Imaging in Pregnancy: Safety and Decision-Making
In trauma, suspected cauda equina syndrome, septic arthritis, unstable fracture, or suspected visceral injury, the correct principle is to image decisively. A missed maternal diagnosis is usually a bigger threat to mother and fetus than the radiation from a justified diagnostic study.
SAFESAFE Imaging Hierarchy
Hook:SAFE means choose the lowest-risk adequate test, not no test.
DOSEDOSE Counselling
Hook:DOSE is how you counsel rather than frighten the patient.
Overview
Pregnancy imaging decisions are built around two facts. First, ultrasound and MRI avoid ionising radiation and therefore become preferred whenever they can answer the clinical question. Second, most diagnostic radiographs and many justified CT studies still deliver fetal doses well below the level associated with deterministic effects such as malformation or neurodevelopmental injury.
That means the real task is not to avoid imaging at all cost. The real task is to match modality to question, optimise dose when ionising radiation is used, and counsel patients honestly. Orthopaedic practice most often encounters this in trauma, suspected pelvic or spinal injury, infection, and severe back pain with neurological compromise.
Systematic Approach
- Question
- Is the question time-critical or limb/life threatening?
- Preferred action
- Image without delay
- Question
- Will ultrasound or MRI answer it?
- Preferred action
- Use them first when equivalent
- Question
- If radiographs or CT are needed, what body region and protocol are involved?
- Preferred action
- Optimise collimation and avoid extra phases
- Question
- Is contrast essential to answer the question?
- Preferred action
- Avoid gadolinium unless the extra information is necessary
- Question
- Does the patient understand the rationale and expected risk?
- Preferred action
- Explain benefits, dose context, and alternatives
Fetal Radiation and Contrast
- Typical fetal exposure pattern
- Negligible to extremely low
- Exam takeaway
- Usually safe when indicated
- Typical fetal exposure pattern
- Low
- Exam takeaway
- Often far below deterministic thresholds
- Typical fetal exposure pattern
- Usually low fetal scatter
- Exam takeaway
- May still be justified in trauma
- Typical fetal exposure pattern
- Higher than radiographs but often still below deterministic thresholds
- Exam takeaway
- Optimise protocol and justify clearly
Examiners reward realistic figures and the practical points the prose only implies:
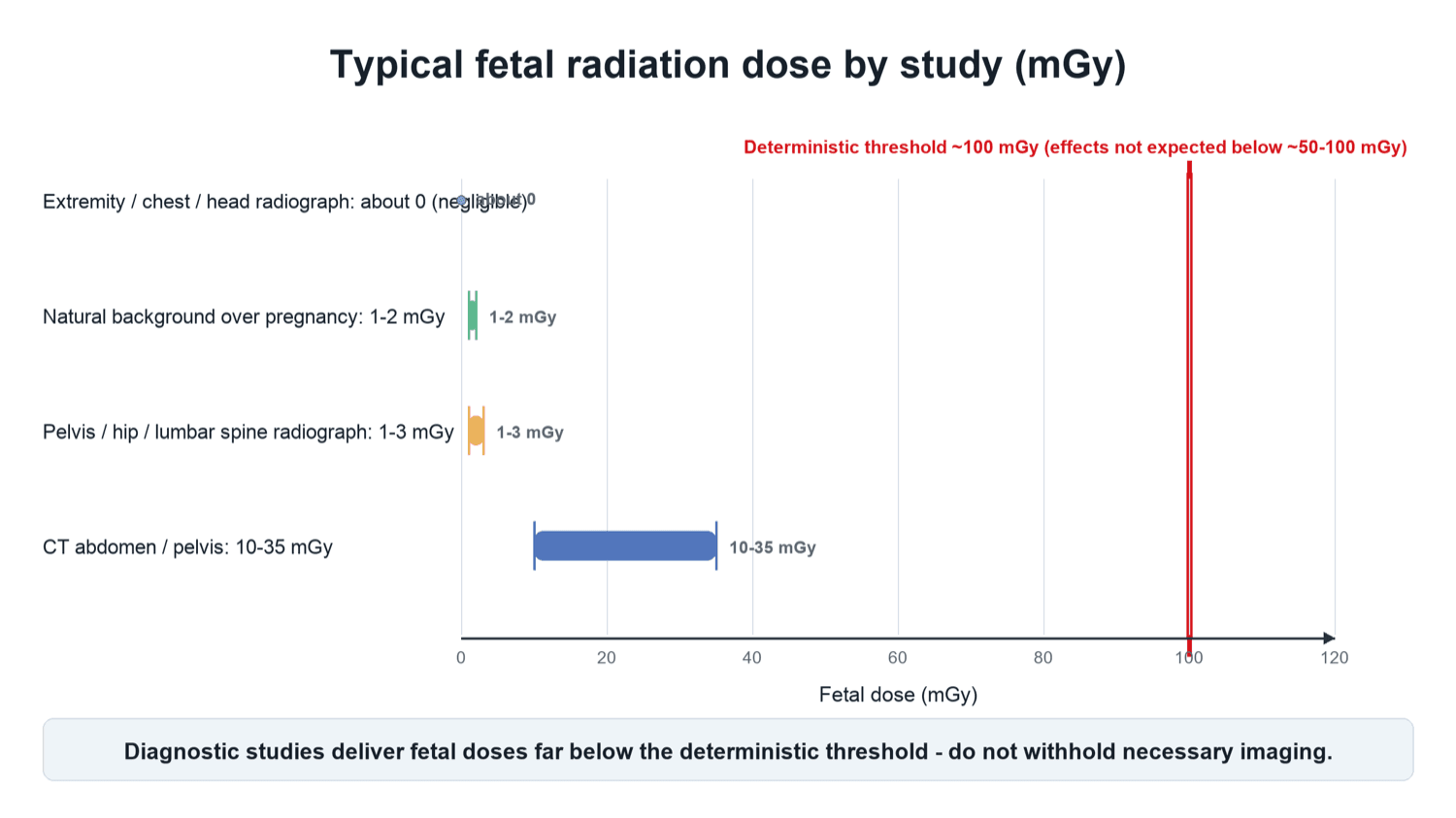
- Approximate fetal doses to quote (for perspective, natural background over the whole pregnancy is roughly 1–2 mGy): extremity, chest, head and cervical-spine radiographs and CT of the head/chest deliver a fetal dose that is essentially negligible (well under a fraction of a mGy of scatter); pelvis, hip, abdomen and lumbar-spine radiographs are low — of the order of 1–3 mGy; CT of the abdomen/pelvis is the highest common study, roughly of the order of 10–35 mGy, yet still usually below the ~50–100 mGy threshold.
- Dose reduction is about protocol, not refusal: justify the study, collimate to the region of interest, use a single phase (avoid multiphase acquisitions), apply low-dose / iterative-reconstruction CT protocols, and avoid repeats.
- The shielding update: routine external lead "fetal/gonadal" shielding is no longer recommended by many bodies (e.g. AAPM) — it can obscure anatomy, trigger the automatic-exposure-control to increase dose, and does little against internal scatter. Optimising the protocol, not a lead apron over the abdomen, is what lowers fetal dose.
- Breastfeeding does NOT need to be interrupted after contrast — for both iodinated and gadolinium agents, the amount excreted into breast milk and then absorbed by the infant gut is negligible (ACR/ESUR). Telling a mother to "pump and dump" after contrast is a common, outdated myth.
Gestational Windows and Deterministic Risk
The reason gestational age matters is that the fetus passes through phases of differing radiosensitivity. Counselling and protocol decisions should reflect this, while remembering that diagnostic doses rarely reach the relevant thresholds.
- Dominant concern
- All-or-nothing effect (loss vs unaffected survival)
- Practical implication
- Malformation risk not increased; pregnancy may not yet be recognised
- Dominant concern
- Congenital malformation if dose is high
- Practical implication
- Most radiosensitive for structural anomaly, but threshold is around 100 to 200 mGy
- Dominant concern
- Highest risk of reduced IQ / severe intellectual disability
- Practical implication
- Most sensitive window for the developing CNS
- Dominant concern
- Lower CNS sensitivity
- Practical implication
- Effects only at substantially higher doses
- Dominant concern
- Small stochastic increase in childhood cancer
- Practical implication
- Relative risk small; absolute baseline childhood cancer risk is low
"Counsel honestly" only works if you anchor it to the baseline risks the patient already carries:
- Frame against background risk. In the general population the risk of a major congenital anomaly is about 3 per cent (roughly 1 in 33) and the baseline childhood-cancer risk is about 0.1–0.3 per cent. A single diagnostic study adds a negligible increment on top of these — a fetal dose around 1 mGy adds a childhood-cancer risk on the order of 1 in 10,000 or less, dwarfed by the baseline.
- The no-termination principle (ICRP). Fetal doses below about 100 mGy are NOT an indication to terminate a pregnancy and are not a reason to withhold a justified examination; deterministic effects are not expected below roughly 50–100 mGy. Even the highest common diagnostic exposures do not reach the level at which termination would be discussed.
- Do not overstate the linear-no-threshold model. Presenting stochastic risk without the (tiny) absolute numbers can frighten a patient into refusing necessary imaging or seeking inappropriate termination — give both the very low absolute risk and the benefit of an accurate diagnosis.
- Practical consent: document the indication and discussion; for the highly anxious patient, or one who has had multiple or high-dose studies, ask a medical physicist for an estimated fetal dose. If a study was already done before the pregnancy was known, reassure with the actual estimated dose — the vast majority are far below any threshold.
Differential of the Pregnant Patient with Bone or Back Pain
Not every musculoskeletal complaint in pregnancy is mechanical. Several pregnancy-associated conditions can mimic trauma or degenerative disease, and recognising them changes both imaging choice and management.
- Distinguishing features
- Atraumatic hip or back pain, often third trimester or postpartum
- Preferred imaging
- Non-contrast MRI (marrow oedema); avoids radiation
- Distinguishing features
- Low back / pelvic pain, often peripartum, normal radiographs
- Preferred imaging
- MRI most sensitive; radiograph often negative early
- Distinguishing features
- Mechanical pain over symphysis or sacroiliac joints
- Preferred imaging
- Clinical; radiograph or MRI only if severe or refractory
- Distinguishing features
- Fever, raised inflammatory markers, joint effusion
- Preferred imaging
- Ultrasound-guided aspiration; MRI without gadolinium
- Distinguishing features
- Saddle anaesthesia, bladder dysfunction, bilateral leg symptoms
- Preferred imaging
- Urgent MRI lumbar spine without gadolinium
- Distinguishing features
- Groin pain, antalgic gait, risk factors (steroids)
- Preferred imaging
- Non-contrast MRI
Back and pelvic pain are common in normal pregnancy, but red-flag features (neurological deficit, fever, atraumatic fracture, night pain) demand the same decisive imaging you would offer a non-pregnant patient. The default is non-contrast MRI, which carries no ionising-radiation risk.
Guidelines, Registries & Global Practice
Global Epidemiology
Trauma complicates roughly 6 to 8 percent of pregnancies and is a leading non-obstetric cause of maternal death, which is precisely why decisive maternal imaging is emphasised worldwide. Musculoskeletal complaints are near-universal in pregnancy: pelvic girdle pain and low back pain affect a large proportion of pregnancies, the majority mechanical and self-limiting, but a minority masking insufficiency fracture, transient osteoporosis, infection or neural compression.
Side-by-Side Guidance
- Core position
- Ultrasound and MRI are imaging of choice; do not withhold indicated radiography/CT; single diagnostic studies rarely reach deterministic thresholds
- Core position
- Ionising studies appropriate when justified; emphasise protocol optimisation and realistic, region-specific dose communication
- Core position
- Clinically justified imaging proceeds; non-contrast MRI preferred cross-sectional study; gadolinium avoided unless essential
- Core position
- Fetal doses under about 100 mGy are not a reason to terminate or withhold a justified examination
- Core position
- In major trauma, maternal stabilisation and decisive imaging take priority; fetal monitoring runs in parallel
High- vs Limited-Resource Practice
In well-resourced settings, urgent MRI and dose-optimised multidetector CT are usually available around the clock, so the safest adequate test is rarely out of reach. In limited-resource settings, MRI may be unavailable or delayed; here the justified use of radiographs and CT becomes more important, and ultrasound (including FAST in trauma) carries even greater weight as a radiation-free, bedside, low-cost first-line tool. The underlying principle is universal: match the modality to the question, optimise dose, and never withhold imaging that will change maternal management.
Controversies and Areas of Uncertainty
Clinical Imaging
The hierarchy of imaging in pregnancy follows directly from the radiation principle: lead with modalities that carry no ionising radiation, and reserve radiography or CT for when they will change management.


Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 12-week pregnant patient presents with severe back pain and possible cauda equina syndrome.”
“A 20-week pregnant patient falls and may have a pelvic fracture.”
“A major trauma patient at 8 weeks gestation may have intra-abdominal injury.”
Preferred Order
- Ultrasound first when adequate
- MRI without gadolinium for most cross-sectional questions
- Radiographs when clinically indicated
- CT when it best answers an urgent question
Counselling Principles
- Use realistic dose language
- Explain that most diagnostic studies are far below deterministic thresholds
- State that maternal diagnosis protects fetal outcome
- Document indication and discussion
Contrast Rules
- Avoid gadolinium unless essential
- Use iodinated contrast if the CT question requires it
- Do not sacrifice diagnosis simply to avoid contrast
- Follow local neonatal thyroid-check policy if relevant
Viva Bottom Line
- Do not withhold necessary imaging
- Optimise protocol rather than avoid diagnosis
- MRI is preferred, not mandatory
- Emergency imaging proceeds when management depends on it
Evidence Base
Every citation below has been checked against its source record in PubMed (the ACOG and ACR entries are society guidance without a PMID). The recurring theme is consistent across guidelines, the large Ray cohort, and the dosimetry/trauma reviews: necessary imaging proceeds, ultrasound and non-contrast MRI lead, single diagnostic studies sit far below deterministic thresholds, and gadolinium is the one agent to avoid unless essential.
ACOG Guidance on Diagnostic Imaging During Pregnancy and Lactation
- Ultrasound and MRI are the imaging techniques of choice when they answer the clinical question.
- Withholding needed radiography or CT because of pregnancy is discouraged when the result will change management.
- Counselling should emphasise that necessary diagnostic imaging rarely approaches deterministic-risk thresholds.
ACR Practice Guidance for Imaging Potentially Pregnant Patients
- Ionising studies remain appropriate when clinically justified and when the result will materially affect care.
- Protocol design and dose reduction are more important than avoiding every study regardless of diagnostic need.
- Risk communication should use realistic region-specific exposure rather than generic statements that overstate harm.
Association Between MRI Exposure During Pregnancy and Fetal and Childhood Outcomes
- Among 1,424,105 deliveries in Ontario, first-trimester MRI (n=1737) was NOT associated with increased stillbirth/neonatal death, congenital anomaly, neoplasm, or vision/hearing loss versus no MRI.
- Gadolinium MRI at any time in pregnancy (n=397) was associated with a higher risk of a broad set of rheumatological, inflammatory or infiltrative skin conditions (adjusted HR 1.36, 95% CI 1.09 to 1.69).
- Gadolinium exposure was also associated with increased stillbirth or neonatal death (adjusted RR 3.70, 95% CI 1.55 to 8.85).
Fetal Dosimetry at CT: A Primer
- No single diagnostic CT examination commonly used in pregnancy approaches the deterministic-effect dose thresholds for the fetus.
- Fetal dose cannot be measured directly in vivo and is estimated by medical physicists using validated methods; radiologists should understand the magnitude of these doses.
- Knowing dose thresholds for biologic effects allows confident, evidence-based counselling rather than reflexive avoidance.