From Standard Radiographs to Advanced MRI Assessment
- Minimum shoulder trauma series: AP in internal rotation + true axillary lateral. The axillary lateral confirms or excludes dislocation.
- Systematic radiograph reading: ABCS -- Alignment, Bone density, Cartilage spaces, Soft tissues.
- MRI is the gold standard for rotator cuff assessment. Ultrasound is a valid alternative with equivalent sensitivity in experienced hands.
- MR arthrography (direct) is the most accurate test for labral pathology and partial-thickness cuff tears, outperforming non-contrast MRI; joint distension is key to demonstrating capsulolabral detachment.
- CT with three-dimensional reconstruction is essential for glenoid bone loss quantification -- more than 20-25% loss mandates bony procedure (Latarjet).
- “The Hill-Sachs lesion is best seen on AP internal rotation radiograph. The Bankart lesion (bony) is best seen on Bernageau profile view or CT.
- “Acromion morphology (Bigliani classification): Type I flat, Type II curved, Type III hooked -- Type III associated with impingement.
- “Critical shoulder angle (CSA): more than 35 degrees = higher cuff tear risk; less than 30 degrees = higher OA risk.
- “Rotator cuff tear grading on MRI: high signal on T2 within tendon = tear. Full-thickness: extends from articular to bursal surface.
- “The crescent sign on MRI = high T2 signal at the articular margin of the supraspinatus insertion -- suggests partial articular-surface tear.
Systematic shoulder imaging is one of the most commonly tested musculoskeletal imaging topics. You must be able to: describe the standard radiographic views and what each shows, read a shoulder radiograph systematically (ABCS), select appropriate advanced imaging (MRI vs MRA vs CT vs USS), and interpret key MRI findings (cuff tears, labral tears, acromion morphology). Classic traps: not requesting an axillary lateral in trauma (missing a dislocation) and relying on non-contrast MRI for labral assessment.
CRISTKey MRI Findings in Shoulder Pathology
Hook:CRIST: a systematic MRI checklist ensuring complete shoulder assessment.
Overview
The shoulder is the most commonly imaged upper limb joint in orthopaedic practice, with a broad spectrum of pathology ranging from acute trauma (dislocation, fracture) to chronic conditions (rotator cuff disease, instability, arthritis). A systematic approach to shoulder imaging is essential for both the clinical setting and the fellowship examination, where candidates are frequently asked to describe radiographic views, select appropriate advanced imaging, and interpret MRI findings.
The imaging workup begins with plain radiographs in virtually all presentations. Advanced imaging (MRI, ultrasound, CT, arthrography) is selected based on the specific clinical question. Understanding which modality best answers which question is a key examination skill.
Acute trauma: Radiographs (AP + axillary lateral minimum). If complex fracture: CT with three-dimensional reconstruction for surgical planning. Rotator cuff symptoms: MRI (non-contrast) or USS. If partial tear suspected on USS: MRI for confirmation. Instability: MR arthrography for labral assessment + CT with three-dimensional reconstruction for bone loss. Calcific tendinitis: AP radiograph + ultrasound. Frozen shoulder: Usually clinical diagnosis. MR arthrography if diagnostic uncertainty. OA assessment: True AP (Grashey) + axillary lateral radiographs.
Missing a posterior dislocation: the AP view may look near-normal (lightbulb sign). The axillary lateral is ESSENTIAL to confirm direction of dislocation. Missing a bony Bankart: standard radiographs often miss anterior glenoid rim fractures. CT or West Point view is needed. Overdiagnosing labral tears: sublabral foramen (12-18%) and Buford complex are NORMAL VARIANTS. Underestimating cuff tears on non-contrast MRI: partial articular-surface tears are best detected on MR arthrography.
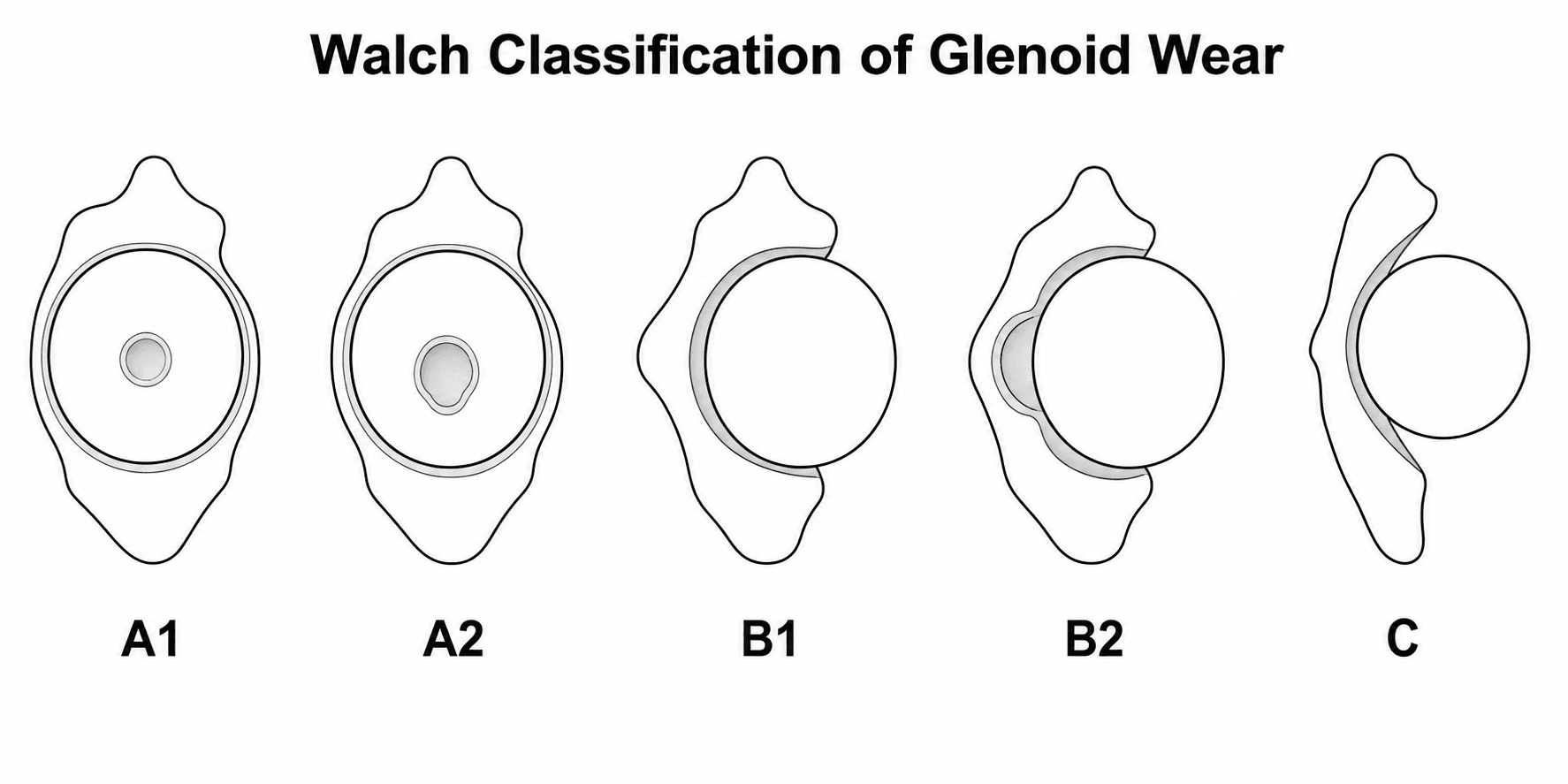
Walch Classification of Glenoid Wear
The modality-selection, differential and guideline sections all invoke the "Walch classification" for CT arthroplasty planning, but it is never set out. Walch grades the glenoid wear pattern of primary glenohumeral osteoarthritis on the axial CT (or MRI), and it drives the choice between anatomic and reverse shoulder arthroplasty.
- Glenoid morphology
- Centred humeral head, minor central erosion
- Implication
- Symmetric wear; well suited to anatomic total shoulder arthroplasty
- Glenoid morphology
- Centred head, major central erosion (head cups into the glenoid)
- Implication
- Symmetric but significant medial wear
- Glenoid morphology
- Posterior subluxation with posterior joint-space narrowing/sclerosis, no bone erosion
- Implication
- Asymmetric, early posterior wear
- Glenoid morphology
- Biconcave glenoid — posterior erosion creates a neoglenoid, with retroversion
- Implication
- Posterior wear and instability complicate anatomic arthroplasty
- Glenoid morphology
- Monoconcave but markedly retroverted / posteriorly worn (modified Walch)
- Implication
- Severe retroversion without a frank biconcavity
- Glenoid morphology
- Dysplastic glenoid, retroversion over 25 degrees (congenital)
- Implication
- High fixed retroversion
- Glenoid morphology
- Glenoid anteversion or anterior humeral subluxation (modified Walch)
- Implication
- Anterior wear pattern
Posteriorly worn, retroverted glenoids (B2, B3 and dysplastic C) make anatomic total shoulder arthroplasty prone to component malposition, persistent posterior instability and eccentric 'rocking-horse' glenoid loosening. These patterns push toward an augmented glenoid component, posterior bone grafting, or a reverse shoulder arthroplasty — which is exactly why the Walch type is read off the pre-operative CT.
Systematic Approach
Systematic Shoulder Imaging Assessment
- First-Line Imaging
- AP + axillary lateral radiographs (MINIMUM 2 views)
- Advanced Imaging
- CT with three-dimensional reconstruction for complex fractures (proximal humerus, glenoid). MRI for associated soft tissue injury after fracture management
- First-Line Imaging
- AP radiograph (acromiohumeral distance, calcification)
- Advanced Imaging
- MRI (gold standard) or USS by experienced operator. MRA if partial tear suspected
- First-Line Imaging
- AP + axillary lateral (Hill-Sachs, bony Bankart)
- Advanced Imaging
- MR arthrography (labral tears, capsular pathology) + CT three-dimensional reconstruction (glenoid bone loss quantification)
- First-Line Imaging
- Zanca view (10-15 degree cephalic tilt AP)
- Advanced Imaging
- MRI for distal clavicle oedema (osteolysis), ligament assessment. Weighted views for instability (controversial)
- First-Line Imaging
- AP radiograph (demonstrates calcification)
- Advanced Imaging
- Ultrasound (confirms location, guides barbotage/aspiration). No MRI needed for isolated calcific tendinitis
- First-Line Imaging
- True AP (Grashey) + axillary lateral
- Advanced Imaging
- CT for glenoid wear pattern (Walch classification) pre-arthroplasty planning. MRI for associated cuff status
ABCSSystematic Shoulder Radiograph Reading
Hook:ABCS: the systematic approach that ensures you never miss a finding on shoulder radiographs.
Radiographic Assessment
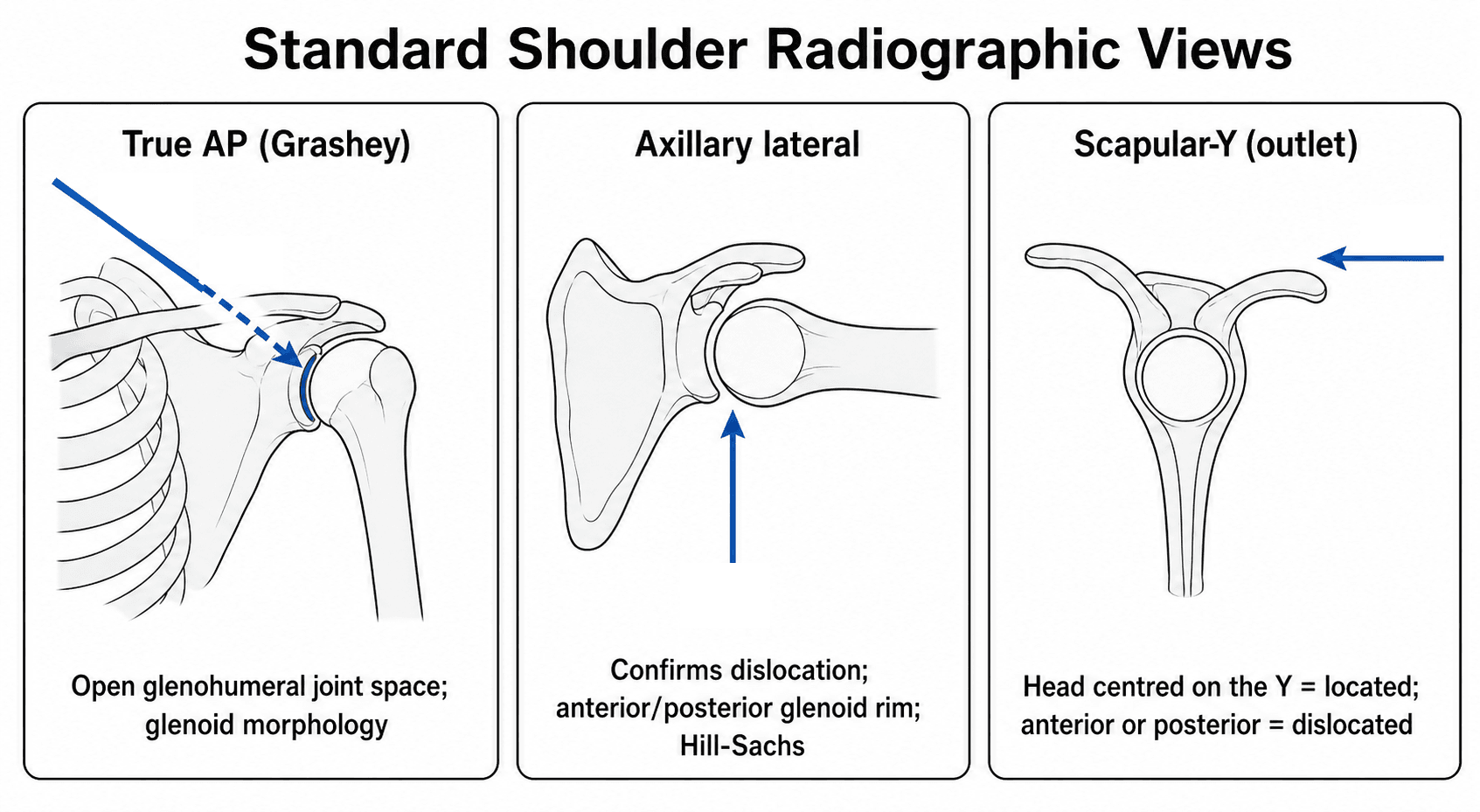
Standard Shoulder Radiographic Views
AP in internal rotation: The arm is internally rotated, positioning the greater tuberosity in profile (overlapping the humeral head). This view shows: Hill-Sachs lesion (posterolateral humeral head compression fracture from anterior dislocation), glenohumeral joint space, and acromial morphology.
AP in external rotation: The arm is externally rotated, positioning the greater tuberosity laterally. This view shows: the greater tuberosity in profile (best for tuberosity fractures), the bicipital groove, and the humeral head articular surface.
True AP (Grashey view): The beam is angled 40 degrees to align with the glenohumeral joint plane. This eliminates overlap between the humeral head and glenoid, providing the most accurate assessment of joint space width and glenoid morphology.
Axillary lateral: ESSENTIAL for trauma. The patient is supine or seated with the arm abducted. The beam passes through the axilla from inferior to superior. This view shows: glenohumeral relationship (confirms or excludes dislocation), anterior and posterior glenoid rim (bony Bankart), Hill-Sachs lesion, and coracoid process.
Y-view (scapular lateral): The beam is tangential to the scapular spine. Shows the relationship of the humeral head to the glenoid fossa -- the head should be centred over the glenoid Y. Anterior dislocation: head is anterior to the Y. Posterior dislocation: head is posterior.
Acromiohumeral distance: Measured on the AP view from the inferior surface of the acromion to the superior surface of the humeral head. Normal: more than 7mm. Less than 7mm suggests massive rotator cuff tear with superior migration of the humeral head.

ATWAStandard Shoulder Radiographic Views
Hook:ATWA: AP, True AP, West Point, Axillary -- know which view shows what.
Differential Diagnosis on Imaging
Several shoulder conditions overlap clinically; imaging is what separates them. The table below highlights the discriminating imaging features the examiner expects.
- Key imaging finding
- Fluid-signal gap through the tendon; reduced acromiohumeral distance if massive
- Best modality / pitfall
- MRI or ultrasound; pitfall -- many tears are asymptomatic in older patients
- Key imaging finding
- Dense calcification over the supraspinatus on radiograph
- Best modality / pitfall
- Radiograph plus ultrasound; pitfall -- resorptive (fluffy) phase is most painful
- Key imaging finding
- Often normal radiograph; MR arthrography may show reduced axillary recess volume and rotator-interval/coracohumeral ligament thickening
- Best modality / pitfall
- Clinical diagnosis; imaging mainly excludes mimics
- Key imaging finding
- Anteroinferior labral and bony glenoid defect, posterolateral Hill-Sachs
- Best modality / pitfall
- MR arthrography plus CT for bone loss; pitfall -- normal sublabral variants
- Key imaging finding
- Lightbulb sign on AP, head behind the scapular Y
- Best modality / pitfall
- Axillary lateral is decisive; pitfall -- AP can look near-normal
- Key imaging finding
- Joint-space loss, inferior osteophyte (goat's beard), posterior glenoid wear
- Best modality / pitfall
- Grashey AP plus axillary; CT (Walch) for arthroplasty planning
- Key imaging finding
- Sublabral foramen, Buford complex (cord-like MGHL, absent anterosuperior labrum)
- Best modality / pitfall
- MR arthrography; pitfall -- do NOT call these SLAP/Bankart tears
Labral Lesions: SLAP and the Bankart Variants
The CRIST checklist and the vivas name SLAP, Bankart, ALPSA and HAGL lesions, but the labral-lesion classification itself is never developed — and naming the lesion precisely on MR arthrography is a classic viva. The superior labrum is graded by the Snyder SLAP system; the anteroinferior labrum has its own family of named variants.
- Lesion
- Fraying/degeneration of the superior labrum, biceps anchor intact
- Note
- Often degenerative; usually debrided
- Lesion
- Detachment of the superior labrum AND biceps anchor from the glenoid
- Note
- The commonest surgical SLAP; anterior, posterior and combined subtypes
- Lesion
- Bucket-handle tear of the superior labrum with an INTACT biceps anchor
- Note
- Displaced fragment may cause mechanical symptoms
- Lesion
- Bucket-handle tear extending INTO the biceps tendon
- Note
- Biceps involvement changes the repair/tenodesis decision
- What it is
- Anteroinferior labrum and IGHL avulsed from the glenoid with periosteal disruption
- Imaging clue
- Contrast tracks under the detached labrum on MR arthrography
- What it is
- Bankart with an anteroinferior glenoid rim fracture
- Imaging clue
- CT for bone-loss quantification (Latarjet threshold)
- What it is
- Labrum with INTACT periosteum strips and heals MEDIALISED on the glenoid neck
- Imaging clue
- Medially displaced, rounded labral mass (chronic)
- What it is
- Labrum avulsed but periosteum intact and the labrum non-displaced
- Imaging clue
- Easily missed; the ABER MR-arthrography view lifts it off the glenoid
- What it is
- Anteroinferior labral tear PLUS an articular cartilage injury
- Imaging clue
- Usually stable; look for the cartilage defect
- What it is
- Inferior glenohumeral ligament avulsed from the HUMERAL side (not the glenoid)
- Imaging clue
- 'J sign' on coronal MR arthrography; bony variant is BHAGL
The Perthes lesion is the classic miss because the labrum sits in a near-normal position — the ABER (abduction-external rotation) view on MR arthrography tensions the IGHL and reveals contrast under the labrum. Conversely, the normal sublabral foramen and Buford complex (cord-like middle glenohumeral ligament with an absent anterosuperior labrum) must NOT be reported as a Bankart or SLAP tear.
Guidelines, Registries & Global Practice
Across health systems, shoulder imaging follows the same evidence-based logic: plain radiographs first for nearly all presentations, then advanced imaging targeted to the specific clinical question. What varies between regions is which advanced modality is reached for first, driven by scanner access, sonographer expertise and cost.
Global epidemiology of the questions imaging must answer:
- Rotator cuff disease is the commonest cause of shoulder pain in adults; full-thickness cuff tear prevalence rises steeply with age, exceeding 50% in those over 80, and a large share are asymptomatic -- so imaging findings must always be interpreted against the clinical picture.
- Anterior glenohumeral dislocation is the most common large-joint dislocation; recurrence is highest in young, active patients, which is the group in whom glenoid bone loss and Hill-Sachs assessment most change management.
- Calcific tendinitis affects roughly 3-10% of adults, frequently incidental on radiographs.
- Cuff / impingement
- Radiographs first; MRI or ultrasound both acceptable for cuff tears, with ultrasound endorsed as cost-effective in experienced hands
- Instability / trauma
- Axillary or comparable orthogonal view mandatory; CT for glenoid bone loss in recurrent instability
- Cuff / impingement
- Plain films plus ultrasound as efficient first-line cuff assessment; MRI when ultrasound equivocal or surgery planned
- Instability / trauma
- Two orthogonal radiographs in every dislocation; cross-sectional imaging before stabilisation surgery
- Cuff / impingement
- Imaging focused on fracture characterisation; CT for displaced proximal humeral fractures and articular involvement
- Instability / trauma
- CT with 3D reconstruction for glenoid rim fractures and surgical planning
- Cuff / impingement
- ESSR consensus supports ultrasound as a first-line cuff tool and MR arthrography for partial tears
- Instability / trauma
- Direct MR arthrography favoured for labroligamentous assessment in instability
- Cuff / impingement
- Radiographs initial; MRI without contrast usually most appropriate for cuff/impingement
- Instability / trauma
- MR arthrography most appropriate for instability/labrum; CT for bone loss
Shoulder arthroplasty registries (UK NJR shoulder data, AOANJRR Australia, the Swedish and other national shoulder registries) reinforce why pre-operative imaging matters -- glenoid morphology (Walch classification on CT) and cuff/teres minor status (Goutallier on MRI) predict implant choice between anatomic and reverse arthroplasty and influence revision risk. These registries do not dictate which scan to order but make accurate pre-operative characterisation a quality issue.
Where MRI and skilled musculoskeletal sonography are scarce, radiographs (including dedicated instability views such as the West Point and Bernageau profile) and CT arthrography carry more diagnostic weight, and ultrasound -- being inexpensive, portable and radiation-free -- becomes the dominant cuff tool. In well-resourced centres, non-contrast MRI and direct MR arthrography are the defaults. The exam-correct principle is universal: choose the cheapest test that reliably answers the specific question, and never omit an orthogonal (axillary-equivalent) view in trauma.
Controversies & Areas of Uncertainty
The glenoid bone-loss threshold for adding a Latarjet to (or instead of) a Bankart repair is debated. Biomechanical and clinical work place it anywhere from about 13.5% to 25%, and the field is moving toward a combined glenoid-plus-Hill-Sachs (bipolar, glenoid-track) assessment rather than a single glenoid number. Subcritical loss (around 13.5-20%) increasingly prompts bony augmentation in high-demand patients.
Whether the Bigliani Type III hook is a developmental driver of impingement or an acquired traction enthesophyte remains unresolved, and the critical shoulder angle has partly supplanted acromial-shape grading as the cuff-risk parameter. Inter-observer reliability for both is only moderate.
Because asymptomatic cuff tears, labral variants and calcium deposits are common, advanced imaging risks over-treatment. The recurring controversy is how much weight to give an imaging abnormality that may not explain the patient's pain.
With comparable accuracy for cuff tears, the first-line choice is as much about local resources and sonographer skill as about evidence. Ultrasound's dynamic capability and point-of-care convenience must be weighed against MRI's comprehensive single-study assessment.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 60-year-old woman presents with a 6-month history of progressive shoulder pain and weakness in external rotation. Her AP radiograph shows an acromiohumeral distance of 5mm.”
“A 22-year-old soldier has had three anterior shoulder dislocations. His MRI shows a Bankart lesion. An examiner asks what additional imaging you need for surgical planning.”
“An examiner asks you to compare MRI, ultrasound, and MR arthrography for the assessment of rotator cuff pathology.”
Radiographic Views
- Trauma MINIMUM: AP + axillary lateral (confirms dislocation)
- Hill-Sachs: best on AP internal rotation
- Bony Bankart: best on axillary lateral or West Point view
- True AP (Grashey): best for joint space assessment
- AHD less than 7mm = massive cuff tear with superior migration
ABCS Systematic Reading
- Alignment: GH congruence, AC joint alignment, dislocation
- Bones: cortical outline (fractures), tuberosities, Hill-Sachs
- Cartilage spaces: GH joint space, AHD, AC joint
- Soft tissues: calcification, swelling, periosteal reaction
Advanced Imaging Selection
- MRI: gold standard for cuff assessment, comprehensive evaluation
- USS: equivalent to MRI for full-thickness tears, dynamic, cheaper
- MRA: most accurate for labral tears and partial-thickness cuff tears
- CT three-dimensional: glenoid bone loss quantification (more than 20-25% = Latarjet)
- CT arthrography: MRI alternative + bone detail
Key MRI Measurements
- Goutallier fatty infiltration: 0-4 (3-4 = irreversible, poor prognosis)
- Patte retraction: Stage 1 (at footprint), 2 (humeral head), 3 (glenoid)
- Critical shoulder angle: more than 35 = cuff tear risk, less than 30 = OA risk
- Bigliani acromion: Type I flat, II curved, III hooked (impingement risk)
Evidence Base
MRI vs Ultrasound vs MR Arthrography for Rotator Cuff Tears
- Pooled analysis of 65 studies (surgical reference standard) comparing MRI, MR arthrography and ultrasound for rotator cuff tears.
- MR arthrography was significantly more sensitive AND specific than either MRI or ultrasound for both full- and partial-thickness tears.
- No significant difference between MRI and ultrasound for either tear type. Area under the ROC curve: MRA 0.935, ultrasound 0.889, MRI 0.878.
Goutallier Classification for Fatty Muscle Degeneration
- Preoperative CT graded fatty muscle degeneration in five stages (0-4) in 63 patients before rotator cuff repair, with postoperative review of 57.
- Infraspinatus fatty degeneration worsened with time and, once present, never regressed after repair; it correlated with impaired pre- and post-operative external rotation.
- Infraspinatus degeneration had a strongly negative influence on supraspinatus repair outcome -- the authors concluded it is preferable to operate on wide tears before irreversible muscular damage occurs.
MR Arthrography vs Conventional MR and CT Arthrography
- 100 consecutive post-operative shoulders had conventional MR and MR arthrography on the same patients, all confirmed at arthroscopy.
- MR arthrography detected additional pathology missed by conventional MR -- 12 extra SLAP tears, several anterior/posterior labral tears and 9 extra full-thickness supraspinatus tears.
- In 22 patients with metallic artefact, CT arthrography revealed labral and cuff lesions not visible on MR.
Systematic clinical evidence guides imaging selection for rotator cuff pathology.