Benign Myxoid Soft-Tissue Tumour | GNAS-Driven | Classic Sarcoma Mimic
- Intramuscular myxoma is benign - it never metastasises and almost never recurs after marginal excision
- It is a classic sarcoma mimic: hypercellular foci can be mistaken for myxofibrosarcoma or low-grade fibromyxoid sarcoma
- Activating GNAS mutation (R201) is the molecular driver, shared with fibrous dysplasia
- Mazabraud syndrome = intramuscular myxoma plus fibrous dysplasia of bone
- MRI shows a fluid-like mass (low T1, very high T2) with a peritumoral fat rind and surrounding muscle oedema
- “A deep, fluid-bright intramuscular mass that is NOT a simple cyst should raise myxoma versus myxoid sarcoma
- “The peritumoral fat rind and bright peripheral muscle oedema are characteristic MRI clues
- “GNAS mutation supports myxoma over a myxoid sarcoma when the biopsy is small
- “Always image and ask about bone lesions - do not miss Mazabraud syndrome
- “Core needle or open biopsy first; marginal (not wide) excision is sufficient once benign
Benign with essentially zero metastatic potential, yet it is one of the great sarcoma mimics. Hypercellular and hypervascular foci can be misread as myxofibrosarcoma or low-grade fibromyxoid sarcoma. Knowing the bland cytology and lack of mitoses/necrosis prevents over-treatment.
Activating GNAS mutation (codon R201) underlies most intramuscular myxomas - the same gene mutated in fibrous dysplasia. A detectable GNAS mutation on a small biopsy supports myxoma over a myxoid sarcoma.
Fluid-like mass plus extra clues: low T1, very high T2 signal, a thin peritumoral fat rind, and bright muscle oedema at the periphery. These features raise myxoma but never exclude a myxoid sarcoma - biopsy is still required.
Intramuscular myxoma plus fibrous dysplasia of bone = Mazabraud syndrome. Always review the bones on imaging and ask about previous fractures or deformity. Multiple myxomas in particular should trigger a search for bone disease.
MAZAMazabraud Syndrome
Hook:MAZA = Myxoma And fibrous dysplasiA - two GNAS-driven lesions in one patient.
Overview and Epidemiology
Intramuscular myxoma is a benign soft-tissue tumour that arises deep within skeletal muscle and is composed of bland spindle and stellate cells set in an abundant, mucoid (myxoid) matrix. It is important out of proportion to its rarity for two reasons: it is a classic mimic of myxoid sarcomas on both imaging and small biopsies, and it is the soft-tissue half of Mazabraud syndrome. Getting the diagnosis right prevents a benign lesion being treated as a sarcoma.
According to PubMed, the largest classic series of 51 cases found a clear female predominance (35 women, 16 men), a mean age of 52 years, and tumours ranging from 2 to 15 cm (average 5.6 cm); crucially, no tumour recurred or metastasised on follow-up (Nielsen et al., Am J Surg Pathol 1998; DOI). A surgical series of 17 patients reported a similar profile - mean age 55 years, female predominance, the great majority in the thigh - and again no recurrences after marginal excision over a mean 7-year follow-up (Silver et al., Clin Orthop Relat Res 2002, PMID 12360026).
Typical patient and site: a middle-aged adult (peak fifth to sixth decade), more often female, presenting with a slowly enlarging, deep, painless mass. The thigh is the single most common location, followed by the buttock/gluteal region, shoulder and upper arm. A deep myxoid mass in a young child or a superficial myxoid mass should prompt you to reconsider the diagnosis.
- Age: Peak fifth to sixth decade (mean ~52-55 years)
- Gender: Female predominance (roughly 2:1 in large series)
- Growth: Slow, often present for months to years
- Symptoms: Usually painless; aching/pain in a minority
- Thigh: Most common single site (quadriceps, adductors)
- Buttock / gluteal: Second most common
- Shoulder / upper arm: Frequent in upper limb
- Calf and other large muscles: Less common
Pathophysiology and Genetics
The GNAS - cAMP Pathway
Intramuscular myxoma and fibrous dysplasia are united by the same molecular driver: an activating, post-zygotic (somatic) mutation in GNAS, most often at codon R201 (for example p.R201C and p.R201H). GNAS encodes the alpha subunit of the stimulatory G protein (Gs-alpha). The mutation locks Gs-alpha in its active state, constitutively driving adenylate cyclase and raising intracellular cyclic AMP, which in turn alters proliferation and differentiation of the affected mesenchymal cells.
Because the mutation occurs after fertilisation, it produces a mosaic distribution. If it arises early and involves skeletal precursors, the result is fibrous dysplasia (and, when extensive with endocrine features, McCune-Albright syndrome); when it also affects intramuscular mesenchymal cells, intramuscular myxoma can develop. The coexistence of intramuscular myxoma and fibrous dysplasia - Mazabraud syndrome - is the clinical expression of this shared mutation in two tissues.
Activating GNAS Mutation
Key facts:
- Gene: GNAS (encodes Gs-alpha), chromosome 20q13
- Hotspot: codon R201 (p.R201C, p.R201H most common; rarer R201S/L/P and Q227 variants reported)
- Effect: constitutive Gs-alpha activation, raised cyclic AMP
- Inheritance: somatic, post-zygotic - not inherited, mosaic distribution
According to PubMed, sensitive sequencing detects GNAS mutations in a majority of intramuscular myxomas: a next-generation sequencing study combining two assays found mutations in 68% of sporadic myxomas (Bekers et al., Diagn Pathol 2019; DOI), and a COLD-PCR study raised detection from 29% with conventional PCR to 61% with the more sensitive method (Delaney et al., Mod Pathol 2009; DOI).
Pathology and Histology
Macroscopic Features
- Appearance: well-circumscribed but unencapsulated, glistening, gelatinous, lobulated cut surface
- Consistency: soft, mucoid; may have small cystic spaces
- Margin: blends into surrounding muscle at the edge despite looking discrete
- Size: commonly 2 to 15 cm (average around 5 to 6 cm)
Microscopic Features
- Hypocellular: few, widely spaced cells
- Hypovascular: scant, inconspicuous vessels
- Cells: bland spindle and stellate fibroblast-like cells
- Stroma: abundant pale myxoid (mucoid) matrix
- No atypia, no mitoses, no necrosis
- Focal areas of increased cellularity and vascularity
- More collagen; can occupy a large part of the tumour
- Still bland - no significant atypia, mitoses or necrosis
- The main reason myxoma is misdiagnosed as sarcoma
According to PubMed, in the classic 51-case series 38 of 51 tumours contained hypercellular regions occupying 10 to 80% of the lesion, yet none showed cytologic atypia, mitotic activity or necrosis, and none recurred or metastasised - recognising these foci is essential to avoid an erroneous diagnosis of sarcoma (Nielsen et al., Am J Surg Pathol 1998; DOI).
Immunohistochemistry
Intramuscular myxoma has no single specific stain; immunohistochemistry is used mainly to exclude mimics. The lesional cells are typically positive for vimentin and variably for smooth muscle actin (reflecting fibroblastic/myofibroblastic differentiation) and are negative for S100, desmin and CD34.
- Intramuscular Myxoma
- Positive
- Why It Helps
- Confirms mesenchymal origin (non-specific)
- Intramuscular Myxoma
- Variable / focally positive
- Why It Helps
- Reflects myofibroblastic differentiation
- Intramuscular Myxoma
- Negative
- Why It Helps
- Helps exclude myxoid liposarcoma and nerve sheath tumour
- Intramuscular Myxoma
- Negative
- Why It Helps
- Positive in low-grade fibromyxoid sarcoma - a key discriminator
- Intramuscular Myxoma
- Present in majority
- Why It Helps
- Absent in the malignant myxoid mimics
Do not let a hypercellular focus turn a benign myxoma into a sarcoma diagnosis. The constant features of intramuscular myxoma - bland cytology, no mitoses, no necrosis, and a hypovascular myxoid background - are preserved even where cellularity rises. Atypia, frequent mitoses, necrosis or arborising/plexiform capillaries should make you actively look for a myxoid sarcoma instead.
Classification and Differential Diagnosis
There is no formal grading system because intramuscular myxoma is benign. The clinically useful "classification" is contextual - solitary versus multiple, and sporadic versus Mazabraud-associated - and, on histology, classic versus cellular variant. The exam-critical task is the differential diagnosis against myxoid sarcomas.
Benign Lesions to Distinguish
- Clues That It Is NOT Myxoma
- True cyst, thin wall, juxta-articular, no solid enhancement
- Clues That It Is NOT Myxoma
- Rapid growth over weeks, 'tissue-culture' fibroblasts, USP6 rearrangement
- Clues That It Is NOT Myxoma
- S100 positive, relation to a nerve, target sign on MRI
- Clues That It Is NOT Myxoma
- Near a large joint (especially knee), often cystic, may recur locally
When a small myxoid biopsy is hard to call: MUC4 positivity points to low-grade fibromyxoid sarcoma, S100 with chicken-wire vessels and lipoblasts points to myxoid liposarcoma, and a detectable GNAS mutation supports intramuscular myxoma. Atypia, mitoses, necrosis and prominent arborising vasculature all favour a sarcoma over myxoma.
MYXOIDThe Myxoid Soft-Tissue Differential
Hook:Run MYXOID through every fluid-bright deep mass before you commit to a diagnosis.
Juxta-Articular Myxoma: the Other Benign Myxoma
The topic lists juxta-articular myxoma in the benign differential ("near a large joint, especially the knee, often cystic, may recur locally") and notes that the WHO classification places it in the same myxoma group, but never develops it. It is worth knowing because it is a benign myxoma that behaves differently from the intramuscular type and is a favourite "compare and contrast" question.
- Site and association. It arises in the soft tissue immediately around a large joint - most often the knee, and less commonly the shoulder, elbow, hip or ankle. Unlike intramuscular myxoma it is strongly associated with internal joint derangement / degenerative joint disease and is thought to be related to ganglion/meniscal-cyst-type mechanisms, so it often looks cystic and communicates with, or lies adjacent to, the joint.
- Different molecular biology. Whereas intramuscular myxoma is GNAS-driven, juxta-articular myxoma is generally GNAS-negative and is not part of the Mazabraud/fibrous-dysplasia spectrum - a useful discriminator when the two are considered together.
- The key clinical difference - local recurrence. Both are benign and neither metastasises, but the juxta-articular myxoma has a substantially higher local recurrence rate (roughly a third of cases), in contrast to the near-zero recurrence of intramuscular myxoma. Its cystic, para-articular, infiltrative-edged nature makes complete excision harder, so it needs more careful, complete local excision and follow-up.
- Histology overlaps. The microscopic appearance (bland cells in myxoid stroma) overlaps with intramuscular myxoma, but ganglion-like cystic spaces and a juxta-articular location point to the diagnosis; it must still be separated from myxoid sarcomas on the same principles.
Q: How does juxta-articular myxoma differ from intramuscular myxoma? A: Same benign, non-metastasising, bland-myxoid biology, but juxta-articular myxoma sits next to a large joint (classically the knee), is associated with internal derangement/degenerative disease and ganglion-cyst-type mechanisms, is usually cystic, is GNAS-NEGATIVE (not Mazabraud-related), and - the key point - recurs locally in about a third of cases (versus the near-zero recurrence of intramuscular myxoma), so it needs complete excision and follow-up.
MYXOMAIntramuscular Myxoma Key Features
Hook:MYXOMA - a fluid-bright Muscle mass that Yields to excision but tempts you to overcall sarcoma.
Deep ('Aggressive') Angiomyxoma: the Locally Aggressive Myxoid Mimic
The MYXOID differential mnemonic names "deep ('aggressive') angiomyxoma - pelvic/perineal women, infiltrative, locally recurrent" but the entity is never developed. It is the myxoid tumour most likely to be confused clinically with a deep myxoma yet behaves very differently, so it is a high-yield contrast.
- A different patient and site. Deep (aggressive) angiomyxoma is a rare myxoid tumour of the pelviperineal and inguinoscrotal soft tissues, overwhelmingly in adult women (though it occurs in men), typically presenting as a slowly growing, deep, painless mass that can be mistaken for a Bartholin cyst, hernia or abscess - a very different location and demographic from thigh intramuscular myxoma.
- "Aggressive" means locally infiltrative, not malignant. It does not (or very rarely) metastasises, but it is deeply infiltrative with finger-like extensions into the pelvic floor and perineum, which is why it has a high local recurrence rate (of the order of a third or more) and can be difficult to excise completely.
- Distinct biology - hormone-responsive. It is characteristically oestrogen- and progesterone-receptor positive and harbours HMGA2 (chromosome 12q) rearrangements, unlike GNAS-driven intramuscular myxoma. Its hormone sensitivity means GnRH agonists (e.g. leuprolide) can shrink the tumour and are used as an adjunct or to downsize before surgery - a treatment lever that has no equivalent in intramuscular myxoma.
- Imaging and management contrast. MRI shows a T2-hyperintense mass often with a characteristic "swirled" or layered internal pattern and infiltrative margins. Management is complete (often wide) local excision - deliberately more aggressive than the marginal excision that cures an intramuscular myxoma - with hormonal therapy in selected cases and long-term surveillance for recurrence.
Q: How does deep (aggressive) angiomyxoma differ from intramuscular myxoma, and why does it matter? A: It is a pelviperineal/inguinoscrotal tumour of adult women, is ER/PR-positive with HMGA2 rearrangement (not GNAS), and although it essentially never metastasises it is deeply infiltrative with a high local recurrence rate (~a third or more). Consequently it needs complete/wide local excision (not marginal), can be downsized with GnRH agonists, and requires long-term surveillance - the opposite of the reassuringly marginal, GNAS-driven intramuscular myxoma.
Clinical Presentation
Most patients present with a slowly growing, deep, painless mass, often in the thigh, that has been noticed for months. Because the lesion is intramuscular it tends to be firm, fixed to muscle and only mobile in the plane perpendicular to the muscle fibres. Pain or aching occurs in a minority and may reflect size or local pressure rather than aggressive behaviour. There are no overlying skin changes, no regional lymphadenopathy and no systemic ("B") symptoms.
- Slow, painless enlargement over months to years
- Usually a single mass (multiple suggests Mazabraud)
- Ask specifically about bone pain, fractures, deformity
- No constitutional symptoms
- Deep, firm, smooth mass within a muscle belly
- Non-tender in most patients
- Fixed to muscle; mobile across, not along, fibres
- No skin change, no nodes - reassuring but not diagnostic
A deep, enlarging soft-tissue mass - especially if larger than about 5 cm - must be worked up as a possible sarcoma: MRI first, then image-guided biopsy through a planned approach, ideally after discussion with a sarcoma unit. Do not perform an unplanned "shell-out" excision of an undiagnosed deep mass; if it were a sarcoma, contaminated planes would compromise later limb-sparing surgery.
Investigations and Imaging
Magnetic Resonance Imaging (Investigation of Choice)
MRI is the key imaging study. Intramuscular myxoma behaves like a fluid-containing mass because of its watery myxoid matrix, but several extra features help suggest the diagnosis pre-biopsy.
Core Signal Pattern
- T1-weighted: homogeneous low signal (close to or below muscle)
- T2-weighted / fluid-sensitive: very high, fluid-like signal
- Generally well-defined, oval, intramuscular
According to PubMed, in a series of 20 myxomas the lesions were low signal on T1 in 95% and high signal on T2/fluid-sensitive sequences in 100%, with a mean size of 6.9 cm (Bancroft et al., AJR Am J Roentgenol 2002; DOI).
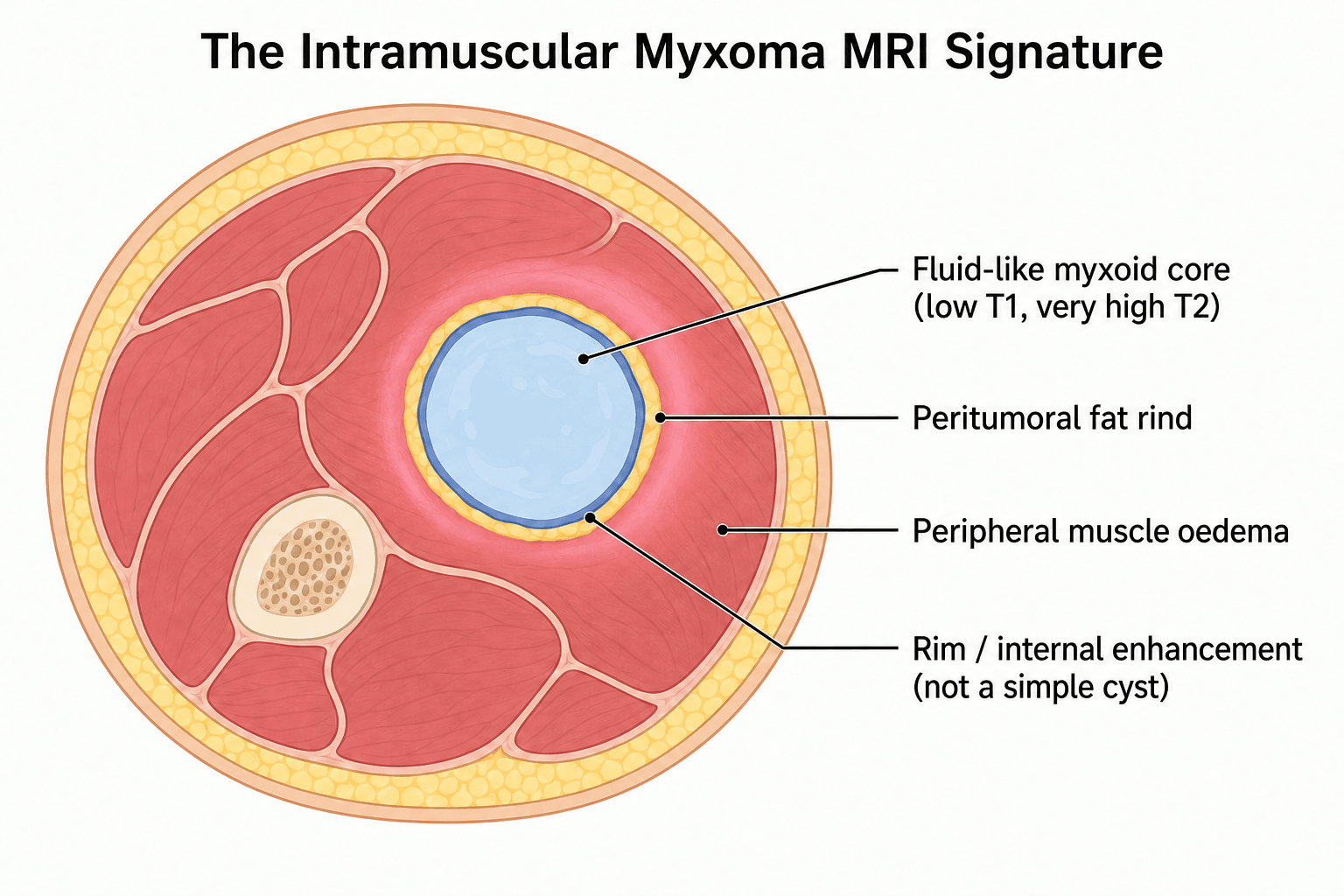
Think intramuscular myxoma when you see:
- A deep intramuscular mass with fluid-like signal (low T1, very high T2)
- A thin peritumoral fat rind
- Bright peripheral muscle oedema on fluid-sensitive sequences
- Internal enhancement (so it is not a simple cyst)
These features raise myxoma but do not exclude a myxoid sarcoma - biopsy is still needed.
Other Modalities and Whole-Patient Assessment
- Ultrasound: a hypoechoic, sometimes cystic-appearing mass; can guide biopsy but cannot define extent or exclude malignancy
- Plain radiographs / CT: usually unremarkable for the soft-tissue mass itself, but invaluable for detecting the fibrous dysplasia of Mazabraud syndrome (ground-glass, expansile bone lesions)
- Look at the bones: when imaging an intramuscular myxoma, deliberately review any visualised bone and consider dedicated skeletal imaging if there is a history of fracture, deformity or multiple myxomas
Biopsy
A tissue diagnosis is mandatory before definitive treatment, because imaging cannot reliably separate myxoma from myxoid sarcoma.
- Image-guided core needle biopsy is preferred; send adequate cores
- Fine-needle aspiration is unreliable here - in a surgical series it matched the final diagnosis in only 3 of 8 aspirated masses (Silver et al., Clin Orthop Relat Res 2002, PMID 12360026)
- Place the biopsy tract so it can be excised with the specimen if malignancy is later confirmed
- Request GNAS analysis when the distinction from a low-grade myxoid sarcoma is difficult
Plan the biopsy as if it might be a sarcoma:
- Use a longitudinal, limb-sparing tract aligned with the definitive incision
- Avoid crossing uninvolved compartments or neurovascular bundles
- Discuss difficult or large deep masses with a sarcoma multidisciplinary team before biopsy
- Never enucleate an undiagnosed deep mass
Management
The management of a confirmed intramuscular myxoma is reassuringly simple, but the path to that confirmation must respect sarcoma principles. Once the diagnosis is secure, treatment is conservative surgery; there is no role for chemotherapy or radiotherapy for the myxoma itself.
Surgical Treatment
- Marginal excision is the treatment of choice and is curative. Wide margins are unnecessary for a benign tumour.
- Function-preserving surgery is appropriate; there is no need to sacrifice nerve, vessel or critical muscle for clearance.
- Recurrence is exceptional, even after incomplete or marginal resection.
According to PubMed, recurrence even after incomplete resection is exceptional and surgical excision is virtually always curative (Nielsen et al., Am J Surg Pathol 1998; DOI), and a 17-patient surgical series treated all tumours by marginal excision with no recurrences over a mean 7-year follow-up (Silver et al., Clin Orthop Relat Res 2002, PMID 12360026).
Managing the Mazabraud Patient
When intramuscular myxoma occurs with fibrous dysplasia, the myxoma is managed as above (marginal excision when indicated), while the bone disease is managed on its own merits - bisphosphonates for pain, prophylactic fixation or correction of deformity for structural bone, and surveillance because the dysplastic bone, not the myxoma, drives most morbidity. There is no convincing evidence that the myxomas of Mazabraud syndrome are more aggressive than sporadic myxomas, although they are more often multiple.
Complications and Prognosis
Prognosis
The prognosis is excellent. Intramuscular myxoma does not metastasise, and local recurrence after marginal excision is rare to non-existent in the major series. The principal "complications" relate to diagnostic error and to the associated conditions rather than to the tumour itself.
- Frequency / Impact
- Leads to unnecessary wide resection / adjuvant therapy
- How to Avoid
- Recognise bland histology, cellular variant; use MUC4/S100/GNAS
- Frequency / Impact
- Untreated bone disease, fracture, deformity
- How to Avoid
- Review bones on imaging; ask about fractures; image skeleton if multiple myxomas
- Frequency / Impact
- Exceptional after marginal excision
- How to Avoid
- Complete (even if marginal) removal; reassure patient
- Frequency / Impact
- Compromises limb-sparing surgery if truly a sarcoma
- How to Avoid
- Biopsy first; treat deep masses as sarcoma until proven benign
A correctly diagnosed intramuscular myxoma is cured by marginal excision with a recurrence risk that is, in practical terms, negligible and zero metastatic potential. The only things that hurt the patient are an incorrect sarcoma diagnosis or a missed bone disease.
Guidelines, Registries & Global Practice
Global Epidemiology
Intramuscular myxoma is a rare benign soft-tissue tumour. Pooled clinicopathologic and surgical series consistently describe a middle-aged patient (mean age in the mid-50s to early 60s), a female predominance of roughly 2:1, and a strong predilection for the thigh and other large proximal muscles. According to PubMed, across the major series tumours average around 5 to 7 cm and behave benignly, with no metastases and exceptional recurrence after marginal excision (Nielsen et al., Am J Surg Pathol 1998; DOI; Silver et al., Clin Orthop Relat Res 2002, PMID 12360026).
Principles That Cross All Jurisdictions
Soft-tissue mass guidance worldwide (for example BSG/BOA and ESMO-EURACAN soft-tissue tumour pathways, and equivalent sarcoma-unit referral standards) converges on the same principles relevant to intramuscular myxoma, even though no guideline is specific to this benign tumour.
- What It Means for Intramuscular Myxoma
- Deep mass over ~5 cm or any diagnostic doubt goes to specialist MDT
- Why
- Myxoma is a sarcoma mimic; getting it wrong harms the patient
- What It Means for Intramuscular Myxoma
- Whole-compartment contrast MRI characterises the mass and plans surgery
- Why
- Defines extent and raises (not confirms) the diagnosis
- What It Means for Intramuscular Myxoma
- Core (not FNA), tract aligned with definitive incision
- Why
- Tissue diagnosis is mandatory; FNA is unreliable here
- What It Means for Intramuscular Myxoma
- MUC4, S100 and GNAS analysis resolve difficult myxoid biopsies
- Why
- Mimics are GNAS-negative; MUC4 marks LGFMS
- What It Means for Intramuscular Myxoma
- Marginal, function-preserving excision; no adjuvant therapy
- Why
- Benign tumour - wide margins are unnecessary
Classification Context
The current WHO Classification of Soft Tissue and Bone Tumours lists intramuscular myxoma among benign tumours of uncertain differentiation (the myxoma group, alongside juxta-articular myxoma), reflecting both its benign behaviour and its GNAS-driven biology shared with fibrous dysplasia. Because it is benign and does not metastasise, it is not staged with the Enneking or AJCC soft-tissue sarcoma systems; those staging frameworks are reserved for the malignant myxoid tumours in its differential. This distinction - a benign WHO category and no malignant staging - is itself an exam point.
Practice Variation
Across health systems the workflow is essentially uniform: MRI, planned core biopsy, specialist review of any indeterminate myxoid lesion, and marginal excision for confirmed myxoma. Differences are largely in access to molecular testing (GNAS sequencing is more readily available in tertiary and reference laboratories) rather than in principles. Internationally, suspected deep soft-tissue masses are referred to specialist sarcoma services, with MRI and image-guided biopsy arranged through or in conjunction with the sarcoma multidisciplinary team; GNAS and other molecular studies are available through specialist anatomical pathology and molecular laboratories, typically at reference centres. An early case report contributed to recognition of the soft-tissue-plus-bone association that defines Mazabraud syndrome (Gianoutsos et al., Aust N Z J Surg 1990; DOI).
- Obtain a tissue diagnosis (core/open biopsy) before any definitive surgery on a deep mass
- Plan the biopsy tract so it can be excised if malignancy is later confirmed
- Discuss indeterminate myxoid lesions at a sarcoma MDT and record the decision
- Document the search for fibrous dysplasia / Mazabraud syndrome, especially with multiple myxomas
- Unplanned excision of an undiagnosed deep mass
- Over-treating a benign myxoma as a sarcoma
- Missing associated fibrous dysplasia and its complications
MCQ Practice Points
Q: What is the characteristic molecular abnormality in intramuscular myxoma? A: An activating, post-zygotic GNAS mutation (codon R201) - the same gene mutated in fibrous dysplasia. According to PubMed it is detectable in the majority of myxomas with sensitive assays (around 68% with combined next-generation sequencing), and it is absent in the malignant myxoid mimics, making it a useful diagnostic discriminator (Bekers et al., Diagn Pathol 2019; DOI).
Q: Why is intramuscular myxoma misdiagnosed as sarcoma? A: Because of its cellular and hypervascular variant. Focal hypercellularity and increased vascularity mimic myxofibrosarcoma, low-grade fibromyxoid sarcoma or myxoid liposarcoma, but the cells remain bland with no mitoses and no necrosis (Nielsen et al., Am J Surg Pathol 1998; DOI).
Q: Which MRI features suggest intramuscular myxoma rather than a simple cyst? A: A peritumoral fat rind and peripheral muscle oedema combined with internal enhancement on a fluid-like (low T1, very high T2) mass. The fat rind is present in roughly two-thirds and adjacent muscle signal in about half of cases (Bancroft et al., AJR 2002; DOI).
Q: What is the treatment and prognosis of a confirmed intramuscular myxoma? A: Marginal excision is curative with negligible recurrence and zero metastatic potential; no radiotherapy or chemotherapy is needed. A surgical series treated all tumours by marginal excision with no recurrences over a mean 7-year follow-up (Silver et al., Clin Orthop Relat Res 2002, PMID 12360026).
Q: What defines Mazabraud syndrome? A: The coexistence of intramuscular myxoma (often multiple) and fibrous dysplasia of bone, both driven by the same GNAS mutation (Wirth, Orthopade 2020; DOI).
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 56-year-old woman presents with a slowly enlarging, painless, deep mass in the right anterior thigh, present for about a year. It is firm, fixed to muscle and roughly 6 cm. How do you investigate and manage her?”
“The pathologist reports a hypocellular myxoid lesion with focal hypercellular and more vascular areas, and is uncertain between intramuscular myxoma and a low-grade myxoid sarcoma. How do you help resolve this and how does it change management?”
“A 45-year-old man has two biopsy-proven intramuscular myxomas in the thigh. Plain films of the femur show expansile lucent lesions with a ground-glass matrix. What is the unifying diagnosis, what is the underlying mechanism, and how do you manage him?”
Key Definition
- Benign myxoid soft-tissue tumour arising within skeletal muscle
- Bland spindle/stellate cells in abundant hypovascular myxoid stroma
- Does NOT metastasise; recurrence after marginal excision is exceptional
- Classic sarcoma mimic - especially the cellular/hypervascular variant
Who and Where
- Middle-aged adults (mean mid-50s to early 60s)
- Female predominance (~2:1)
- Thigh is the most common site; then buttock, shoulder, upper arm
- Slowly enlarging, deep, usually painless mass
Genetics (High Yield)
- Activating post-zygotic GNAS mutation (codon R201)
- Same gene as fibrous dysplasia - basis of Mazabraud syndrome
- Detectable in the majority of myxomas with sensitive assays (~68% by NGS)
- Malignant myxoid mimics are GNAS-negative
MRI Features
- Fluid-like signal: low T1, very high T2
- Peritumoral fat rind (~65%)
- Bright peripheral muscle oedema (~55%)
- Internal/rim enhancement (not a simple cyst) - more cellular = more enhancement
Histology
- Hypocellular, hypovascular, abundant myxoid matrix
- Bland cells, NO mitoses, NO necrosis (even in cellular foci)
- S100 negative, MUC4 negative; SMA variable, vimentin positive
- GNAS mutation supports the diagnosis
Differential (Myxoid Sarcomas)
- Myxofibrosarcoma - atypia, curvilinear vessels, elderly
- Myxoid liposarcoma - chicken-wire vessels, lipoblasts, DDIT3 fusion
- Low-grade fibromyxoid sarcoma - MUC4 positive, FUS-CREB3L2
- Extraskeletal myxoid chondrosarcoma - EWSR1-NR4A3 fusion
Management
- Treat any deep mass over 5 cm as sarcoma until proven otherwise
- MRI, then planned image-guided CORE biopsy (FNA unreliable)
- Marginal, function-preserving excision is curative
- No radiotherapy or chemotherapy; no wide margins needed
Mazabraud Syndrome
- Intramuscular myxoma(s) + fibrous dysplasia of bone
- Shared activating GNAS mutation; myxomas often multiple
- Treat myxoma and bone disease separately
- Bone disease drives morbidity (deformity, fracture)
Exam Pearls
- Benign but the great myxoid mimic - do not overcall sarcoma
- Fat rind + peripheral oedema + enhancement = think myxoma
- GNAS positive supports myxoma; GNAS negative does NOT exclude it
- Not staged (Enneking/AJCC are for the malignant mimics)
- Always look at the bones - do not miss Mazabraud
Evidence Base and Key Studies
Hypercellular and Hypervascular Variants - The Sarcoma Mimic (Nielsen, MGH)
- Clinicopathologic study of 51 intramuscular myxomas; 35 women and 16 men, mean age 52 years, tumours 2 to 15 cm
- 38 of 51 tumours contained hypercellular regions occupying 10 to 80% of the lesion
- These cellular foci showed NO cytologic atypia, NO mitotic activity and NO necrosis
- No tumour recurred or metastasised on available follow-up (mean 30 months)
- Cellular/vascular foci are commonly mistaken for myxofibrosarcoma, low-grade fibromyxoid sarcoma or myxoid liposarcoma
Surgical Outcomes - Marginal Excision is Curative (Silver, Duke)
- 17 patients (13 women, 4 men), mean age 55 years, tumours mostly in the thigh (quadriceps, adductors, gluteal)
- Most masses were hypointense on T1, hyperintense on T2, well-circumscribed with peripheral enhancement
- Fine-needle aspiration matched the final surgical diagnosis in only 3 of 8 masses biopsied
- All patients treated by marginal excision; tumours 3.5 to 9.5 cm
- No recurrences over a mean 7-year follow-up (range 1 to 20 years); none associated with Mazabraud or McCune-Albright
Characteristic MRI Features (Bancroft, Mayo Clinic)
- Retrospective MRI review of 20 intramuscular myxomas; mean age 61 years, mean size 6.9 cm
- Low T1 signal in 95% and high T2/fluid-sensitive signal in 100% of lesions
- Peritumoral fat rind present in 65%; increased adjacent muscle signal in 55%
- Enhancement (in 11 imaged with gadolinium) was most often intense and heterogeneous (55%)
- Combination of fluid-like signal, fat rind and adjacent muscle signal is strongly suggestive of myxoma
MRI-Histology Correlation (Luna)
- 18 histologically proven intramuscular myxomas in 17 patients (14 women, 3 men), mean age 58.9 years, mostly thigh
- Well-circumscribed masses, hypointense on T1 and hyperintense on T2; pseudocapsule in 12 and peritumoral fat in 16
- Enhancement patterns: peripheral, peripheral plus patchy internal, or peripheral plus linear internal
- More cellular tumours with scant myxoid stroma showed more prominent internal enhancement
- Histology was uniformly hypocellular, hypovascular and myxoid with a partial collagenous capsule
GNAS Mutation Detection by Next-Generation Sequencing (Bekers)
- 34 intramuscular myxoma samples from 33 patients tested with a TaqMan assay and a novel smMIP next-generation sequencing assay
- TaqMan detected GNAS mutations in 55% and smMIP in 57% of samples, with high concordance
- Combining both methods, 68% of sporadic myxomas harboured a GNAS mutation
- Hotspot mutations were p.R201C and p.R201H; novel variants (R201S/L/P and Q227R) were also identified
- Sensitive molecular testing is valuable because these tumours yield little DNA due to low cellularity
GNAS Testing Separates Myxoma from Low-Grade Myxofibrosarcoma (Delaney, RNOH)
- GNAS1 mutations detected in 8 of 28 myxomas (29%) by conventional PCR but 17 of 28 (61%) using more sensitive COLD-PCR
- Mutations were found in two cases that had been favoured as low-grade myxofibrosarcoma
- No GNAS mutations were found in 9 low-grade and 19 high-grade myxofibrosarcomas, or in 40 control samples
- GNAS detection therefore increases diagnostic accuracy when separating myxoma from myxofibrosarcoma
- Demonstrates GNAS mutations are more common in intramuscular myxoma than previously appreciated