Load Sharing | Stress Shielding | Fracture Healing Mechanics
- Wolff's Law: Bone adapts to mechanical stress by remodeling architecture
- Stress shielding occurs when implant bears majority of load, leading to bone resorption
- Working length of construct determines flexibility (longer = more flexible)
- Screws fail by pullout or shear; plates fail by bending or fatigue fracture
- Torsional rigidity proportional to diameter to the 4th power
- “AO principles: Reduction, fixation, preservation of blood supply, early mobilization
- “Locked plating converts screws into fixed-angle device (more like external fixator)
- “Composite beam effect: Plate and bone together stronger than sum of parts
- “Elastic modulus mismatch causes stress concentration at implant-bone interface
Load sharing = implant and bone share load (bridge plating). Load bearing = implant carries all load (comminuted fracture, bone loss). Determines implant selection.
Distance between nearest screws on each side of fracture. Longer working length = more flexible construct = more callus but more implant stress.
Bone resorption from implant bearing load. Rigid plates reduce bone stress by 50-80%. Leads to refracture risk after implant removal.
Pullout strength proportional to thread engagement. Bicortical screws 2-3x stronger than unicortical. Stripping torque defines maximum tightness.
Overview and Introduction
Introduction to Implant Biomechanics
Successful fracture fixation requires understanding the biomechanical interaction between implant, bone, and healing tissue. The choice of fixation construct determines the stability type (absolute vs relative), which in turn influences the healing mechanism (primary vs secondary).
Key Biomechanical Principles:
- Load sharing: Implant and bone distribute load together
- Load bearing: Implant carries all load (comminuted fractures)
- Stress shielding: Excessive implant rigidity leads to bone resorption
- Working length: Distance between screws determines construct flexibility
Concepts and Fundamental Principles
Wolff's Law and Bone Adaptation
Wolff's Law states that bone adapts its structure to the mechanical demands placed upon it. Increased stress stimulates bone formation; decreased stress leads to resorption. This principle underlies stress shielding after rigid internal fixation.
- Rigid implant bears majority of load
- Bone stress reduced by 50-80%
- Remodeling leads to cortical thinning, porosity
- Refracture risk after implant removal
- Bridge plating preferred over compression plating in some cases
- Locked plates act as internal fixators, less stress shielding
- Gradual load sharing as fracture heals
- Delayed removal allows bone adaptation before unloading implant
Mechanical Properties of Implants
Elastic modulus mismatch between implant and bone creates stress concentration at the implant-bone interface, particularly at screw holes. This can lead to peri-implant fractures.
Interfragmentary Strain Theory (Perren)
Perren's interfragmentary strain theory is the unifying concept linking construct stability to the tissue that can form in the fracture gap, and examiners expect it.
Strain at the fracture is the relative change in gap width under load — the interfragmentary movement divided by the original gap width. A tissue can only form and survive in the gap if the local strain stays below the strain tolerance of that tissue:
- Approx. strain tolerated
- Under about 2%
- Implication
- Forms only in a very stable gap — the basis of direct/primary healing
- Approx. strain tolerated
- Up to roughly 10%
- Implication
- Forms with the controlled micromotion of relative stability
- Approx. strain tolerated
- Up to about 100%
- Implication
- Tolerates large motion; persists as fibrous nonunion if motion never falls
Two clinically vital corollaries follow:
- A gap that is too small can paradoxically fail to heal. With a tiny gap, even a small absolute movement produces a very high percentage strain that exceeds bone's tolerance — so an imperfectly stable simple fracture with a hairline gap can progress to nonunion. The answer is either true absolute stability (compress the gap towards zero motion) or deliberate relative stability with a larger effective gap.
- Comminution helps healing. Spreading the same total motion across many fracture lines means each individual gap sees only a fraction of the strain. This is why multifragmentary fractures bridged with a flexible construct heal readily by callus, whereas a single transverse gap is far less forgiving.
Strain = interfragmentary motion ÷ gap size. Bone needs roughly under 2% strain to form. A smaller gap raises the strain for the same motion, so a near-anatomic simple fracture must be either rigidly compressed (absolute stability) or given relative stability — "almost stable" is the recipe for nonunion. Comminution lowers strain per gap and favours callus.
Load Sharing vs Load Bearing
Definitions
- Load Sharing: Implant and bone both transmit load across the fracture site. Bone contributes to mechanical stability. Examples: Bridge plating of simple fractures, intramedullary nailing with cortical contact.
- Load Bearing: Implant carries all or most of the load. Bone contributes minimally due to comminution, bone loss, or non-union. Examples: Locked plating of segmental defects, arthroplasty, massive allografts.
- Load Sharing
- Significant (50%+)
- Load Bearing
- Minimal (under 20%)
- Clinical Example
- Simple vs comminuted fracture
- Load Sharing
- Lower, distributed
- Load Bearing
- Higher, concentrated
- Clinical Example
- Bridge plate vs locking plate with gap
- Load Sharing
- Bone failure more likely
- Load Bearing
- Implant fatigue fracture risk
- Clinical Example
- Refracture vs plate breakage
- Load Sharing
- Callus formation essential
- Load Bearing
- Biological healing may not occur
- Clinical Example
- Hypertrophic vs atrophic non-union
Load-bearing constructs require stronger implants and carry higher failure risk. If bone cannot contribute (segmental defect, severe comminution, infection with bone loss), consider stronger constructs (double plating, reconstruction nail, arthroplasty) or biological augmentation (bone graft, BMP).
Working Length and Construct Stiffness
Working Length Defined
Working length is the distance between the nearest screws on either side of the fracture site. It determines the flexibility of the construct.
- Short working length = rigid construct = less callus formation = higher implant stress
- Long working length = flexible construct = more callus = lower implant stress but higher strain at fracture
- Articular fractures requiring anatomic reduction
- Metaphyseal fractures with good bone quality
- Fractures where callus is undesirable
Maximum stability, minimal motion
Stress shielding, higher implant stress, less biological stimulus
- Diaphyseal fractures amenable to relative stability
- Osteoporotic bone requiring load distribution
- Fractures where callus formation is desirable
Load distribution, biological healing, lower implant stress
More motion at fracture, potential for delayed union if too flexible
Stiffness is inversely proportional to working length cubed: Doubling the working length reduces stiffness by 8-fold.
Screw Biomechanics
Pullout Strength
Screw pullout strength depends on:
- Thread engagement: Deeper threads = more surface area
- Outer diameter: Larger diameter = more bone engagement
- Bone density: Osteoporotic bone has 50-70% lower pullout strength
- Cortical vs cancellous: Cortical provides majority of holding power
Screw Types and Mechanics
- Mechanism
- Fine threads, cut own path
- Advantage
- Maximum holding in cortical bone
- Disadvantage
- Poor purchase in cancellous bone
- Mechanism
- Coarse threads, self-tapping
- Advantage
- Good purchase in metaphyseal bone
- Disadvantage
- Weaker in pure cortical bone
- Mechanism
- Threads engage plate, fixed angle
- Advantage
- No compression on bone, unicortical OK
- Disadvantage
- Cannot compress fracture, more expensive
- Mechanism
- Gliding hole, compression across fracture
- Advantage
- Absolute stability, interfragmentary compression
- Disadvantage
- Requires precise technique, can overdistract
The Tension Band Principle
The tension band principle converts the tensile (distraction) force on the convex side of an eccentrically loaded bone into compression at the far cortex. An implant (wire, plate or band) placed on the tension side resists distraction; as the bone is loaded, the fragments are driven together on the opposite cortex.
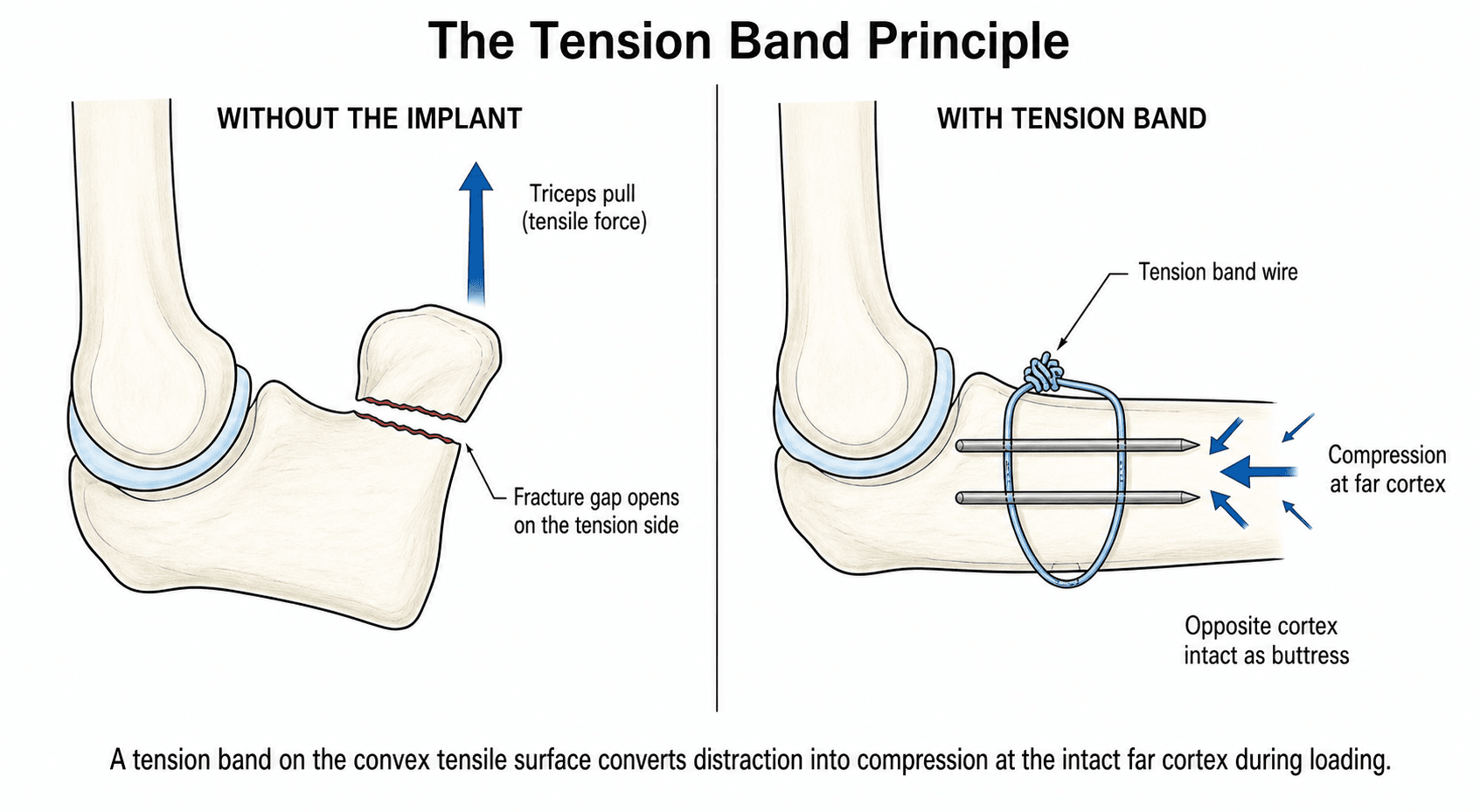
- The implant must lie on the tension (convex) side of the bone.
- There must be an intact cortex opposite the implant to act as a buttress for the compression. If the far cortex is comminuted or deficient, the construct sees bending instead and the tension band fails.
- The bone must be loaded dynamically (typically by active muscle pull) to generate the repeated compressive cycle.
- Olecranon and patella fractures — the triceps/quadriceps pull is the deforming tensile force; a tension band (K-wires plus a figure-of-eight wire) converts it into articular compression with elbow/knee flexion.
- Greater trochanter and medial malleolus avulsions — driven by abductor and deltoid-ligament pull respectively.
- A plate placed on the tension side of a loaded long bone (e.g. the lateral femur) acts as a tension band for the same reason, which is why plate position relative to the tension surface matters.
A tension band only works if the cortex opposite the implant is intact to take the compression. Apply a tension band across a fracture with a comminuted or deficient far cortex and it fails in bending — that situation needs a buttress or a load-bearing construct instead.
Implant Materials and Stiffness
Material Properties That Matter
The elastic (Young's) modulus of an implant determines how much load it carries relative to bone. A stiffer implant shields the bone from stress; a more compliant implant transfers more load to healing bone. Fatigue strength governs how many loading cycles an implant survives before failure - a key consideration in load-bearing constructs spanning a fracture gap.
- Elastic Modulus (GPa)
- 15-20
- Key Property
- Reference value
- Biomechanical Implication
- Implants are far stiffer, driving stress shielding
- Elastic Modulus (GPa)
- 0.1-2
- Key Property
- Highly variable with BMD
- Biomechanical Implication
- Poor screw purchase in metaphysis when osteoporotic
- Elastic Modulus (GPa)
- ~110
- Key Property
- Lower modulus, biocompatible, MRI-friendly
- Biomechanical Implication
- Less stiff than steel, lower stress shielding, notch-sensitive
- Elastic Modulus (GPa)
- ~200-210
- Key Property
- High stiffness and ductility
- Biomechanical Implication
- Stiffer construct, more stress shielding, allows contouring
- Elastic Modulus (GPa)
- ~210-240
- Key Property
- High wear and fatigue resistance
- Biomechanical Implication
- Very stiff; used for bearing surfaces and stems
The order of stiffness is cobalt-chrome greater than stainless steel greater than titanium greater than cortical bone. The larger the modulus mismatch between implant and bone, the greater the stress concentration at the bone-implant interface (e.g. at the last screw hole) and the more stress shielding under the plate.
Clinical Relevance and Applications
Applying Biomechanics to Fixation Decisions
- Simple fractures: Absolute stability via compression plating, lag screws
- Comminuted fractures: Relative stability via bridge plating, nailing
- Articular fractures: Anatomic reduction + absolute stability
- Match implant stiffness to fracture personality
- Longer working length for comminuted patterns (more flexible)
- Bicortical screws for maximum pullout strength
- Locked plates act as internal external fixators
- Stress shielding: Use less rigid constructs when possible
- Implant failure: Ensure adequate working length and screw density
- Refracture after removal: Gradual loading, delay high-impact activities
Guidelines, Registries & Global Practice
Global Epidemiology
- Fractures requiring fixation are among the commonest procedures in orthopaedics worldwide; the global incidence of fragility fractures is rising sharply with population ageing, increasingly shifting fixation challenges into osteoporotic bone.
- Implant-related complications (loss of fixation, nonunion, peri-implant fracture, fatigue failure) are a leading reason for unplanned reoperation after fracture surgery globally.
- Osteoporosis disproportionately affects fixation in older adults and in low- and middle-income settings where bone-protection therapy and implant choice may be limited.
Side-by-Side Guideline Frameworks
- Core Position
- Anatomical reduction, stable fixation matched to pattern, blood-supply preservation, early motion
- Practical Emphasis
- Absolute vs relative stability framework; biological internal fixation
- Core Position
- Standards for open fractures and fragility-fracture care emphasising soft tissues and timely definitive fixation
- Practical Emphasis
- Construct that permits early weight-bearing in the elderly
- Core Position
- Evidence-based clinical practice guidelines (e.g. hip fracture) supporting stable fixation and early mobilisation
- Practical Emphasis
- Implant selection guided by fracture stability and bone quality
- Core Position
- Promotes fragility-fracture networks and fixation strategies tailored to osteoporotic bone
- Practical Emphasis
- Locked/augmented constructs and orthogeriatric co-management
Across frameworks the biomechanical principles are universal - they differ mainly in emphasis on system-level care (open-fracture timing, orthogeriatric pathways) rather than in the underlying mechanics.
Registry Evidence
- Arthroplasty and implant registries - NJR (UK), AJRR (US), AOANJRR (Australia), SHAR (Sweden), the Norwegian and New Zealand registries - track implant survival and revision and have repeatedly shown how design and fixation choices affect longevity. The same registry methodology increasingly captures fracture-fixation devices and peri-implant fractures.
- Registry data reinforce that construct and material choice (e.g. fixation mode, modulus, bearing) measurably influence revision rates over time.
High- vs Limited-Resource Practice Variation
- Well-resourced settings: full range of locking plates, multiple alloys, intraoperative imaging, cement/augmentation and orthogeriatric pathways are available, allowing precise tailoring of stiffness and stability.
- Limited-resource settings: reliance on a narrower implant range, more external fixation and conventional plating, and emphasis on robust, low-cost constructs; sound biomechanical reasoning (working length, screw purchase, load sharing) becomes even more important when implant options are constrained.
Controversies and Areas of Uncertainty
Very stiff bridging constructs can suppress callus and lead to delayed/nonunion (especially distal femur). Strategies to "soften" constructs - far cortical locking, longer working length, titanium plates, fewer screws near the fracture - aim to allow healthy micromotion, but the ideal target stiffness is still debated.
Whether to remove plates after union (to reverse stress shielding and reduce refracture risk) is contested. Removal carries its own risks (refracture through screw holes, neurovascular injury) and is increasingly reserved for symptomatic hardware rather than performed routinely.
Unicortical locked screws reduce dissection but provide less torsional and pullout resistance; the balance between soft-tissue preservation and mechanical security remains case-dependent.
Reamed nailing improves fixation and union in closed fractures but the marginal benefit in open tibial fractures is small; debate continues over the embolic and biological cost of reaming versus the mechanical gain.
MCQ Practice Points
Q: What is the most important factor affecting screw pullout strength? A: Outer thread diameter and depth of engagement. Bicortical purchase increases strength 2-3x compared to unicortical. Bone density is also critical (osteoporotic bone has 50-70% reduced pullout strength).
Q: How does doubling the working length affect construct stiffness? A: Reduces stiffness by 8-fold (stiffness is inversely proportional to working length cubed). Longer working length = more flexible = more callus but higher implant stress.
Q: What percentage of stress is reduced in bone beneath a rigid plate? A: 50-80% stress reduction. This leads to bone resorption (Wolff's Law) and refracture risk if plate removed before remodeling (12-18 months).
Q: What are the four AO principles of fracture fixation? A: FREP: Fracture reduction, Rigid fixation (absolute or relative stability), Early mobilization, Preservation of blood supply.
At a Glance
Fracture fixation biomechanics follows the AO principles (FREP): anatomic or relative Fracture reduction, Rigid fixation appropriate to fracture pattern, Early mobilization, and Preservation of blood supply. Constructs provide either absolute stability (compression plating, lag screws—no interfragmentary motion, direct bone healing) or relative stability (bridge plating, intramedullary nails—controlled micromotion, callus formation). Stress shielding occurs when rigid implants bear 50-80% of load, causing bone resorption per Wolff's Law and risking refracture after implant removal. The working length (distance between nearest screws on each side of fracture) determines construct flexibility—longer working length increases flexibility but also implant stress. Critical geometric relationships include: doubling implant diameter increases bending strength roughly 8-fold (section modulus proportional to diameter³) and bending/torsional rigidity roughly 16-fold (area and polar moment of inertia proportional to diameter⁴). Screw pullout strength depends on thread engagement; bicortical screws are 2-3× stronger than unicortical fixation.
FREPAO Principles of Fracture Fixation
Hook:FREP your fracture: Follow AO principles for successful fixation!
STRIPPEDScrew Failure Modes
Hook:Don't get STRIPPED: Know how screws fail to prevent fixation failure!
STABLEFactors Affecting Fracture Healing with Implants
Hook:Keep it STABLE: Control these factors for optimal fracture healing!



Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A patient returns 2 years after femoral shaft fracture fixation with a plate. X-rays show cortical thinning beneath the plate. Explain the mechanism and management.”
“You are plating a comminuted mid-shaft tibial fracture. Discuss how you would determine the working length of your construct and the biomechanical rationale.”
“An 82-year-old woman has a distal femoral fracture fixed with a non-locking plate. At 6 weeks the screws have pulled out and the construct has collapsed into varus. Explain why this failed and how you would revise it.”
Key Concepts
- Wolff's Law: Bone adapts to stress (increased stress = formation, decreased = resorption)
- Stress shielding: Implant bears load, bone resorbs (50-80% stress reduction)
- Working length: Distance between nearest screws (longer = more flexible)
- Load sharing: Bone and implant share load (vs load bearing: implant carries all)
AO Principles (FREP)
- Fracture reduction: Anatomic (articular) or relative (diaphyseal)
- Rigid fixation: Absolute stability (compression) or relative (bridge plating)
- Early mobilization: Prevent stiffness during healing
- Preservation of blood supply: Minimize stripping, biological fixation
Screw Mechanics
- Pullout strength: Bicortical 2-3x stronger than unicortical
- Diameter effect: Pullout proportional to diameter squared
- Osteoporotic bone: 50-70% reduced holding power
- Failure modes: Pullout (tension), shear, stripping, fatigue
Working Length
- Short working length: Rigid, less callus, higher implant stress
- Long working length: Flexible, more callus, load distribution
- Stiffness inversely proportional to length cubed (2x length = 8x less stiff)
- Optimal: 2-3 screw holes each side for diaphyseal fractures
Implant Properties
- Stainless steel: 210 GPa modulus (10x bone)
- Titanium: 110 GPa modulus (5x bone)
- Cortical bone: 20 GPa modulus
- Elastic mismatch creates stress concentration at interface
Evidence Base and Key Studies
Strain Theory & the Scientific Basis of Biological Internal Fixation
- Interfragmentary strain theory: tissue at the fracture gap can only form if local strain stays below the strain tolerance of that tissue (granulation tissue tolerates high strain, lamellar bone very little)
- Flexible (relative) stability induces callus; rigid fixation of a small gap with even minimal motion produces high strain and impairs direct healing
- The internal fixator splints rather than compresses, preserving periosteal blood supply and enabling minimally invasive percutaneous osteosynthesis (MIPO)
- Bone loss under plates is attributed to stress shielding and necrosis-induced remodelling rather than to plate-bone contact alone
Internal Plate Fixation: Stress Shielding & Cortical Porosis
- Rigid plates cause cortical porosis, delayed bridging and refracture after plate removal
- Histomorphometry showed necrosis predominantly in the periosteal cortex and porosis in the endosteal cortex, with no positive correlation between them
- Evidence favoured stress shielding (not interference with cortical perfusion from plate-bone contact) as the dominant cause of bone loss
- Motivated axially compressible plate designs that reduce stress shielding during remodelling