Intra-articular Elbow Fracture | Bicolumnar Fixation | Early Motion Essential
- Bicolumnar anatomy: Medial and lateral columns form triangular construct
- Dual plate fixation required - single plate inadequate
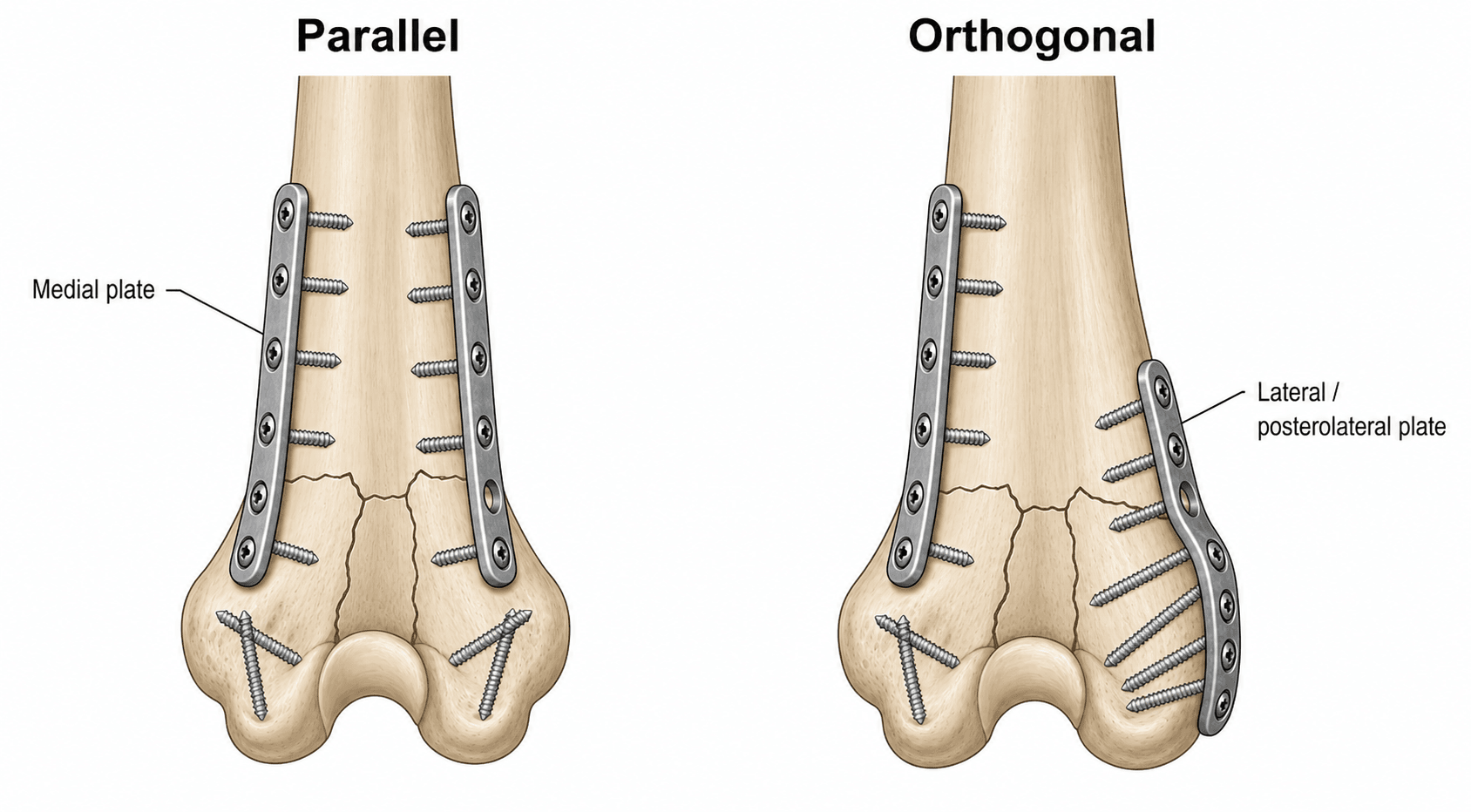
- Orthogonal plating (90°) or parallel plating both effective
- Early motion critical - stiffness is the enemy
- Olecranon osteotomy provides best articular visualization
- “Columns diverge distally to support trochlea and capitellum
- “Articular reconstruction priority before column fixation
- “Ulnar nerve must be identified and protected
- “TEA is reasonable option for elderly with comminution
Distal humerus is a triangle: Two columns (medial and lateral) diverge distally to support the articular surface. Fixation must restore BOTH columns for stability. Single plate fixation will fail.
Identify and protect the ulnar nerve in all cases. Options: in situ, transpose subcutaneously, or transpose submuscularly. Most surgeons transpose to avoid hardware irritation.
Motion is mandatory - elbow stiffness is the most common complication. Start gentle ROM within 1-2 weeks. Stable fixation allows early motion without risking construct.
Dual plate fixation required: Either orthogonal (90°) or parallel plating. Minimum 2-3 screws in each distal fragment. Screws should interdigitate in distal fragments for maximum stability.
- Patient
- Any
- Bone Quality
- Good
- Treatment
- ORIF dual plating
- Patient
- Any
- Bone Quality
- Good
- Treatment
- ORIF dual plating
- Patient
- Young/Active
- Bone Quality
- Good
- Treatment
- ORIF dual plating with articular reconstruction
- Patient
- Elderly/Low demand
- Bone Quality
- Poor
- Treatment
- Consider TEA (total elbow arthroplasty)
- Patient
- Elderly with RA/osteoporosis
- Bone Quality
- Poor
- Treatment
- TEA preferred
Overview
Intercondylar fractures of the distal humerus are complex intra-articular injuries that require anatomic reduction and stable fixation to restore elbow function. These fractures disrupt the bicolumnar architecture of the distal humerus and separate the articular surface from the humeral shaft.
- 2% of all fractures
- 30% of elbow fractures
- Bimodal distribution: Young adults (high energy), Elderly women (low energy)
- Young males: High-energy trauma (MVA, sports)
- Elderly females: Low-energy falls, osteoporosis
- Increasing incidence in elderly population
- Osteoporosis
- High-energy mechanism
- Direct trauma to elbow
- Motor vehicle accidents
- Fall from height
- Sports injuries
- Direct blow to elbow
- Fall onto flexed elbow
- Fall onto outstretched hand with elbow flexed
- Common in osteoporotic elderly
- Olecranon driven into trochlea
- Splits columns apart
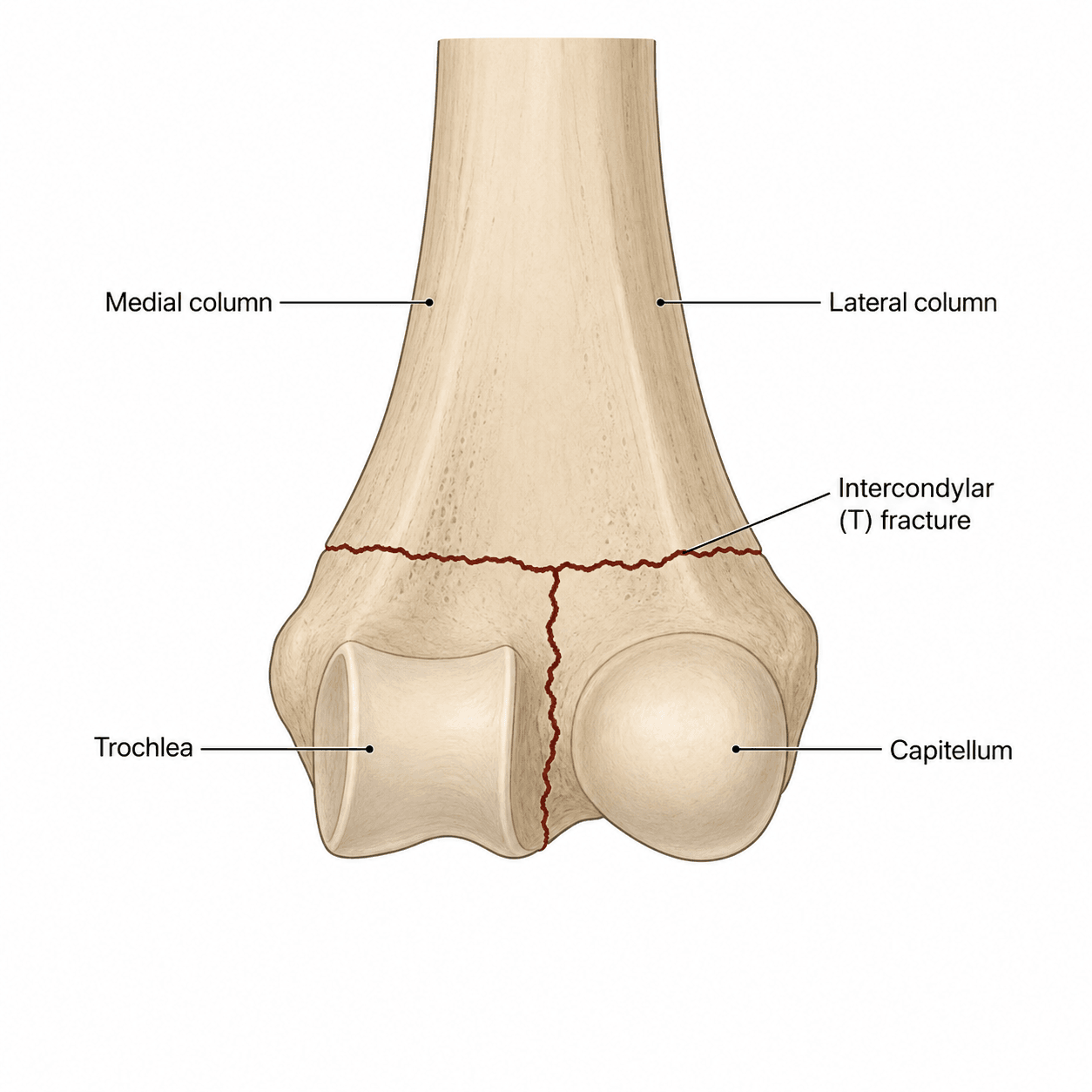
- Creates characteristic T or Y pattern
- Open fractures (15-20%)
- Nerve injuries (ulnar most common)
- Vascular injuries (rare)
Anatomy and Pathophysiology
Bicolumnar Architecture
Understanding the unique triangular architecture of the distal humerus is essential for treating these fractures.
- Two columns diverge distally from humeral shaft
- Forms triangular structure when viewed end-on
- Supports articular surface (trochlea and capitellum)
- Supports the trochlea
- Medial epicondyle is non-articular
- Thicker bone posteriorly and medially
- Best plate position: Posteromedial
- Supports the capitellum
- Lateral epicondyle is non-articular
- Thicker bone posteriorly and laterally
- Best plate position: Posterolateral
- Olecranon fossa (posterior)
- Coronoid fossa (anterior)
- Not suitable for screw placement
The bicolumnar anatomy dictates the dual plating strategy.
The distal humerus resembles a triangle when viewed end-on. The two columns form the sides, and the articular surface (trochlea and capitellum) forms the base. Stable fixation requires restoration of both columns.
COLUMNSDistal Humerus Anatomy
Hook:The COLUMNS support the elbow - remember the bicolumnar anatomy!
Classification
Classification
Bone: 13 (Distal Humerus)
- A1: Avulsion
- A2: Simple metaphyseal
- A3: Multifragmentary metaphyseal
- B1: Sagittal lateral condyle
- B2: Sagittal medial condyle
- B3: Coronal plane (capitellum/trochlea)
- C1: Simple articular, simple metaphyseal
- C2: Simple articular, comminuted metaphyseal
- C3: Comminuted articular
Type C fractures are the focus of intercondylar management.
- Articular
- Simple
- Metaphyseal
- Simple
- Treatment Challenge
- Standard - good prognosis
- Articular
- Simple
- Metaphyseal
- Comminuted
- Treatment Challenge
- Moderate - metaphyseal reconstruction
- Articular
- Comminuted
- Metaphyseal
- Variable
- Treatment Challenge
- Complex - may need TEA in elderly
Clinical Assessment
History and Physical Examination
History
- Fall onto flexed elbow
- Direct blow to elbow
- Motor vehicle accident
- Fall from height
- High energy: MVA, falls from height
- Low energy: Simple falls in elderly
- Severe elbow pain
- Inability to move elbow
- Swelling
- Deformity
- Osteoporosis
- Rheumatoid arthritis (affects treatment choice)
- Previous elbow problems
- Functional demands
Energy level and patient factors guide treatment decisions.
Physical Examination
- Swelling (often marked)
- Deformity
- Ecchymosis
- Skin integrity (open fractures 15-20%)
- Tenderness throughout distal humerus
- Crepitus (avoid excessive manipulation)
- Olecranon prominence preserved (vs dislocation)
- Limited by pain and instability
- Do not force motion
- Document baseline
- Ulnar nerve function (most commonly injured)
- Radial nerve function
- Median nerve function
- Distal pulses and perfusion
Complete neurovascular examination is mandatory before any treatment.
Soft Tissue Assessment
- 15-20% of intercondylar fractures
- Gustilo-Anderson classification
- Urgent debridement required
- Rare but possible
- Assess forearm compartments
- High index of suspicion with high energy
- Posterior skin often compromised
- Fracture blisters common
- May delay surgery
- Often severe
- May need elevation and ice before surgery
- Soft tissue recovery before ORIF
Soft tissue condition may dictate surgical timing.
ALWAYS document ulnar nerve function before any treatment. The ulnar nerve lies posterior to the medial epicondyle and is at risk from both the injury and surgical approach. Pre-operative deficit must be documented.
Differential Diagnosis
- Distinguishing features
- Intra-articular crepitus, gross instability, both columns disrupted
- Key investigation
- AP/lateral X-ray + CT (articular comminution, column split)
- Distinguishing features
- Deformity above joint, articular surface intact
- Key investigation
- X-ray - fracture line proximal to fossae
- Distinguishing features
- Anterior fragment, double-arc sign on lateral, block to flexion
- Key investigation
- Lateral X-ray + CT (coronal plane fragment)
- Distinguishing features
- Partial articular, one column only, may be subtle
- Key investigation
- X-ray +/- CT; stress views
- Distinguishing features
- Loss of olecranon-epicondyle relationship; radial head + coronoid involvement
- Key investigation
- X-ray pre/post reduction + CT
- Distinguishing features
- Posterior tenderness, loss of active extension, palpable gap
- Key investigation
- Lateral X-ray of elbow
- Distinguishing features
- Lateral tenderness, painful rotation, often subtle
- Key investigation
- AP/lateral + radiocapitellar view
Investigations
Imaging Studies
- AP of elbow
- Lateral of elbow
- Oblique views if needed
- Fracture pattern (T, Y, H, Lambda)
- Degree of comminution
- Articular involvement
- Column fractures
- Radial head fracture
- Coronoid fracture
- Olecranon fracture (terrible triad)
- Overlapping fragments obscure detail
- CT often needed for planning
- May underestimate comminution
Plain radiographs provide initial assessment but CT is usually needed.
CT with 3D reconstruction is the gold standard for surgical planning of intercondylar fractures. It reveals articular comminution that may not be apparent on plain radiographs and helps determine if ORIF or TEA is more appropriate.
Management Algorithm
Treatment Decision Making
- Reserved for non-ambulatory patients
- Severe medical comorbidities precluding surgery
- "Bag of bones" technique (historical, poor outcomes)
- Standard of care for displaced fractures
- Options: ORIF or Total Elbow Arthroplasty
- Young/active patients
- Good bone quality
- Reconstructable fracture pattern
- High functional demands
- Elderly low-demand patients
- Severe osteoporosis
- Unreconstructable articular comminution
- Pre-existing arthritis or RA
Most intercondylar fractures require operative treatment.
- Young active patients
- Good bone quality
- Reconstructable pattern
- High demand lifestyle
- ROM: 100-110° arc
- Function: Good to excellent in 75-80%
- Return to activities: Yes
- Elderly (over 65-70)
- Osteoporotic bone
- Severe comminution
- Low demand lifestyle
- ROM: 100-120° arc
- Pain relief: Excellent
- Restrictions: Lifelong 5kg limit
Beyond ORIF and TEA there is a third reconstructive option that examiners increasingly ask about - distal humeral hemiarthroplasty (DHH):
- What it is: replacement of the articular (trochlea/capitellum) surface only with a humeral component, leaving the native ulna and radial head to articulate against it - the columns and collateral ligaments are NOT replaced.
- The niche it fills: the unreconstructable isolated articular fracture (the articular surface is shattered but the columns are intact or fixable and the collateral ligaments are competent) in a patient who is too young/active to accept the TEA lifelong load restriction.
- Prerequisites (the exam discriminators): intact/reconstructable medial and lateral columns (the hemiarthroplasty needs stable columns to anchor to) and competent collateral ligaments and a healthy ulnar/radial articular surface - if these are gone, TEA is the answer instead.
- The key advantage over TEA: no formal lifelong lifting restriction (no linked ulnar component to loosen), making it attractive in the younger-but-unreconstructable patient.
- The caveats: it is technically demanding, the evidence is lower-level than for TEA, and wear of the native ulnar/radial cartilage against the metal hemiarthroplasty is the main long-term concern.
Exam point: DHH is for the isolated unreconstructable articular fracture with intact columns and competent ligaments in an active patient - it avoids the TEA load restriction but depends on healthy columns, ligaments and the opposing native cartilage.
Surgical Technique
Operative Procedures
- Best articular visualization
- Most intercondylar fractures
- Complex articular patterns
- Posterior midline incision
- Identify and mobilize ulnar nerve
- Chevron or transverse osteotomy
- Pre-drill for fixation before osteotomy
- Elevate olecranon with triceps attached
- Direct visualization of trochlea
- Best articular visualization
- Direct access to both columns
- Allows anatomic reduction
- Creates additional fracture
- Risk of nonunion (2-5%)
- Hardware prominence
Olecranon osteotomy provides best visualization for complex fractures.
The olecranon osteotomy provides the best visualization of the articular surface. Use a chevron osteotomy for rotational stability and pre-drill the screw hole before performing the osteotomy to ensure accurate reduction.
Articular Reconstruction
- Identify key articular fragments
- Reduce trochlea first (medial to lateral)
- Provisional K-wire fixation
- Lag screws for articular fragments
- Reduce articular block to medial column
- Reduce articular block to lateral column
- Restore column length and alignment
- Apply first plate (usually medial)
- Apply second plate
- Final tightening
- Check ROM intraoperatively
Sequence: Articular first, then columns, then plates.
PLATESSurgical Principles
Hook:PLATES reminds you of the key surgical principles!
Complications
Potential Complications
- Incidence: 20-40%
- Worse with prolonged immobilization
- Worse with heterotopic ossification
- Early motion (within 1-2 weeks)
- Stable fixation
- Consider indomethacin for HO prophylaxis
- Aggressive physiotherapy
- Dynamic splinting
- Manipulation under anesthesia
- Arthroscopic or open release
- 30-130° arc adequate for most ADLs
- Loss of terminal extension common
- Loss of flexion more functionally limiting
Early motion is the key to preventing stiffness.
Elbow stiffness is the most common complication of intercondylar fractures. Prevention through stable fixation and early motion is essential. Start gentle ROM within 1-2 weeks of surgery.
When TEA is selected for a fracture, examiners expect you to know the implant design and its specific complications - these are what drive the lifelong load restriction:
- Linked (semi-constrained) TEA: the humeral and ulnar components are connected by a sloppy-hinge bushing that allows a few degrees of varus-valgus/rotational laxity. It does not depend on the collateral ligaments or bone columns for stability, so it is the design used for comminuted fractures with deficient columns/ligaments (the usual fracture scenario).
- Unlinked (unconstrained) TEA: the components are not connected and rely on intact bone columns and competent collateral ligaments for stability - rarely suitable for a comminuted fracture, more an arthritis option.
- Failure modes to quote: polyethylene bushing wear and aseptic loosening (the reason for the lifelong ~5 kg lifting restriction - load accelerates wear/loosening), periprosthetic fracture, deep infection (catastrophic, harder to treat than in ORIF), and triceps insufficiency/extensor-mechanism failure from the posterior approach.
- Why fracture-TEA can still be durable: in genuinely low-demand elderly patients who respect the load limit, long-term implant survival is high (most never need revision) - the restriction is precisely what protects the bushing and bone-cement interface.
Exam point: fracture-TEA is a linked (semi-constrained) implant (independent of ligaments/columns); its defining complications are bushing wear, aseptic loosening, periprosthetic fracture, infection and triceps insufficiency, which is why the lifelong load restriction is non-negotiable.
STIFFComplications
Hook:Don't let your patient become STIFF - move them early!
Postoperative Care
Rehabilitation Protocol
- Protect fixation
- Begin early ROM
- Control swelling
- Posterior splint at 90° flexion
- Elevation
- Active finger, wrist, shoulder motion
- Begin active-assisted elbow ROM
- Remove splint for exercises
- Gravity-assisted flexion
- Extension stretching
- Progress ROM exercises
- Active motion all planes
- May use hinged brace for protection
- Continue to avoid loading
Early motion is critical - begin within 1-2 weeks.
Outcomes
Expected Results
- Good to excellent: 75-85%
- Fair: 10-15%
- Poor: 5-10%
- Average arc: 100-110°
- Extension loss: 20-30° common
- Flexion usually 120-130°
- Stiffness: 20-40%
- Ulnar nerve symptoms: 10-20%
- Hardware removal: 15-25%
- Nonunion: 2-10%
- Fracture complexity (C1 better than C3)
- Quality of reduction
- Early motion protocol
- Patient compliance
ORIF outcomes are generally good with proper technique and rehabilitation.
Guidelines, Registries & Global Practice
Global Epidemiology
Distal humeral fractures account for roughly 2% of all fractures and about a third of elbow fractures, with a characteristic bimodal age-sex distribution: high-energy injuries in young men and low-energy fragility fractures in older women. Population-based registry data from Finland show the age-adjusted incidence of osteoporotic distal humeral fractures in women aged 60 and over rising from 12 to 28 per 100,000 between 1970 and 1995, with absolute numbers projected to almost triple by 2030 (Palvanen et al., 1998).
- Figure
- ~2%
- Source / Notes
- Distal humerus, all ages
- Figure
- ~30%
- Source / Notes
- Adult elbow injuries
- Figure
- 28 / 100,000
- Source / Notes
- Palvanen 1998 (Finland, age-adjusted)
- Figure
- Almost x3
- Source / Notes
- Driven by ageing + rising age-specific risk
- Figure
- ~15-20%
- Source / Notes
- Higher in high-energy young cohort
Guideline & Registry Landscape
There is no single dedicated AAOS/NICE/BOA clinical practice guideline specific to intercondylar (OTA 13-C) distal humeral fractures; recommendations are derived from elbow-fracture management literature, the AO Surgery Reference, fragility-fracture pathways and elbow-arthroplasty registries. The table below summarises the practical positions that converge across major bodies.
- Position on intercondylar fractures
- Dual-column fixation; articular reconstruction first; parallel or orthogonal plating; early motion
- Underlying evidence
- Biomechanical + cohort evidence (Sanchez-Sotelo, Schwartz, Arnander)
- Position on intercondylar fractures
- ORIF standard for reconstructable fractures; primary TEA an option for comminuted fractures in low-demand elderly
- Underlying evidence
- Level I RCT (McKee) + meta-analyses
- Position on intercondylar fractures
- Frail/fragility limb fractures: senior decision-making, early surgery and early mobilisation within orthogeriatric pathways
- Underlying evidence
- Fragility-fracture and frailty standards
- Position on intercondylar fractures
- No fracture-specific guideline; covered by falls/fragility-fracture and osteoporosis (NG) guidance plus bone-health assessment
- Underlying evidence
- Fragility-fracture prevention evidence
- Position on intercondylar fractures
- Endorse TEA in selected elderly comminuted fractures; caution re lifelong load limit and revision burden
- Underlying evidence
- RCT + registry/long-term cohort data
Registry Evidence
National joint registries (e.g. the UK NJR elbow dataset, the Australian Orthopaedic Association National Joint Replacement Registry [AOANJRR] and the Norwegian Arthroplasty Register) capture total elbow arthroplasty undertaken for acute fracture and report this as a recognised indication distinct from inflammatory and degenerative arthritis. Registry signals consistently show that fracture is a substantial minority indication for TEA and that revision risk is influenced by patient activity and adherence to load restrictions. Long-term follow-up of the McKee trial cohort found only 1 of 25 fracture-TEA implants required revision at a mean of 12.5 years, supporting durable survivorship in genuinely low-demand patients (Dehghan et al., 2019).
Practice Variation
ORIF remains the default worldwide for reconstructable fractures and for essentially all younger or active patients. Primary TEA is used selectively for comminuted, unreconstructable fractures in low-demand elderly patients; its uptake varies by surgeon elbow-arthroplasty experience and by health-system access to implants and revision services, and complex reconstruction is often concentrated in specialist or metropolitan trauma centres. Distal humeral hemiarthroplasty is offered in some centres for isolated articular destruction in patients considered too young/active for the TEA load restriction, though evidence remains lower-level.
Rehabilitation access is decisive for outcome: supervised early-motion physiotherapy is essential, and some elderly patients, particularly after TEA, benefit from a period of inpatient rehabilitation.
MCQ Practice
High-Yield Exam Facts
Q: Why is dual plate fixation mandatory for intercondylar fractures? A: The distal humerus has a bicolumnar architecture where medial and lateral columns diverge distally to support the articular surface. Both columns must be stabilized for adequate fixation; single plate fixation will fail.
Q: What are the AO/OTA 13-C subtypes and how do they guide treatment? A: C1 (simple articular, simple metaphyseal) - standard ORIF; C2 (simple articular, comminuted metaphyseal) - ORIF with possible bone graft; C3 (comminuted articular) - ORIF in young patients or TEA in elderly. Treatment selection depends on fracture complexity, patient age, and bone quality.
Q: Compare orthogonal vs parallel plating configurations. A: Both are biomechanically equivalent. Orthogonal (90°) positions plates posteromedially and posterolaterally at 90° to each other. Parallel (180°) positions both plates on the posterior surface. Both require minimum 2-3 screws in each distal fragment with interdigitating screws for stability.
Q: When is TEA preferred over ORIF for intercondylar fractures? A: TEA is preferred in elderly patients (over 65-70) with severe osteoporosis and unreconstructable articular comminution (C3 fractures). Level I evidence (McKee 2009) shows better DASH scores and fewer complications than ORIF in this population.
Q: What is the most common complication and how is it prevented? A: Elbow stiffness (20-40% incidence) is most common. Prevention requires stable fixation allowing early motion within 1-2 weeks. The functional ROM arc needed for ADLs is 30-130° (100° total arc). Early aggressive physiotherapy is critical.
Q: How should the ulnar nerve be managed during surgery? A: Ulnar nerve identification is mandatory in all cases - it runs posterior to the medial epicondyle. Most surgeons transpose the nerve (subcutaneously or submuscularly) to prevent late ulnar neuritis from hardware irritation, though in situ management is an option.
Self-Assessment Questions
Question 1: What is the primary reason dual plate fixation is required for intercondylar distal humerus fractures?
- A. To increase stability against rotational forces
- B. Because of the bicolumnar anatomy requiring both columns to be stabilized
- C. To allow placement of more screws
- D. Because single plates are not strong enough
- E. To facilitate hardware removal
Answer: B - The distal humerus has a bicolumnar architecture with medial and lateral columns supporting the articular surface. Both columns must be stabilized for adequate fixation, requiring dual plates.
Question 2: Which surgical approach provides the best visualization of the articular surface in intercondylar fractures?
- A. Medial approach
- B. Lateral approach
- C. Olecranon osteotomy
- D. Bryan-Morrey approach
- E. Paratricipital approach
Answer: C - The olecranon osteotomy provides the best direct visualization of the articular surface (trochlea), allowing anatomic reduction of complex articular fractures.
Question 3: What is the most common complication following ORIF of intercondylar fractures?
- A. Infection
- B. Nonunion
- C. Stiffness
- D. Ulnar nerve injury
- E. Hardware failure
Answer: C - Elbow stiffness is the most common complication, occurring in 20-40% of cases. Prevention through early motion is essential.
Question 4: In which patient would TEA be preferred over ORIF for an intercondylar fracture?
- A. 35-year-old manual laborer with C1 fracture
- B. 80-year-old with RA and C3 fracture with severe comminution
- C. 50-year-old with C2 fracture
- D. 25-year-old athlete with C3 fracture
- E. 60-year-old with C1 fracture and good bone quality
Answer: B - TEA is appropriate for elderly, low-demand patients with osteoporosis or RA and unreconstructable articular comminution (C3). Young active patients should have ORIF attempted regardless of complexity.
Question 5: When performing dual plating, what is the recommended minimum number of screws in each distal fragment?
- A. 1
- B. 2-3
- C. 4-5
- D. 6
- E. As many as possible
Answer: B - A minimum of 2-3 screws in each distal fragment is recommended. Screws should interdigitate between the two plates for maximum stability.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old man sustains an AO 13-C2 intercondylar distal humerus fracture in a motorcycle accident. Describe your management.”
“A 78-year-old active female presents after a fall with a comminuted intra-articular distal humerus fracture (AO type 13-C3). She has osteoporosis but lives independently. How do you manage this?”
“At your post-operative review 6 weeks after ORIF, your patient has only 30-100 degrees of motion (70 degree arc). What is your approach?”
“Describe the bicolumnar anatomy of the distal humerus and how this guides your fixation strategy.”
Classification (AO 13-C)
- 13-C1: Simple articular, Simple metaphyseal
- 13-C2: Simple articular, Comminuted metaphyseal
- 13-C3: Comminuted articular/metaphyseal
- Frequency: C3 (comminuted) most common
- High T vs Low T patterns
Key Concepts
- Bicolumnar Anatomy (Structure)
- Tie Arch Concept (Articular Block)
- Dual Plating Mandatory
- Orthogonal (90°) or Parallel (180°)
- Early Motion is Critical
Treatment Priorities
- Young/Active: ORIF (Dual Plate)
- Elderly/C3: TEA (Arthoplasty)
- Approach: Olecranon Osteotomy (Best view)
- Ulnar Nerve: Transpose or Protect
- Reduction: Articular first then Columns
Complications & Pitfalls
- Stiffness (Most common 20-40%)
- Ulnar Nerve Neuropathy (15%)
- Non-union/Malunion (5-10%)
- HO (Heterotopic Ossification)
- Hardware Failure/Prominence
Evidence Base
Key Studies
McKee et al. - ORIF vs TEA in the Elderly (Multicentre RCT)
- Multicentre RCT of 42 patients over 65 with OTA 13-C distal humeral fractures (15 ORIF, 25 TEA after intention-to-treat)
- 5 of 21 (25%) randomised to ORIF were converted to TEA intra-operatively because stable fixation could not be achieved
- TEA gave significantly better Mayo Elbow Performance Scores at 3, 6, 12 and 24 months (86 vs 73 at 2 years, p=0.015)
- DASH favoured TEA in the short term but was not significantly different at 2 years; reoperation rates (12% TEA vs 27% ORIF) did not differ statistically
Schwartz et al. - Parallel vs Perpendicular Plating (Biomechanical)
- Bicolumnar intra-articular fractures created in 10 composite humeri, randomised to parallel or perpendicular plating
- No statistically significant difference in construct stiffness in any loading direction (flexion, extension, varus, valgus, axial, torsion)
- Plate-strain patterns differed (90° lower longitudinal strain in axial compression; 180° lower transverse strain in torsion)
- Authors conclude surgeon experience and preference may dictate plate construct choice
Sanchez-Sotelo et al. - Principle-Based Parallel-Plate ORIF
- 34 consecutive complex distal humeral fractures (26 type C3, 14 open) fixed with two parallel plates in the sagittal plane
- Primary union in 31 of 32 fractures followed; no hardware failure or fracture displacement
- Mean flexion-extension arc 99°; mean Mayo Elbow Performance Score 85 (excellent/good in 27 of 32)
- Technique maximises distal articular fixation and supracondylar stability to permit intensive early rehabilitation
Ring et al. - Olecranon Osteotomy for Distal Humeral Exposure
- 45 consecutive apex-distal chevron olecranon osteotomies (16 fractures, 29 nonunions) repaired with K-wires and figure-of-eight tension wires
- 44 of 45 osteotomies (98%) healed within 6 months; one early failure from premature loading required ulnar plating
- 12 of 45 (27%) had wire removal, but only 6 (13%) for symptoms directly related to the wires
- Demonstrates that osteotomy complications are low when a precise apex-distal chevron technique is used
Githens et al. - ORIF vs TEA Systematic Review & Meta-Analysis
- Systematic review and meta-analysis of geriatric distal humeral fractures treated with locked-plate ORIF or primary TEA
- TEA and ORIF produced similar functional outcome scores and range of motion
- A non-significant trend toward higher major complication and reoperation rates was seen after ORIF
- Methodological quality of included studies was generally weak; prospective and cost data were called for
Dehghan & McKee et al. - Long-Term TEA Implant Survival
- Long-term follow-up (mean 12.5 years in survivors) of the original McKee RCT cohort (25 TEA, 15 ORIF)
- Only 1 of 25 TEA patients required revision arthroplasty (an early revision); no late revisions occurred
- 15 patients died with a well-functioning implant in situ and 7 retained their original implant
- Confirms durable long-term implant survival of TEA for fracture in elderly patients
Palvanen et al. - Epidemiology of Distal Humeral Fractures
- Population-based Finnish registry analysis of osteoporotic distal humeral fractures in women aged 60 and over, 1970-1995
- Age-adjusted incidence rose from 12 to 28 per 100,000 women over the study period
- Increase exceeded that explained by demographic change alone, implying a true rising age-specific risk
- Projected an almost three-fold increase in absolute fracture numbers by 2030