Safe Scanning Around Metal
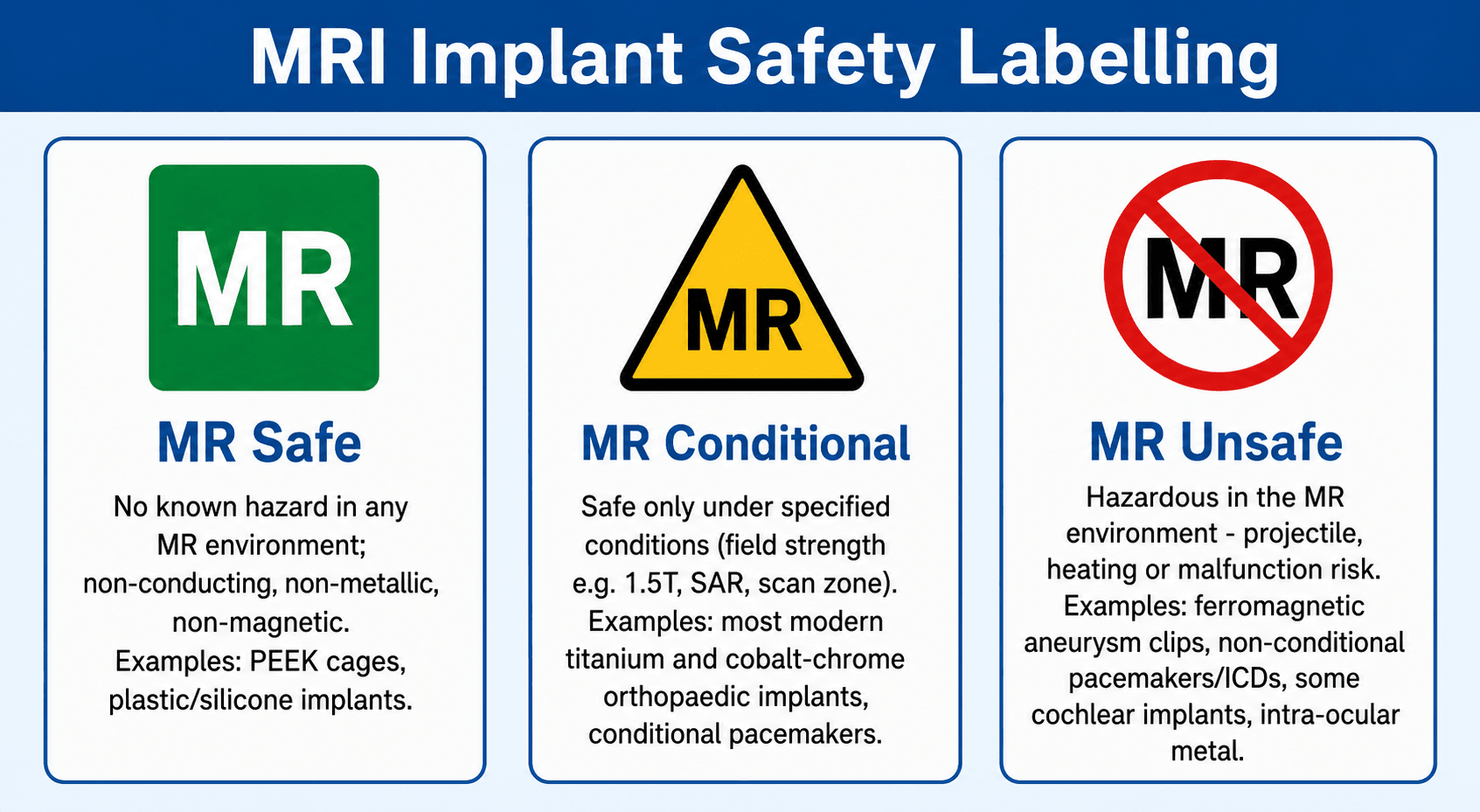
MR Safe: Non-conducting, non-metallic, non-magnetic — safe in ALL MR environments
MR Conditional: Safe under SPECIFIC conditions (field strength, SAR limits, scan duration, gradient specifications)
MR Unsafe: Known hazard in ALL MR environments — MUST NOT enter the MR scanner room
Key: The term 'MRI compatible' is NO LONGER used — it has been replaced by the three-tier classification system
- The three MRI safety categories: MR Safe (no hazard in any MR environment), MR Conditional (safe under specific conditions), MR Unsafe (hazardous in MR).
- Hazards of metal in MRI: missile/projectile effect (translational force), torque (rotational force), RF-induced heating, and image artefact.
- Most modern orthopaedic implants (titanium, cobalt-chrome, tantalum) are MR Conditional at 1.5T — safe to scan under specified conditions.
- Absolute contraindications: non-MR-conditional cardiac pacemakers/defibrillators, ferromagnetic intracranial aneurysm clips, metallic foreign bodies (especially intraocular).
- 1.5T produces less metal artefact than 3T. Spin echo sequences are preferred over gradient echo near metal.
- “Titanium alloy produces the LEAST susceptibility artefact and ferromagnetic force — ideal for MRI-compatible implants.
- “Stainless steel (316L) produces SIGNIFICANT artefact but most modern implants are non-ferromagnetic and MR Conditional at 1.5T.
- “Cobalt-chrome (CoCr) produces moderate artefact — between titanium and stainless steel.
- “The 'missile effect' occurs when ferromagnetic objects experience strong translational force toward the magnet bore — potentially lethal.
- “Implant heating risk depends on: implant geometry (loops concentrate current), field strength, SAR, and scan duration.
MRI safety with orthopaedic implants is a high-yield topic tested in both physics viva stations and clinical scenarios. You must know: the three ASTM safety categories, the mechanisms of harm (missile effect, torque, heating, artefact), which implant materials are safest, the difference between 1.5T and 3T for imaging around metal, and artefact reduction strategies (MAVRIC-SL, SEMAC, spin echo, STIR). A common viva scenario presents a patient with a joint replacement requiring MRI of the spine — you must demonstrate safe decision-making.
MATHMRI Hazards of Metal
Hook:MATH: Missile, Artefact, Torque, Heating — the four hazards of metal in MRI.
SWIMSArtefact Reduction Strategies
Hook:SWIMS through the artefact: Spin echo, Wider bandwidth, Inversion recovery, MAVRIC, Smaller voxels/lower field.
Overview
MRI safety in patients with implants is one of the most clinically important topics in musculoskeletal radiology. As MRI use continues to increase and the population of patients with orthopaedic implants grows, orthopaedic surgeons are frequently asked whether their patients can safely undergo MRI scanning. Understanding the principles of implant-MRI interactions is essential for safe clinical practice.
The key concept is that the interaction between metal and the magnetic field depends on the ferromagnetic properties of the implant material, not simply whether it is metal. Ferromagnetic materials (iron, nickel, cobalt in certain alloys) experience strong forces in the magnetic field. Non-ferromagnetic metals (titanium, tantalum, most modern orthopaedic alloys) experience minimal forces and are generally safe.
Modern MRI safety classification uses three standardised categories defined by ASTM International: (1) MR Safe — poses no hazards in any MR environment (e.g., plastic, ceramic). (2) MR Conditional — safe under specified conditions documented by the manufacturer (field strength, spatial gradient, SAR limits, body part scanned). Most modern orthopaedic implants are MR Conditional at 1.5T. (3) MR Unsafe — poses hazards in all MR environments and must not enter the scanner room. The obsolete term 'MRI compatible' should no longer be used.
When a patient with an orthopaedic implant needs MRI: (1) Identify the exact implant (manufacturer, model, material). (2) Check the manufacturer's MRI safety documentation for the specific device. (3) If MR Conditional, ensure all specified conditions (field strength, SAR, gradients) are met. (4) If the implant cannot be identified, assume MR Unsafe unless the clinical need is urgent and the risk-benefit ratio favours scanning. (5) Document the safety assessment in the medical record.
Gadolinium Contrast Agents: Safety and Contraindications
Beyond implants and devices, the other major MRI "contraindication" the surgeon must know concerns gadolinium-based contrast agents (GBCAs).
- Nephrogenic Systemic Fibrosis (NSF): a rare but serious scleroderma-like fibrosing disorder of skin, joints and viscera linked to GBCAs in patients with severe renal impairment (eGFR < 30 mL/min/1.73m², dialysis, or acute kidney injury). Screen renal function (eGFR) before giving contrast to at-risk patients.
- Agent classes (ACR): older Group I (linear) agents carry the highest NSF risk and are largely withdrawn or restricted; Group II (macrocyclic) agents have a very low / negligible NSF risk and are now preferred — NSF is now very rare with appropriate agent selection and renal screening.
- Gadolinium retention/deposition: trace gadolinium can deposit in brain (dentate nucleus, globus pallidus) and bone, more with linear agents; clinical significance is uncertain, but it favours using the lowest effective dose of a Group II agent.
- Acute hypersensitivity reactions: uncommon but possible (urticaria to anaphylaxis); ask about prior contrast reaction.
- Pregnancy: gadolinium crosses the placenta — avoid in pregnancy unless essential; non-contrast MRI itself is generally considered safe in pregnancy when indicated.
In a patient with renal impairment who needs contrast (e.g. suspected periprosthetic infection or tumour), check the eGFR, prefer a Group II macrocyclic agent at the lowest effective dose, and weigh whether a non-contrast protocol can answer the question.
PACEDMRI Contraindications
Hook:PACED: check for these five categories before EVERY MRI scan. Missing one could be fatal.
Systematic Approach
Systematic MRI Safety Assessment for Patients with Implants
- Action
- Complete a standardised MRI safety questionnaire for EVERY patient
- Key Considerations
- Questions must cover: cardiac devices, surgical implants, foreign bodies, cochlear implants, metallic fragments, occupational exposure
- Action
- Identify the exact implant: manufacturer, model, material
- Key Considerations
- Surgical records, implant cards, hospital databases, or contact the operating surgeon. Radiographs can help identify implant type
- Action
- Consult manufacturer MRI safety documentation or MRIsafety.com
- Key Considerations
- Categorise as MR Safe, MR Conditional, or MR Unsafe. Note specific conditions for MR Conditional devices
- Action
- Assess whether the clinical benefit of MRI outweighs any residual risk
- Key Considerations
- If implant cannot be identified, consider alternative imaging (CT, ultrasound). Urgency of clinical need vs risk
- Action
- Select appropriate MRI protocol to minimise risks and artefact
- Key Considerations
- 1.5T preferred. Spin echo sequences. Wider bandwidth. STIR over chemical fat sat. Consider MAVRIC-SL/SEMAC
- Action
- Record the safety assessment, implant details, and conditions met
- Key Considerations
- Document in the medical record for medicolegal protection and future reference
The MRI Environment: Safety Zones (ACR)
Screening is enforced physically through the ACR four-zone access-control model. Knowing the zones is a standard viva point — the magnet is always on, so access is controlled by location, not by switching the field off.
- Area
- Freely accessible public area outside the MR environment (e.g. corridors, general reception)
- Access
- Open to everyone; no screening
- Area
- Interface between the public Zone I and the controlled Zone III — where patients are greeted, screened and history taken
- Access
- Patients under supervision of MR personnel; screening begins here
- Area
- Strictly restricted region (including the scanner control room) where free access by unscreened people/objects can cause serious injury
- Access
- Physically controlled (locked/badge access); only screened patients and MR personnel
- Area
- The MR scanner (magnet) room itself — the most restricted zone; the magnetic field is always present
- Access
- Entry only by screened individuals under direct MR-personnel supervision; clearly marked, magnet-on signage
Implant Materials and MRI
- Ferromagnetism
- Non-ferromagnetic
- Artefact Severity
- Minimal — smallest artefact of all metals
- MRI Safety
- MR Conditional at 1.5T and 3T (most implants)
- Common Uses
- Spinal instrumentation, fracture plates, screws, total joint stems
- Ferromagnetism
- Very weakly ferromagnetic
- Artefact Severity
- Moderate — larger artefact than titanium
- MRI Safety
- MR Conditional at 1.5T (most modern implants)
- Common Uses
- Femoral heads, tibial trays, bearing surfaces
- Ferromagnetism
- Weakly/non-ferromagnetic
- Artefact Severity
- Significant — largest artefact of common orthopaedic metals
- MRI Safety
- MR Conditional at 1.5T (most modern 316L implants)
- Common Uses
- Fracture plates, intramedullary nails, cerclage wires, K-wires
- Ferromagnetism
- Non-ferromagnetic
- Artefact Severity
- Minimal to moderate
- MRI Safety
- MR Conditional at 1.5T
- Common Uses
- Acetabular augments, spinal fusion cages, tumour implants
- Ferromagnetism
- Weakly ferromagnetic (temperature-dependent)
- Artefact Severity
- Minimal to moderate
- MRI Safety
- Usually MR Conditional at 1.5T
- Common Uses
- Staples, fracture fixation devices, shape memory implants
- Ferromagnetism
- Non-magnetic (polymer)
- Artefact Severity
- None — MR transparent
- MRI Safety
- MR Safe
- Common Uses
- Spinal fusion cages, suture anchors, interference screws
Titanium alloy (Ti-6Al-4V) is the preferred material for MRI-compatible implants because it is: (1) Non-ferromagnetic — no missile or torque risk. (2) Produces minimal susceptibility artefact — allows diagnostic imaging near the implant. (3) MR Conditional at both 1.5T and many 3T scanners. (4) Biocompatible with excellent osseointegration. The main limitation is that titanium cannot be used for bearing surfaces (it has poor wear characteristics for articulation).
When MRI Is Contraindicated: Imaging Alternatives
When MRI is genuinely contraindicated (e.g., a non-MR-conditional cardiac device that cannot be reprogrammed, an unidentifiable implant, or a confirmed intraocular ferromagnetic foreign body that cannot be removed in time), the clinical question still has to be answered. The choice of alternative depends on whether the target pathology is bony, soft tissue, vascular, or infective.
- Best For
- Bone detail, osteolysis, component position, loosening, fracture
- Key Strength
- Excellent osseous and implant geometry; fast; widely available
- Key Limitation
- Ionising radiation; inferior soft-tissue contrast; residual streak artefact near dense metal
- Best For
- Periprosthetic fluid, abscess, tendon integrity, guided aspiration
- Key Strength
- No artefact from metal; dynamic; allows real-time aspiration/biopsy
- Key Limitation
- Operator-dependent; limited depth and field of view; cannot assess bone or deep central structures
- Best For
- Component position, loosening, periprosthetic fracture, lysis screening
- Key Strength
- Cheap, reproducible, baseline for change over time
- Key Limitation
- Low sensitivity for early soft-tissue and marrow pathology
- Best For
- Suspected periprosthetic infection or loosening when MRI/CT equivocal
- Key Strength
- Functional/metabolic information; whole-body survey
- Key Limitation
- Limited spatial resolution; lower specificity; radiation; time-consuming
- Best For
- Vascular assessment when MR angiography is unavailable
- Key Strength
- Rapid vascular mapping without magnetic field exposure
- Key Limitation
- Iodinated contrast load; radiation; calcium/metal can obscure lumen
There is no single replacement for MRI. For a suspected periprosthetic infection in a pacemaker-dependent patient, ultrasound-guided aspiration plus CT and inflammatory markers usually answers the question. For acute neurology with an intraocular foreign body, non-contrast CT and CT angiography cover most emergencies. State explicitly in a viva that you would choose the alternative based on the specific diagnostic question, not default to a single substitute.


Guidelines, Registries & Global Practice
MRI safety is governed worldwide by a consistent framework — standardised ASTM International terminology (MR Safe / MR Conditional / MR Unsafe), the four-zone access-control model, and mandatory pre-scan screening — but the implementing society and the local infrastructure vary by region. Demand is rising globally as both MRI utilisation and the prevalence of orthopaedic implants increase with ageing populations.
Side-by-Side Guidance
- Core Position
- ACR Manual on MR Safety: four safety zones, designated MR Medical Director and MR Safety Officer, screening of all persons/objects
- Practical Emphasis
- Strong governance and personnel roles; widely adopted reference for zone control
- Core Position
- MHRA guidance on safe use of MRI equipment plus RCR clinical standards; emphasises documented local safety policy
- Practical Emphasis
- Regulatory device-safety focus and clear local accountability
- Core Position
- Defines MR Safe / Conditional / Unsafe terminology and the icons used on device labelling and in the bore environment
- Practical Emphasis
- The shared vocabulary all other guidance is built on
- Core Position
- Manufacturer Instructions for Use specify the exact MR Conditional parameters (field strength, spatial gradient, SAR, scan time)
- Practical Emphasis
- The legally and clinically binding source for any individual implant
- Core Position
- Protocols permitting scanning of selected non-MR-conditional cardiac devices at 1.5T with EP supervision
- Practical Emphasis
- Shifts some legacy devices from absolute contraindication to conditional, protocol-driven
Registries and Implant Identification
When the operative note or implant card is missing, national arthroplasty registries can help identify the device and therefore its alloy and MR labelling. Large registries include the National Joint Registry (NJR, UK), the American Joint Replacement Registry (AJRR, US), the Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR), and the Swedish and Norwegian registries. Manufacturer databases and curated resources such as MRIsafety.com complement these for non-arthroplasty hardware.
High- vs Limited-Resource Practice Variation
In well-resourced centres, 1.5T and 3T scanners, dedicated metal-artefact-reduction sequences (MAVRIC, SEMAC, WARP, MARS), ferromagnetic detection systems, and formal MR safety officer roles are routine. In limited-resource settings, access to MRI itself may be restricted, advanced metal-suppression sequences may be unavailable, and implant identification can be difficult where surgical records or registries are incomplete. Where MRI capacity is constrained, CT (with metal-artefact-reduction reconstruction), ultrasound, and radiographs carry more of the diagnostic load, and rigorous screening discipline becomes even more important because rescue resources are limited.
The Surgeon's Responsibilities (Universal)
Regardless of region, the operating surgeon should: accurately document the implant manufacturer, model, and material in the operative record; provide the patient with an implant identification card; and communicate implant details to radiology whenever MRI is being considered.
Controversies & Areas of Uncertainty
The traditional teaching that MRI should be delayed for 6 weeks after implantation to allow tissue ingrowth to resist torque is largely historical. It applied to a concern about ferromagnetic implant migration. For modern non-ferromagnetic titanium and cobalt-chrome implants, translational force and torque are minimal, and there is little evidence that early scanning displaces a well-fixed implant. Most authorities now permit earlier scanning of MR Conditional non-ferromagnetic implants when clinically indicated, while still exercising caution with any genuinely ferromagnetic device.
A major shift over the past decade is the recognition that many 'legacy' (non-MR-conditional) pacemakers and defibrillators can be scanned at 1.5T under a strict institutional protocol with electrophysiology supervision, device interrogation, and reprogramming. This is now reflected in some cardiology society guidance. However, it remains an off-label, protocol-driven decision — not a green light — and the safest exam answer is still to treat a non-MR-conditional device as a contraindication unless a formal pathway with cardiology is in place.
The rule of thumb that susceptibility artefact roughly scales with field strength favours 1.5T for large implants. But 3T offers higher signal-to-noise, and with modern multispectral sequences and high bandwidth, diagnostic imaging around smaller implants (screws, anchors, fine wires) at 3T is often acceptable. The field-strength choice should be individualised to implant size, alloy, and the clinical question rather than applied as an absolute.
Some tattoo and permanent-makeup pigments contain iron oxide and can cause local heating or a tingling sensation, occasionally a superficial burn. This is usually a minor, self-limiting issue rather than a contraindication. Patients should be counselled, monitored, and given a means to alert staff; large or recently applied tattoos near the region of interest warrant extra caution.
Specific Clinical Scenarios
Total Hip and Knee Replacement
Safety: Virtually all modern total hip and knee replacement components are MR Conditional at 1.5T. This includes components made of:
- Titanium femoral stems and tibial baseplates
- Cobalt-chrome femoral components and femoral heads
- Stainless steel components (older designs)
- Polyethylene (UHMWPE) liners — MR transparent
Wait period: Traditionally, a 6-week wait after implantation was recommended to allow soft tissue ingrowth to stabilise the implant before MRI (to prevent torque displacement). However, for most modern non-ferromagnetic implants, this is no longer considered necessary if the clinical need is urgent.
Artefact management: Joint replacement components produce significant artefact, particularly cobalt-chrome and stainless steel components. For peri-prosthetic assessment (infection, adverse reaction to metal debris, component loosening), specialised protocols are essential:
- 1.5T (less artefact than 3T)
- Spin echo sequences (Fast Spin Echo preferred)
- STIR for fluid and oedema detection (not chemical fat suppression)
- MAVRIC-SL or SEMAC if available
- Wider receiver bandwidth
These optimised protocols can provide diagnostic imaging of periprosthetic soft tissues despite the presence of large metallic components.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 70-year-old patient with a total hip replacement develops new-onset thigh pain 5 years post-operatively. You want to request an MRI of the hip. The patient also has a cardiac pacemaker.”
“An examiner asks you to explain why titanium produces less MRI artefact than stainless steel, and what strategies you would use to minimise artefact around a stainless steel implant.”
“A patient presents to the emergency department with a metallic foreign body in the orbit suspected from an industrial accident two days ago. They now need an urgent brain MRI for unrelated acute neurological symptoms.”
Safety Categories (ASTM)
- MR Safe: no hazard in any MR environment (plastic, ceramic, PEEK)
- MR Conditional: safe under specific conditions (most modern ortho implants at 1.5T)
- MR Unsafe: hazardous in all environments (old pacemakers, ferromagnetic clips)
- Term 'MRI compatible' is OBSOLETE — do not use
Absolute Contraindications (PACED)
- Pacemakers/ICDs (non-MR-conditional)
- Aneurysm clips (ferromagnetic intracranial)
- Cochlear implants (non-MR-conditional)
- Eye metallic foreign bodies (orbital radiograph screening)
- Electronic devices (neurostimulators, insulin pumps)
Metal Hazards (MATH)
- Missile (projectile) effect — translational force on ferromagnetic objects
- Artefact — signal void and geometric distortion
- Torque — rotational force aligning object with B0
- Heating — RF-induced current in conductive loops
Implant Materials
- Titanium: least artefact, non-ferromagnetic, gold standard for MRI-safe implants
- CoCr: moderate artefact, MR Conditional at 1.5T
- Stainless steel 316L: most artefact, MR Conditional at 1.5T
- PEEK: MR Safe — no artefact (polymer, not metal)
Artefact Reduction (SWIMS)
- Spin echo over gradient echo (refocusing pulse corrects field distortion)
- Wider bandwidth (reduces artefact extent, increases noise)
- Inversion recovery = STIR (not chemical fat sat near metal)
- MAVRIC-SL / SEMAC (dedicated multi-spectral sequences)
- Smaller voxels / lower field (1.5T, not 3T)
Evidence Base
MRI Safety Update 2008: Screening Patients for MRI
- Systematic pre-MRI screening (a standardised questionnaire plus active verbal interview) is the cornerstone of patient safety, identifying implants, devices, and foreign bodies before scanning.
- Implant and device safety must be assessed against the current ASTM terminology — MR Safe, MR Conditional, MR Unsafe — and the obsolete term 'MR compatible' should be abandoned.
- Conditions specified for an MR Conditional device (static field strength, spatial gradient, SAR, time-varying gradients) must all be satisfied; an implant cleared at 1.5T is not automatically safe at 3T.
Projectile Cylinder Accidents in the MR Suite
- Ferromagnetic nitrous oxide and oxygen cylinders brought into the scanner room became dangerous projectiles drawn toward the bore.
- Four of the last five projectile accidents at the reporting institutions occurred within the preceding three years, despite existing screening policies and staff education.
- Projectile incidents continue to occur and may be increasing, underscoring that policy alone is insufficient without enforced physical access control.
Safety evidence underscores the importance of screening and protocol adherence.