) Check adequacy — both hips visible, symmetric obturator foramina (no rotation), coccyx aligned with symphysis. (2) Shenton line bilaterally — disruption indicates fracture or dislocation. (3) Hip joint spaces — bilateral comparison, normal more than 4mm (medial JSW). (4) Pelvic ring integrity — trace the entire ring, looking for disruption at pubic rami, SI joints, and acetabulum. Remember: the pelvic ring must break in TWO places. (5) Femoral neck — cortical integrity, trabecular pattern. Garden I fractures may show only a valgus impaction line. (6) Lesser trochanter profile — if visible in straight AP, suggests external rotation from displaced NOF fracture.
MRI is critical in: (1) Occult NOF fracture (radiographs normal, clinical suspicion) — MRI within 24 hours has 99-100% sensitivity. (2) AVN staging — MRI detects stage I (pre-radiographic) AVN with the 'double line sign' (band pattern of low signal on T1 with high signal on T2). (3) Labral tears — MR arthrography (sensitivity 87%) for FAI workup. (4) Transient osteoporosis — diffuse bone marrow oedema without AVN changes. (5) Bone marrow pathology — metastases, myeloma infiltration, stress fractures. (6) Perthes disease staging — extent of epiphyseal involvement.
Pelvic Ring and Sacral Fracture Classification
Having traced the ring on the AP pelvis (plus inlet/outlet views and CT), classify the injury — the classification predicts instability, haemorrhage and neurological risk.
Pelvic ring: Young-Burgess (mechanistic) and Tile (stability)
Young-Burgess groups injuries by force vector:
- APC (anteroposterior compression / "open book") I-III — symphyseal diastasis ± progressive anterior then posterior SI disruption. Highest transfusion requirement and mortality (the Whitbeck data below).
- LC (lateral compression) I-III — sacral impaction ± internal rotation of the hemipelvis (the "windswept" pelvis at LC-III).
- VS (vertical shear) — vertical displacement of the hemipelvis (fall from height); vertically unstable.
- CM (combined mechanism) — features of more than one pattern.
Tile classifies by stability: A = stable (ring intact / minimally displaced), B = rotationally unstable but vertically stable (open-book or lateral-compression), C = rotationally AND vertically unstable (complete posterior disruption).
Sacral fractures: Denis zones
- Location
- Ala (lateral to the foramina)
- Neurological risk
- Lowest (~6%); L5 root if any
- Location
- Transforaminal
- Neurological risk
- Intermediate (~28%); L5/S1/S2 roots
- Location
- Central (canal, medial to foramina)
- Neurological risk
- Highest (~57%); bowel/bladder/sexual (cauda equina)
A transverse sacral fracture with bilateral vertical components (a U- or H-shaped fracture) produces spinopelvic dissociation — the upper sacrum/spine separates from the pelvis — and carries a high rate of neurological deficit.
PAINOccult NOF Fracture Pathway
Hook:PAIN: an elderly patient in PAIN after a fall with normal X-rays STILL NEEDS MRI — do NOT discharge without it.
Garden I-IVGarden Classification for NOF Fractures
Hook:Garden Types: I=impacted (lowest risk), II=non-displaced, III=partially displaced, IV=fully displaced (highest AVN risk). Non-displaced (I-II): fix. Displaced (III-IV): replace (in elderly).
Systematic Approach
Systematic Pelvis and Hip Imaging Assessment
- First-Line Imaging
- AP pelvis + lateral hip radiograph
- Advanced Imaging
- MRI within 24 hours if normal radiographs and clinical suspicion persists (occult NOF fracture). CT if MRI unavailable
- First-Line Imaging
- AP pelvis + Judet views (45 degree obliques)
- Advanced Imaging
- CT with 3D reconstruction for Letournel-Judet classification and surgical planning. MRI for associated labral/cartilage injury
- First-Line Imaging
- AP pelvis + inlet/outlet views
- Advanced Imaging
- CT for complete ring assessment (posterior ring is often underestimated on radiographs). Angiography if haemodynamically unstable
- First-Line Imaging
- AP pelvis + frog lateral hip
- Advanced Imaging
- MRI: gold standard for early AVN detection (pre-radiographic). Ficat-Arlet or Steinberg classification
- First-Line Imaging
- AP pelvis + Dunn view (45 degree flexion lateral)
- Advanced Imaging
- MR arthrography for labral assessment. CT for alpha angle measurement, head-neck offset ratio
- First-Line Imaging
- USS (less than 6 months) or AP pelvis (more than 6 months)
- Advanced Imaging
- MRI if USS equivocal. Arthrography (fluoroscopic) for concentric reduction assessment during surgery
SHIPSystematic AP Pelvis Assessment
Hook:SHIP: Sail through the AP pelvis systematically — Shenton, Hip joint, Iliac wings, Proximal femur.
Differential Diagnosis — The Painful Hip with Normal or Subtle Radiographs
When the AP pelvis is normal or near-normal but the patient has significant hip pain, the differential is the highest-yield part of this topic. Distinguishing these entities is almost entirely an MRI exercise, because the discriminating features are in the bone marrow and soft tissue.
- Typical patient
- Elderly, fall, cannot weight-bear
- Key MRI features
- Low-signal fracture line on T1 with surrounding marrow oedema (high T2/STIR), usually subcapital/transcervical
- Discriminator
- A discrete linear T1 hypointensity crossing the neck — not just diffuse oedema
- Typical patient
- 30-50 years; steroids, alcohol, sickle cell; often bilateral
- Key MRI features
- Serpiginous band (double-line sign on T2) demarcating the anterosuperior necrotic segment, preserved fatty marrow within
- Discriminator
- Geographic lesion with a reactive interface, not crossing as a single fracture line
- Typical patient
- Middle-aged men; third-trimester women
- Key MRI features
- Diffuse marrow oedema of head and neck, no demarcating band, no subchondral fracture
- Discriminator
- Self-limiting; oedema is homogeneous and lacks the AVN reactive interface
- Typical patient
- Older osteoporotic patient, acute pain
- Key MRI features
- Subchondral low-signal line with surrounding oedema, often superolateral head
- Discriminator
- Fracture line parallels the subchondral plate (mimics but is not AVN)
- Typical patient
- Young active adult, groin pain, positive impingement test
- Key MRI features
- Best on MR arthrography: contrast tracking into a torn anterosuperior labrum; cam/pincer morphology
- Discriminator
- Mechanical, activity-related; marrow usually normal
- Typical patient
- Febrile adult or unwell child
- Key MRI features
- Joint effusion, synovial enhancement, peri-articular oedema
- Discriminator
- Aspirate if effusion plus systemic signs — do not delay for imaging
Clinical Applications
Neck of Femur Fracture Imaging
Radiographic detection: The AP pelvis radiograph detects approximately 95-98% of NOF fractures. Key signs: (1) cortical discontinuity at the femoral neck, (2) disruption of Shenton line, (3) trabecular pattern disruption (medial calcar compression), (4) valgus angulation (Garden I — impacted), (5) shortening and external rotation of the affected limb (displaced fracture — lesser trochanter becomes prominent).
Garden classification on radiographs: Garden I (incomplete/impacted): subtle valgus impaction line, trabeculae still visible. Often the most difficult to detect. Garden II (complete non-displaced): fracture line visible across the entire neck, fragments in anatomical position. Garden III (partially displaced): femoral head rotated but still in contact with the neck. Garden IV (fully displaced): complete separation, femoral head may be in acetabulum while neck/shaft retract.
Occult NOF fracture: In 2-5% of patients, the initial radiograph is NORMAL despite a genuine fracture. These patients present with hip pain, inability to weight-bear, and pain on internal rotation. Clinical suspicion MUST lead to MRI within 24 hours. MRI has 99-100% sensitivity for occult NOF fracture. On MRI: a fracture line appears as a low-signal line on T1 surrounded by bone marrow oedema (high signal on T2/STIR). The fracture configuration (subcapital, transcervical, basicervical) and displacement determine management.
CT as alternative: When MRI is unavailable, CT has approximately 80% sensitivity for undisplaced NOF fractures. CT is inferior to MRI for this indication but is a reasonable alternative in emergency settings.
Guidelines, Registries & Global Practice
Pelvis and hip imaging pathways are broadly concordant worldwide, but the named guidelines, resource availability and registry context differ. The AP pelvis radiograph is the universal first-line study; the principal global divergence is in how quickly and how often advanced imaging (MRI/CT) is added.
Global epidemiology
Hip fracture is the dominant high-volume indication. There are an estimated 1.5 million-plus hip fractures per year worldwide, projected to rise sharply with population ageing, with the largest absolute increase expected in Asia. Around 5-10% of fractures that ultimately require surgery are not seen on the initial radiograph, and meta-analysis data show that among elderly patients imaged for clinical suspicion with negative/equivocal films the occult-fracture rate is far higher (about 39%). Non-traumatic AVN of the femoral head presents most often in the 30-50 age group and is bilateral in roughly half to four-fifths of non-traumatic cases. Developmental dysplasia of the hip (DDH) affects roughly 1-3 per 1000 live births for frank dislocation, with higher rates of sonographic dysplasia.
Side-by-side guideline comparison
- Occult NOF fracture
- MRI is the first-line investigation when hip fracture is suspected but not seen on radiographs; if MRI is not feasible within 24 hours or is contraindicated, use CT
- Other emphasis
- Hip fracture imaging tied to time-to-surgery care standards
- Occult NOF fracture
- MRI usually appropriate for radiographically occult hip fracture; CT is the main alternative where MRI is unavailable
- Other emphasis
- Detailed modality-by-indication appropriateness ratings
- Occult NOF fracture
- Cross-sectional imaging (CT) central to acetabular and pelvic ring fracture classification and operative planning
- Other emphasis
- Letournel-Judet (acetabulum) and Tile/Young-Burgess (ring) frameworks
- Occult NOF fracture
- Supports MRI-first occult-fracture pathways and early AVN detection; endorses MR arthrography for labral/FAI workup
- Other emphasis
- Aligns with Warwick Agreement principles for FAI assessment
Registry and outcome context
National hip fracture registries and audits (e.g. the UK National Hip Fracture Database, and equivalents in Australia/New Zealand, the Nordic countries and elsewhere) tie prompt, accurate imaging diagnosis to time-to-surgery targets, because delayed diagnosis of an occult fracture delays surgery and worsens outcome. Arthroplasty registries (NJR, AJRR, AOANJRR, SHAR/Swedish, Norwegian, NZJR) capture downstream implant survival for the hemiarthroplasty and total hip replacements that displaced NOF fractures and end-stage AVN ultimately require.
High- versus limited-resource practice variation
In well-resourced systems 24-hour MRI for occult fracture, MR arthrography for labral pathology, and CT with 3D reconstruction for acetabular/ring planning are routine. Where MRI access is constrained, CT (sensitivity around 79% for occult fracture) is the accepted substitute, repeat/delayed radiographs and bone scanning are used, and ultrasonography has an expanding bedside role — for DDH screening, for hip effusion, and as a high-accuracy adjunct for occult femoral neck fracture where MRI is unavailable. DDH screening strategy itself varies globally between universal sonographic screening (common in parts of continental Europe) and selective screening of at-risk infants (breech, family history, clinical instability), with radiography reserved for after the femoral head ossifies (around 4-6 months).
Controversies & Areas of Uncertainty
The classic teaching figure of "2-5% of NOF fractures are occult" describes the proportion of all hip fractures missed on first films. In the subgroup actually selected for advanced imaging because of clinical suspicion and negative/equivocal radiographs, meta-analysis data put the occult-fracture rate much higher (around 39%). The "MRI within 24 hours" standard is driven by avoiding surgical delay rather than by a loss of MRI sensitivity over time, and is a service-delivery target that not all systems can meet.
MRI is the reference standard, but modern CT detects most surgically relevant occult fractures (high negative predictive value for femoral neck/intertrochanteric fractures), while missing a minority — including some undisplaced fractures. Ultrasonography of anterior joint capsule swelling shows promising accuracy for occult femoral neck fracture in dedicated series. The unresolved question is how to triage limited MRI capacity without missing the fractures CT under-calls.
An alpha angle above 55-60 degrees defines cam morphology, but cam morphology is common in asymptomatic athletes and not all cam hips become symptomatic or develop osteoarthritis. Imaging numbers must be interpreted alongside symptoms and examination (the Warwick Agreement frames FAI as a clinical-imaging-symptom triad), and there is no single universally agreed threshold.
Universal sonographic screening detects more dysplasia but increases treatment of hips that would have resolved spontaneously, whereas selective (risk-factor) screening misses some cases. The optimal balance between overtreatment and missed late-presenting DDH remains debated and is reflected in differing national programmes.


Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“An 82-year-old woman presents to the emergency department with hip pain after a fall. She cannot weight-bear. The AP pelvis radiograph appears normal.”
“A 35-year-old man on long-term corticosteroids presents with bilateral hip pain. His AP pelvis radiograph shows sclerosis in the right femoral head. MRI of both hips is requested.”
“An examiner shows you an AP pelvis radiograph and asks you to describe your systematic assessment.”
“A 26-year-old footballer has 6 months of activity-related right groin pain and a positive anterior impingement test (FADIR). The AP pelvis looks broadly normal to the junior doctor.”
Systematic AP Pelvis (SHIP)
- Shenton line: smooth arc along inferior pubic ramus and medial femoral neck
- Hip joints: JSW more than 4mm, sphericity, osteophytes, subchondral changes
- Iliac wings and pelvic ring: ring must break in TWO places — always find the second
- Proximal femur: cortical integrity, trabecular pattern, trochanter avulsions
Occult NOF Fracture (PAIN)
- 2-5% of NOF fractures have normal initial radiographs
- MRI within 24 hours: gold standard (sensitivity 99-100%)
- CT second-line (sensitivity approximately 80%) if MRI unavailable
- Garden I-II (non-displaced): fix. Garden III-IV (displaced): replace (elderly)
AVN Assessment
- MRI gold standard: detects Stage I (pre-radiographic) AVN
- Double line sign (T2): band of low signal + inner high signal = pathognomonic
- Crescent sign: subchondral fracture (Stage III) — indicates imminent collapse
- Bilateral in 50-80% of non-traumatic cases — always image BOTH hips
FAI Imaging
- Alpha angle more than 55-60 degrees = cam morphology
- LCEA more than 40 degrees = pincer overcoverage
- Crossover sign on AP pelvis = focal retroversion
- MR arthrography: sensitivity 87% for labral tears (vs 66% non-contrast MRI)
Evidence Base
Advanced Imaging for Radiographically Occult Hip Fracture
- Across 35 studies (2992 patients, mean age 76.8 years), 39% of patients with acute hip pain and negative or equivocal radiographs had a radiographically occult hip fracture on MRI.
- When initial radiographs showed only an isolated greater trochanter fracture, 92% had an occult intertrochanteric or femoral neck extension on MRI.
- Using MRI as the reference standard, CT sensitivity was 79% and bone scanning 87% — both inferior to MRI for detecting occult fracture.
Garden Classification of Subcapital Fractures
- Original four-grade radiographic classification of subcapital femoral neck fractures based on the trabecular pattern and degree of displacement on the AP view.
- Grade I (incomplete/valgus impacted) and II (complete, undisplaced) are non-displaced; grade III (complete, partial displacement) and IV (complete, full displacement) are displaced.
- Displacement (grades III-IV) reflects greater retinacular vessel disruption and underpins the higher rates of avascular necrosis and non-union reported in later series.
Pelvic Ring Mechanism Predicts Resuscitation and Mortality
- In complete anterior and posterior ring disruptions, the Young-Burgess mechanism classification predicted clinical course: anteroposterior compression (APC) versus vertical shear (VS).
- APC injuries far more often required 10 or more units of blood in 24 hours (15/18) than VS injuries; multisystem organ failure was commoner (11/18 vs 2/14).
- Mortality was markedly higher in the APC group (39% vs 0% for VS), confirming that mechanism on imaging, not just fracture location, drives resuscitation needs.
NOF fracture imaging and pelvic ring assessment have direct, time-critical management implications.