Iodinated and Gadolinium Contrast in Orthopaedic Practice
- Iodinated contrast (CT): reactions are anaphylactoid (NOT IgE-mediated), cannot be predicted by skin testing, and require immediate treatment if severe.
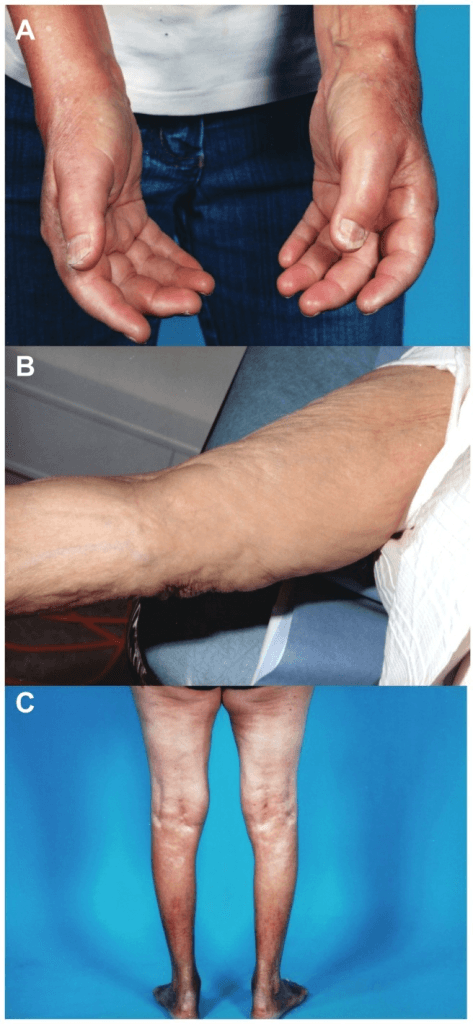
- Gadolinium contrast (MRI): associated with nephrogenic systemic fibrosis (NSF) in patients with severe renal impairment (eGFR less than 30).
- Contrast-induced nephropathy (CIN) is a transient decline in renal function after iodinated contrast — risk is highest with pre-existing renal impairment.
- Adrenaline (epinephrine) 0.5mg IM is the FIRST-LINE treatment for anaphylaxis from contrast media — not antihistamines or steroids.
- Premedication with steroids and antihistamines does NOT prevent all reactions but reduces their severity.
- “Iodinated contrast reactions are NOT true allergies — they are anaphylactoid (direct mast cell degranulation, not IgE-mediated).
- “A previous iodinated contrast reaction increases the risk of future reaction 5-6 fold but does NOT predict the severity of the next reaction.
- “Metformin should be withheld for 48 hours after iodinated contrast in patients with eGFR less than 30 due to the risk of lactic acidosis if AKI develops.
- “Gadolinium-based contrast agents are classified by the ACR into Group I (linear agents, greatest NSF risk), Group II (macrocyclic agents and the stable linear gadobenate, lowest NSF risk), and Group III (gadoxetate, limited data).
- “Breastfeeding does NOT need to be interrupted after iodinated or gadolinium contrast — less than 0.04% of dose enters breast milk.
Contrast agent safety is a high-yield exam topic, particularly the management of anaphylaxis and renal protection strategies. You must be able to: classify contrast reactions, manage anaphylaxis (adrenaline first-line, dose, route), explain the mechanism of contrast-induced nephropathy, discuss prevention strategies (hydration, eGFR thresholds), and differentiate iodinated from gadolinium contrast risks. A common trap is treating anaphylaxis with antihistamines instead of adrenaline.
HYDRATECIN Prevention
Hook:HYDRATE to protect the kidneys: Hydration is the single most effective CIN prevention strategy.
NSFGadolinium Safety
Hook:NSF: the unique and potentially fatal risk of gadolinium contrast in patients with severe kidney disease.
Overview
Contrast agents are used in orthopaedic imaging to enhance tissue differentiation and improve diagnostic accuracy. Iodinated contrast is used for CT, fluoroscopy, and conventional arthrography, while gadolinium-based contrast agents (GBCAs) are used for MRI. Although contrast-enhanced imaging is not routinely required for most musculoskeletal conditions, it plays a critical role in specific scenarios: tumour staging, infection assessment, vascular evaluation, arthrography, and post-operative assessment.
Understanding contrast agent pharmacology, reaction management, and renal safety is essential for all orthopaedic surgeons, not just radiologists, because orthopaedic patients frequently require contrast-enhanced imaging and the operating surgeon may need to manage contrast reactions in the perioperative setting.
Iodinated contrast works by absorbing X-rays due to the high atomic number of iodine (Z=53). Modern agents are non-ionic and low-osmolar (e.g., iohexol, iopamidol), which significantly reduced reaction rates compared to older ionic high-osmolar agents. Iodinated contrast is excreted renally and is the agent associated with contrast-induced nephropathy (CIN). Orthopaedic applications include: CT angiography, contrast-enhanced tumour assessment, and CT arthrography.
Gadolinium is a paramagnetic metal that shortens the T1 relaxation time of nearby water molecules, causing T1-bright signal at the site of accumulation. GBCAs are chelated (bound to a molecular cage) to reduce toxicity. The key safety concern is nephrogenic systemic fibrosis (NSF) in severe renal impairment (eGFR less than 30). Modern macrocyclic agents (e.g., gadobutrol, gadoterate) have the lowest NSF risk due to their more stable chelate structure. Orthopaedic applications: MR arthrography, tumour enhancement, infection assessment, post-operative evaluation.
Gadolinium Agent Classification: ACR Groups and NSF Risk
The topic repeatedly refers to "Group I/II/III" gadolinium agents and a viva explicitly asks for them, but the scheme is never set out. The ACR classifies gadolinium-based contrast agents by their association with nephrogenic systemic fibrosis. The numbering is counter-intuitive: Group I is the HIGHEST-risk (linear) group, not the safest.
- Agents
- Linear agents: gadodiamide, gadopentetate, gadoversetamide
- NSF risk and use
- Associated with the GREATEST number of NSF cases; avoid in eGFR under 30 (most have been suspended or withdrawn in Europe)
- Agents
- Macrocyclic agents (gadobutrol, gadoterate, gadoteridol) plus the more stable linear gadobenate
- NSF risk and use
- Few or NO unconfounded NSF cases - the LOWEST risk and the standard choice, usable with caution even in chronic kidney disease
- Agents
- Gadoxetate disodium (a liver-specific agent)
- NSF risk and use
- Limited NSF data available; used for specific hepatobiliary indications
The key is chelate stability. Linear (open-chain) chelates hold the gadolinium ion less tightly, so during prolonged retention in severe renal impairment they release more free (toxic) gadolinium, which triggers NSF. Macrocyclic chelates fully encage the ion in a rigid ring and release almost none. This is why the Group II macrocyclics are preferred whenever gadolinium is essential, and why the European regulator suspended most Group I linear agents in 2017.
Systematic Approach
Pre-Contrast Safety Assessment
- Assessment
- Ask about any prior reaction to contrast media and its severity
- Action Required
- If prior reaction: risk is 5-6x higher. Consider premedication, alternative imaging, or radiology consultation
- Assessment
- Check eGFR within the last 3 months for iodinated contrast; within 6 months for gadolinium
- Action Required
- eGFR less than 30: high CIN risk (iodinated) and NSF risk (gadolinium). Hydrate and use minimum contrast volume
- Assessment
- History of asthma, atopy, or other drug allergies
- Action Required
- Asthma increases contrast reaction risk 5-10x. Ensure bronchodilator available. Consider premedication
- Assessment
- Metformin, NSAIDs, aminoglycosides, diuretics
- Action Required
- Withhold metformin 48h post-contrast if eGFR less than 30. Avoid nephrotoxins. Ensure adequate hydration
- Assessment
- Pregnancy status and breastfeeding
- Action Required
- Iodinated contrast: avoid in pregnancy unless essential. Gadolinium: avoid in pregnancy (crosses placenta). Breastfeeding: can continue after both agents
- Assessment
- Resuscitation equipment must be immediately available
- Action Required
- Adrenaline, oxygen, IV access, suction, monitoring equipment must be on-site whenever contrast is administered
Iodinated Contrast Reactions
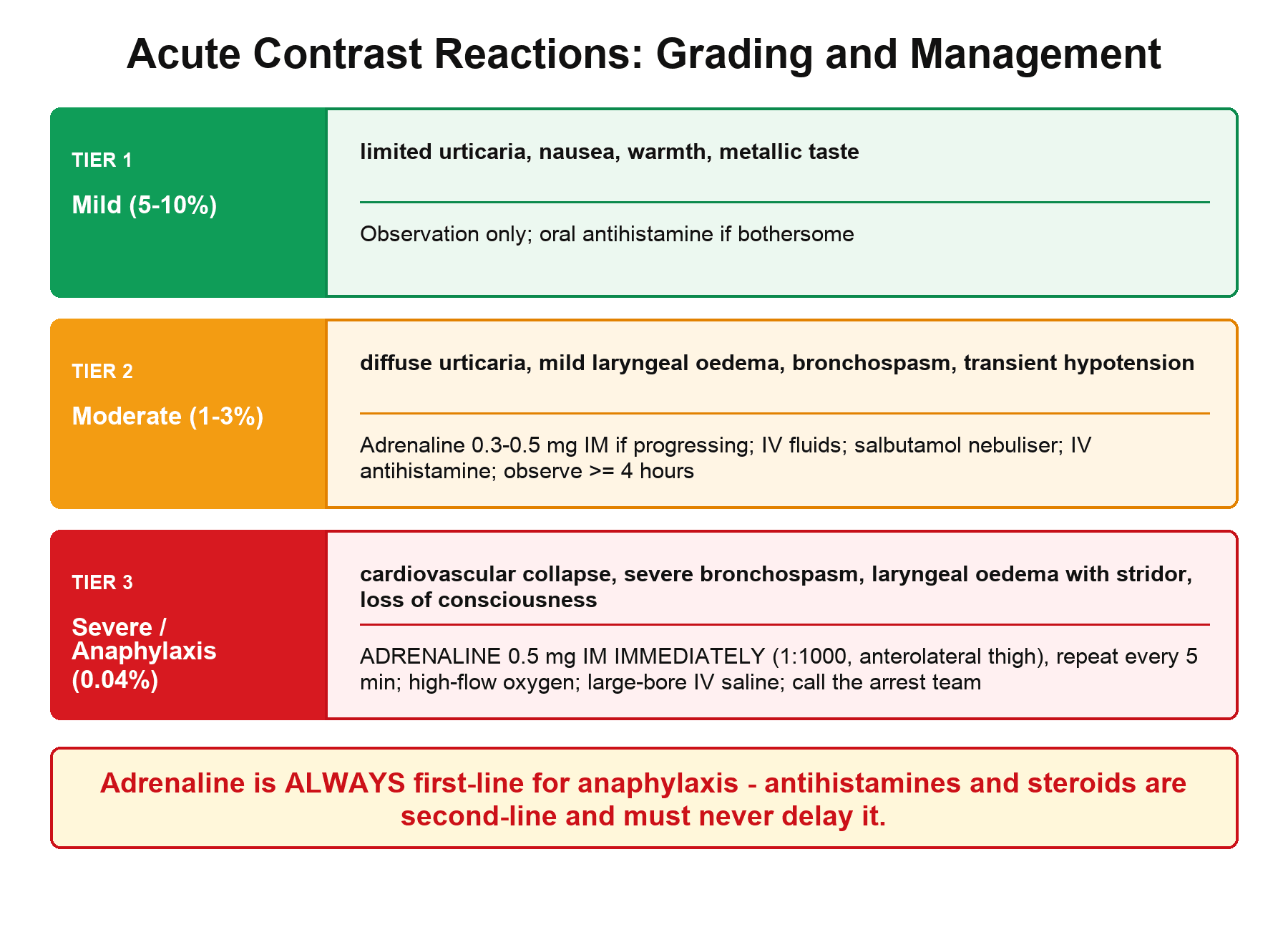
Classification and Management of Iodinated Contrast Reactions
- Symptoms
- Limited urticaria, pruritus, nausea, warmth, metallic taste, sneezing, mild headache
- Incidence
- 5-10%
- Management
- Observation only. Most resolve spontaneously. May give oral antihistamine if symptoms are bothersome
- Symptoms
- Diffuse urticaria, facial/laryngeal oedema (mild), bronchospasm (responsive), hypotension (transient, responds to fluids)
- Incidence
- 1-3%
- Management
- Medical treatment required: adrenaline 0.3-0.5mg IM if progressing, IV fluids, salbutamol nebuliser for bronchospasm, antihistamine IV, observation minimum 4 hours
- Symptoms
- Cardiovascular collapse, severe bronchospasm, laryngeal oedema with stridor, loss of consciousness, seizures, respiratory arrest
- Incidence
- 0.04%
- Management
- ADRENALINE 0.5mg IM IMMEDIATELY (1:1000, anterolateral thigh). Repeat every 5 min. High-flow oxygen. Large-bore IV saline. Call arrest team. Transfer to resuscitation area
Key principles:
- Iodinated contrast reactions are anaphylactoid (direct mast cell degranulation), NOT true IgE-mediated allergies. This means they can occur on first exposure and cannot be predicted by skin testing.
- Adrenaline is ALWAYS the first-line treatment for anaphylaxis — it reverses bronchospasm, supports blood pressure, and reduces oedema.
- Antihistamines and corticosteroids are SECOND-LINE adjuncts — they should NEVER delay adrenaline administration.
- All moderate and severe reactions require a minimum observation period and documentation for future reference.
Biphasic Reactions and Post-Reaction Observation
The anaphylaxis management and viva repeatedly invoke the "biphasic reaction" and the minimum observation period, but the concept is never defined - yet it is the entire reason a patient is watched after a severe reaction has apparently settled.
- Time course
- A single episode that resolves with treatment and does not recur
- Implication
- Standard observation, then discharge with documentation
- Time course
- Symptoms resolve, then RECUR without any re-exposure, usually within 1 to 72 hours (often about 8 to 10 hours)
- Implication
- The reason for a minimum observation period; the second phase can be as severe as the first and is re-treated as new anaphylaxis (adrenaline first)
- Time course
- Anaphylaxis persists for hours despite treatment
- Implication
- Needs ongoing resuscitation and critical-care support
After a moderate or severe contrast anaphylaxis, observe the patient for a minimum period (commonly several hours, and longer when the initial reaction was severe or required repeated adrenaline). A biphasic reaction occurs in a minority of cases and can be life-threatening. Corticosteroids are given as an adjunct but do NOT reliably prevent the biphasic phase, so the protection that actually matters is adequate first-line adrenaline plus a sufficient monitored observation window, with immediate re-treatment if symptoms recur.
ABCDAContrast Reaction Management
Hook:ABCDA: Adrenaline first, then Breathing, Circulation, Drugs, and Arrest team. Remember: ADRENALINE saves lives, not antihistamines.
Contrast-Induced Nephropathy
Contrast-Induced Nephropathy (CIN)
CIN is defined as an acute decline in renal function (rise in serum creatinine of 25% or more, or 44 micromol/L or more above baseline) occurring within 48-72 hours of iodinated contrast administration, in the absence of another cause.
- Risk Factor
- eGFR less than 30 (highest risk), eGFR 30-60 (moderate risk)
- Management
- IV hydration: N/S 1mL/kg/hr for 12h pre and 12h post. Use lowest contrast volume
- Risk Factor
- Diabetic nephropathy compounds the risk, especially with metformin
- Management
- Withhold metformin for 48h post-contrast if eGFR less than 30 (risk of lactic acidosis if AKI develops). Check creatinine before restarting
- Risk Factor
- Hypovolaemia reduces renal perfusion and concentrates contrast in tubules
- Management
- Ensure adequate hydration; correct volume depletion before contrast
- Risk Factor
- NSAIDs, aminoglycosides, ACE inhibitors, diuretics
- Management
- Withhold nephrotoxins if clinically safe. Ensure volume status is optimised
- Risk Factor
- Larger volumes increase the osmotic and direct toxic load on the kidneys
- Management
- Use the minimum effective dose. Avoid repeated contrast studies within 48-72 hours
- Risk Factor
- High-osmolar ionic contrast has the highest CIN risk
- Management
- Use low-osmolar or iso-osmolar non-ionic contrast for all patients
CIN is typically transient: creatinine peaks at 3-5 days and returns to baseline within 7-14 days in the majority of cases. However, a small proportion of patients (particularly those with severely impaired baseline renal function) may develop persistent renal impairment or require temporary dialysis. The risk of permanent dialysis-dependent renal failure from CIN is very low in the general population but clinically significant in high-risk patients (eGFR less than 15, diabetic nephropathy, heart failure).
Guidelines, Registries & Global Practice
Contrast media safety is governed by broadly convergent international guidance, with non-ionic low-osmolar iodinated agents and macrocyclic gadolinium agents now standard worldwide. The main areas of genuine divergence are the eGFR thresholds for renal precautions and the role of premedication.
Global Epidemiology
- Iodinated contrast acute reactions: mild 0.5-3% and severe approximately 0.04% with low-osmolar agents (down from approximately 0.22% with the older high-osmolar agents).
- Gadolinium acute reactions are rarer (roughly 0.04-0.07% overall); confirmed NSF is now exceedingly rare since linear agents were restricted, with virtually no unconfounded cases reported after macrocyclic-only exposure.
- Contrast-associated AKI: historically reported in 2-25% of at-risk patients, but contemporary controlled data (propensity-matched and RCT) suggest the true attributable risk from modern IV contrast is much lower than once believed, especially above eGFR 30.
Side-by-Side Guideline Comparison
- Renal / CIN threshold
- Prophylactic hydration for eGFR under 30 (or AKI); routine renal screening targeted by risk
- Gadolinium / NSF
- Group II macrocyclic agents considered very low NSF risk even in CKD; group-based classification
- Premedication stance
- Recognises premedication value but highlights breakthrough reactions and high number needed to treat
- Renal / CIN threshold
- Volume expansion advised for eGFR under 30 (IV contrast) / under 45 (intra-arterial first-pass)
- Gadolinium / NSF
- Avoid high-risk linear agents in severe CKD; macrocyclic preferred
- Premedication stance
- Steroid premedication for prior moderate/severe reaction; emphasises shared decision-making
- Renal / CIN threshold
- Risk-stratified hydration; pragmatic thresholds around eGFR 30
- Gadolinium / NSF
- Restricts linear GBCAs; macrocyclic standard
- Premedication stance
- Premedication for prior reaction; resuscitation readiness mandatory
- Renal / CIN threshold
- Labelling-based renal cautions
- Gadolinium / NSF
- EMA suspended most linear GBCAs (2017); FDA retained with boxed warning and patient medication guide
- Premedication stance
- Class labelling on reaction risk
High- vs Limited-Resource Practice Variation
- Well-resourced settings: macrocyclic gadolinium exclusively, point-of-care creatinine, structured premedication and anaphylaxis pathways, and routine post-contrast monitoring.
- Limited-resource settings: high-osmolar ionic agents may still be used for cost reasons (higher reaction rates), eGFR may be unavailable before urgent imaging, and adrenaline or resuscitation equipment may not be immediately at the contrast injection site — the single most important safety gap to close.
- Universal minimum standard everywhere: adrenaline, oxygen, IV access and trained staff must be immediately available wherever contrast is injected, regardless of setting.
Controversies & Areas of Uncertainty
Much historical "contrast-induced nephropathy" reflected the natural creatinine fluctuation of sick patients rather than contrast toxicity. Propensity-matched studies and the AMACING trial suggest the attributable risk of modern intravenous low-osmolar contrast is small, especially above eGFR 30. The preferred term is now "contrast-associated AKI" (temporal association) versus "contrast-induced AKI" (proven causation). Renal anxiety should not delay a clinically essential scan.
Premedication reduces but does not abolish reactions, and the number needed to treat to prevent one severe reaction is very high (over 500 in the Mervak data). Mandatory 13-hour steroid regimens can delay urgent imaging and cause hyperglycaemia. Many centres now reserve full premedication for prior moderate/severe reactions and favour switching the contrast agent plus close observation.
Macrocyclic agents deposit far less gadolinium than linear agents, but trace deposition still occurs in the dentate nucleus and globus pallidus with repeated dosing. No clinical harm has been proven, yet the principle of lowest effective cumulative dose and macrocyclic-only use is now standard.
Once widely used for renal protection, both were shown to be no better than plain saline in the large PRESERVE trial and should no longer be used routinely. Isotonic saline volume expansion in the highest-risk patients remains the only consistently endorsed pharmacological measure.
Iodinated vs Gadolinium Contrast
- Iodinated (CT/fluoroscopy)
- High atomic number iodine absorbs X-rays (radiodensity)
- Gadolinium (MRI)
- Paramagnetic gadolinium shortens T1, producing T1-bright signal
- Iodinated (CT/fluoroscopy)
- Anaphylactoid reaction (approximately 0.04% severe); higher than gadolinium
- Gadolinium (MRI)
- Acute reactions rarer than iodinated contrast
- Iodinated (CT/fluoroscopy)
- Contrast-associated AKI (attributable risk small with modern agents)
- Gadolinium (MRI)
- Nephrogenic systemic fibrosis with high-risk agents in eGFR under 30
- Iodinated (CT/fluoroscopy)
- Non-ionic low-osmolar (e.g. iohexol, iopamidol)
- Gadolinium (MRI)
- Macrocyclic (e.g. gadobutrol, gadoterate, gadoteridol)
- Iodinated (CT/fluoroscopy)
- Withhold if eGFR under 30 (lactic acidosis risk if AKI develops)
- Gadolinium (MRI)
- No metformin interaction
- Iodinated (CT/fluoroscopy)
- Use only if essential
- Gadolinium (MRI)
- Avoid — crosses placenta; reserve for compelling indication
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient collapses with severe bronchospasm, hypotension, and urticaria immediately after receiving iodinated contrast for a CT scan.”
“A 72-year-old patient with an eGFR of 25 requires a contrast-enhanced CT scan for staging of a suspected bone tumour.”
“An examiner asks you about nephrogenic systemic fibrosis (NSF) — what it is, who is at risk, and how to minimise the risk.”
Anaphylaxis Management (ABCDA)
- A: Adrenaline 0.5mg IM (1:1000) — FIRST LINE, anterolateral thigh, repeat every 5 min
- B: Breathing — high-flow O2, salbutamol nebuliser for bronchospasm
- C: Circulation — large-bore IV access, rapid saline bolus
- D: Drugs — antihistamine and hydrocortisone are SECOND LINE only
- A: Arrest team — 6-hour minimum observation for severe reactions
Contrast-Induced Nephropathy
- Definition: 25% or 44 micromol/L creatinine rise within 48-72 hours
- Risk highest at eGFR less than 30 (CKD Stage 4-5)
- Prevention: IV saline hydration (most effective), low contrast volume, avoid nephrotoxins
- Withhold metformin 48h post-contrast if eGFR less than 30
- Usually self-limiting: peaks at 3-5 days, resolves within 7-14 days
Gadolinium Safety
- NSF risk in severe renal impairment (eGFR less than 30) — potentially fatal fibrosis
- Group II (macrocyclic): lowest NSF risk — use these if gadolinium essential
- Group I (linear): highest NSF risk — AVOID in renal impairment
- Check eGFR before ALL gadolinium studies
- Gadolinium brain deposition: clinical significance unclear; macrocyclic agents deposit less
Key Myths Debunked
- Shellfish allergy ≠ iodine allergy (tropomyosin protein allergy, not iodine)
- Reactions are anaphylactoid (not IgE-mediated) — can occur on first exposure
- Breastfeeding does NOT need to stop after contrast (less than 0.04% enters milk)
- Premedication reduces but does NOT eliminate reaction risk
Evidence Base
Adverse Reactions to Ionic vs Non-Ionic Contrast (Katayama / Japanese Committee)
- Nationwide prospective study of 337,647 examinations (169,284 ionic, 168,363 non-ionic).
- Overall adverse reaction rate was 12.66% for ionic high-osmolar contrast vs 3.13% for non-ionic low-osmolar contrast.
- Severe reactions occurred in 0.22% (ionic) vs 0.04% (non-ionic); one death occurred in each group, with no proven causal relationship to contrast.
Breakthrough Reactions Despite Premedication
- Among 1,051 inpatients completing 13-hour corticosteroid and diphenhydramine premedication before contrast-enhanced CT, the overall breakthrough reaction rate was 1.2%.
- Patients premedicated because of a previous contrast reaction had a breakthrough rate of 2.1% (3-4 times the 0.6% ordinary rate in the general population); those premedicated for other reasons had a 0% breakthrough rate.
- There were NO severe breakthrough reactions; the number needed to treat was 69 to prevent any reaction and 569 to prevent a severe reaction.
Non-ionic contrast and premedication reduce but do not eliminate reaction risk.