Benign Subchondral Mucin-Filled Bone Cyst
- An INTRAOSSEOUS GANGLION is a BENIGN, MUCIN-filled (gelatinous) SUBCHONDRAL BONE CYST with a fibrous lining - essentially a ganglion arising within bone. They are frequently INCIDENTAL and can cause local pain and, rarely, structural problems.
- BE CAREFUL WITH 'COMMON' - NO COHORT SUPPLIES A FREQUENCY. The statement that intraosseous ganglia are quite common is repeated widely, but the published literature on this lesion is CASE REPORTS and small series, and a case report cannot establish how often something occurs. No population or radiological cohort gives a prevalence, no series reports what proportion are symptomatic, and no study gives a RECURRENCE RATE after curettage and grafting. Say that they are benign, often incidental and generally do well after curettage - and resist quoting a percentage that does not exist.
- They characteristically arise in SUBCHONDRAL bone near a joint, the common sites being the CARPUS (especially the LUNATE and scaphoid), the MEDIAL MALLEOLUS of the ankle, the FEMORAL HEAD/ACETABULUM, and around the KNEE - so a well-defined subchondral cyst at these sites in an otherwise normal joint suggests an intraosseous ganglion.
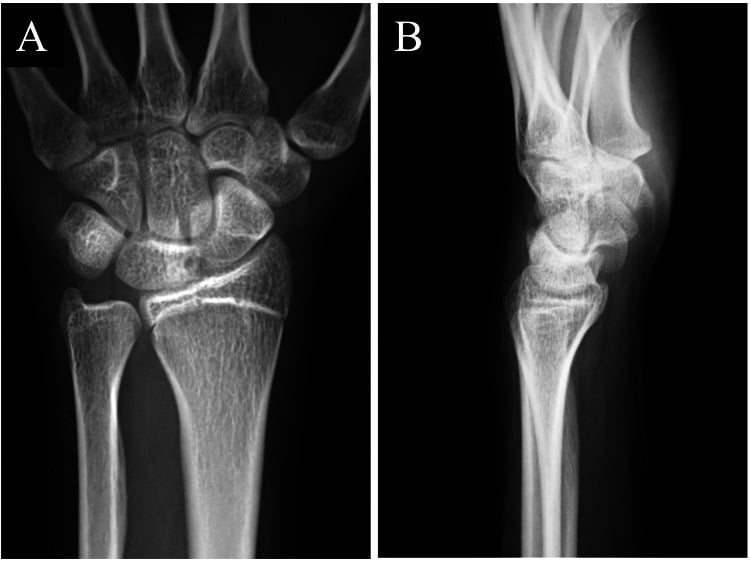
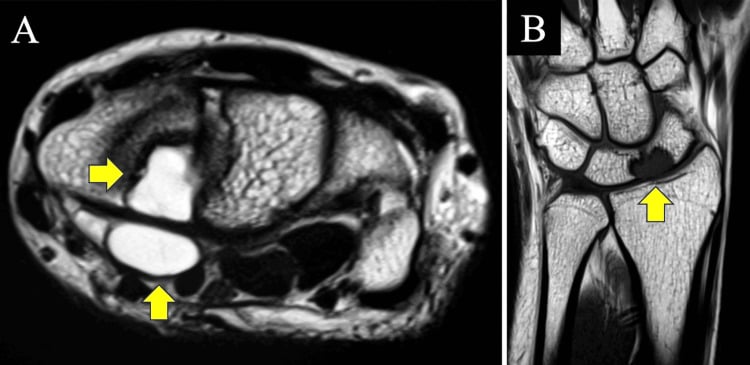
- IMAGING shows a WELL-DEFINED, round or oval LYTIC subchondral lesion with a SCLEROTIC RIM; it usually does NOT communicate with the joint space and the overlying joint is typically preserved, with MRI demonstrating a fluid-like (mucinous) signal - the well-circumscribed, benign appearance is reassuring.
- The key DIFFERENTIAL is the DEGENERATIVE SUBCHONDRAL (geode) CYST, which occurs in a joint with overlying OSTEOARTHRITIS and communicates with the degenerate joint surface, in contrast to the intraosseous ganglion which arises in a relatively NORMAL joint and does not communicate; other lytic lesions (chondroblastoma, giant cell tumour, infection) are usually excluded by the benign, well-defined appearance and location.
- Although benign, an intraosseous ganglion in a confined location can occasionally cause SYMPTOMS or complications: for example, a lunate intraosseous ganglion can cause wrist pain and carpal instability, and a deposit in the carpal tunnel can rarely cause carpal tunnel syndrome - so the lesion is treated when it is the clear source of symptoms.
- MANAGEMENT is conservative when ASYMPTOMATIC - the lesion is benign and incidental lesions need only OBSERVATION; for PERSISTENT symptomatic lesions the treatment is CURETTAGE (removal of the cyst and its lining) with BONE GRAFTING of the defect, which is usually effective, with attention to any associated problem (e.g. addressing carpal instability where present).
- “Intraosseous ganglion = benign, MUCIN-filled SUBCHONDRAL bone cyst ('bone ganglion'). Typical sites: carpus (LUNATE/scaphoid), medial malleolus, femoral head/acetabulum, around the knee. Often incidental - but the literature is CASE REPORTS, so no prevalence or recurrence rate exists to quote.
- “Imaging: well-defined round/oval LYTIC subchondral lesion with a SCLEROTIC RIM; usually does NOT communicate with the joint; overlying joint preserved (vs degenerative geode = OA + communication).
- “Asymptomatic -> OBSERVE; symptomatic -> CURETTAGE + bone GRAFTING (address associated issues, e.g. carpal instability). Benign but can rarely cause symptoms (e.g. lunate ganglion -> wrist pain/instability; carpal tunnel).
A well-defined, round/oval lytic subchondral lesion with a sclerotic rim near a joint (carpus, medial malleolus, hip) in an otherwise normal joint = intraosseous ganglion (benign, mucin-filled).
Degenerative geode = subchondral cyst in an osteoarthritic joint, communicating with the degenerate surface. Intraosseous ganglion arises in a normal joint and usually doesn't communicate.
Features, Imaging & Differential
An intraosseous ganglion is a benign, mucin-filled subchondral bone cyst with a fibrous lining - a ganglion arising within bone - that is common and often incidental but can cause local pain. Typical sites are subchondral bone near a joint: the carpus (lunate, scaphoid), the medial malleolus, the femoral head/acetabulum and around the knee. Imaging shows a well-defined, round/oval lytic lesion with a sclerotic rim, usually not communicating with a preserved overlying joint, and a fluid-like (mucin) signal on MRI. The key differential is the degenerative subchondral (geode) cyst (overlying joint OA, joint communication); other lytic lesions are excluded by the benign, well-defined appearance and location.
- Intraosseous ganglion
- Relatively normal joint
- Degenerative geode
- Osteoarthritic joint
- Intraosseous ganglion
- Usually none
- Degenerative geode
- Communicates with degenerate surface
- Intraosseous ganglion
- Well-defined, sclerotic rim
- Degenerative geode
- Variable; with surrounding OA changes
- Intraosseous ganglion
- Mucin (gelatinous)
- Degenerative geode
- Mucoid/fibrous degenerative material
- Intraosseous ganglion
- Can be the primary cause of pain
- Degenerative geode
- Secondary to osteoarthritis
The Fuller Radiographic Differential
- Chondroblastoma - epiphyseal, but in a skeletally-immature child/adolescent, with a chondroid matrix (stippled calcification); the intraosseous ganglion is typically in an adult.
- Giant cell tumour - epi-metaphyseal, subarticular, eccentric, purely lytic with an ill-defined (non-sclerotic) margin in a skeletally-mature adult - the lack of a sclerotic rim distinguishes it from the well-rimmed ganglion.
- Simple (unicameral) bone cyst - metaphyseal (not subchondral), central, in a child, with a "fallen-fragment" sign.
- Aneurysmal bone cyst - markedly expansile with fluid-fluid levels on MRI.
- Enchondroma - chondroid matrix (rings-and-arcs), usually metaphyseal/diaphyseal.
- Brodie's abscess (subacute osteomyelitis) - lytic with a thick sclerotic rim and the "penumbra sign" on MRI, often with a clinical/inflammatory picture.
- Osteonecrosis-associated cyst - at the femoral head or lunate (Kienbock), accompanied by AVN changes/collapse.
Q: What is the differential of a subchondral/epiphyseal lytic lesion, and how does each differ from an intraosseous ganglion?
A: Degenerative geode (OA + joint communication); chondroblastoma (epiphyseal but in a CHILD, chondroid matrix); giant cell tumour (subarticular, eccentric, NON-sclerotic margin, adult); simple bone cyst (metaphyseal, child, fallen-fragment sign); ABC (expansile, fluid-fluid levels); enchondroma (chondroid rings-and-arcs); Brodie's abscess (thick sclerotic rim, "penumbra sign", infection); osteonecrosis cyst (femoral head/lunate with AVN/collapse). The intraosseous ganglion's well-defined sclerotic rim in a NORMAL adult joint (no OA, no communication) sets it apart.
Management
- Asymptomatic/incidental: observation - the lesion is benign and needs no treatment.
- Persistent symptomatic lesion: curettage (remove the cyst and its lining) with bone grafting of the defect - usually effective.
- Address associated problems: e.g. carpal instability with a lunate/scaphoid ganglion (temporary fixation as needed); decompress a deposit causing carpal tunnel syndrome.
- Confirm benignity: the well-defined subchondral appearance is reassuring; biopsy/curettage histology confirms the diagnosis where there is any doubt.
- Counsel on expectation, not percentages: symptomatic lesions generally settle after curettage, but no series reports a recurrence rate, so avoid quoting one.
The lesions in the radiographic differential each have their own page. The soft-tissue counterpart from which the penetrating type arises is the ganglion cyst; the carpal complications to look for are carpal tunnel syndrome and, where the lunate shows collapse rather than a clean cyst, Kienbock's disease. Among the lytic mimics, chondroblastoma is epiphyseal in a child, giant cell tumour of bone is subarticular with a non-sclerotic margin, aneurysmal bone cyst is expansile with fluid-fluid levels, simple bone cyst is metaphyseal, and Brodie's abscess shows the penumbra sign.
The intraosseous ganglion is a benign, common, often incidental subchondral bone cyst, and the main clinical judgement is whether it is the cause of the patient's symptoms. A well-defined, round or oval lytic subchondral lesion with a sclerotic rim, in an otherwise normal joint at a typical site such as the carpus, medial malleolus or femoral head, is reassuring and, if asymptomatic, needs only observation rather than extensive investigation. When it is the clear source of persistent pain - or causes a complication such as wrist pain and carpal instability from a lunate ganglion, or rarely a carpal tunnel syndrome - it is treated by curettage of the cyst and its lining with bone grafting of the defect, addressing any associated problem at the same time. The lesion should be distinguished from a degenerative geode (which reflects overlying osteoarthritis), and where the imaging appearance is atypical the diagnosis should be confirmed histologically to exclude other lytic lesions.
Histology and How the Lesion Arises
- The histology. A cyst with a fibrous (collagenous) wall lined by bland, flattened spindle (fibroblast-like) cells - there is no true epithelial or synovial lining (exactly like a soft-tissue ganglion) - containing myxoid/mucinous (hyaluronic-acid-rich) gelatinous material. The wall shows myxoid degeneration of the connective tissue, sometimes with reactive new bone or scattered giant cells, and no atypia or mitoses (benign).
- Two pathogenetic types.
- Primary (idiopathic, intramedullary) type - the commoner, non-communicating lesion - is thought to arise de novo within subchondral/medullary bone by myxoid (mucoid) degeneration of intraosseous connective tissue, possibly triggered by local ischaemia or repetitive subchondral microtrauma/stress.
- Penetrating (secondary) type - a soft-tissue (juxta-articular) ganglion or synovial fluid penetrates the cortex into subchondral bone, so this form communicates with the joint.
Q: What is the histology and pathogenesis of an intraosseous ganglion?
A: A fibrous-walled cyst lined by bland flattened spindle cells with no true epithelial/synovial lining (like a soft-tissue ganglion), containing myxoid/mucinous material, with myxoid degeneration of the wall - benign, no atypia. Two types: the primary/idiopathic (commoner, non-communicating) arises de novo by myxoid degeneration of intraosseous connective tissue (± ischaemia/microtrauma); the penetrating (secondary) form is a soft-tissue ganglion/synovial fluid penetrating the cortex, so it communicates with the joint.
Mnemonics & Memory Aids
GANGLION
Hook:GANGLION: Ganglion in bone, Around joints, No joint communication, Geode differential, Lytic+sclerotic rim, Incidental->observe, Operate if symptomatic, Note associations.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A well-defined subchondral lytic lesion with a sclerotic rim is found in the lunate. What is it, and how do you manage it?”
What it is
- Benign, mucin-filled subchondral bone cyst ('bone ganglion'), fibrous lining
- Often incidental - but no cohort gives a prevalence; the literature is case reports
- Can cause local pain / occasional complications
Sites & imaging
- Carpus (lunate/scaphoid), medial malleolus, femoral head/acetabulum, around knee
- Well-defined round/oval lytic lesion with a sclerotic rim
- Usually no joint communication; overlying joint preserved; fluid signal on MRI
Differential
- Degenerative subchondral (geode) cyst: OA + joint communication
- Other lytic lesions excluded by benign well-defined appearance/location
- Confirm histologically if atypical
Management
- Asymptomatic: observation
- Symptomatic: curettage (remove cyst + lining) + bone grafting
- Address associations: carpal instability (fixation); rare carpal tunnel syndrome (decompression)
What the Published Evidence Can and Cannot Tell You
Almost everything written about the intraosseous ganglion consists of single case reports and small series, and that shapes what can honestly be claimed. A case report establishes that something can happen, never how often it happens. So the widely repeated statement that these lesions are "actually quite common" - itself traceable to a case report - has no cohort behind it. Nor does any study give the proportion that become symptomatic, the proportion found incidentally, or the recurrence rate after curettage and bone grafting. What the case literature does support is that the lesion is benign, that symptomatic lesions improve after curettage, and that a carpal lesion can cause wrist pain and instability or, rarely, carpal tunnel syndrome. Those are the defensible statements.
Possibility, and mechanism. A lunate lesion can cause carpal tunnel syndrome, so an atypical carpal tunnel presentation is worth imaging. A ganglion spanning the scaphoid and lunate can produce instability that needs temporary fixation alongside curettage, and bone formation was seen in the curettage bed at follow-up. These change what you look for and what you offer - without pretending to be a frequency.
Counsel on mechanism and expectation rather than percentages: this is a benign cyst, an incidental one needs only observation, and if it is genuinely the source of pain, curettage with grafting usually settles the symptoms - while being honest that no series quantifies how often it comes back. If the imaging is atypical, the diagnosis is confirmed histologically rather than assumed.
Evidence & Key Studies
Intraosseous ganglion spanning the scaphoid and lunate - presentation and treatment
- A single case of an intraosseous ganglion spanning two adjacent carpal bones, which the authors note is uncommon. A carpal intraosseous ganglion can cause wrist pain and carpal instability - as a case report this establishes that the association occurs, not how often.
- Imaging showed small subchondral cysts in the lunate and scaphoid; treatment was bone curettage with sharp curettes, and temporary joint fixation was added for the associated carpal instability.
- At follow-up, wrist pain improved, instability resolved and bone formation was seen in the curettage area - supporting curettage (with grafting/fixation as needed) for symptomatic intraosseous ganglia, in one patient with no comparison group and no stated recurrence rate.
Carpal tunnel syndrome caused by an intraosseous ganglion of the lunate
- An intraosseous (interosseous) ganglion of the lunate caused unilateral wrist pain and carpal tunnel syndrome, highlighting that intraosseous ganglia can occasionally produce symptoms beyond local pain.
- It illustrates the need to consider uncommon aetiologies, such as an intraosseous ganglion, in patients with atypical carpal tunnel symptoms.
- MRI was used to identify the lunate intraosseous ganglion.
The occurrence of intraosseous ganglia in the carpus (lunate/scaphoid) with the capacity to cause wrist pain and carpal instability, and symptomatic improvement after curettage with fixation for associated instability, come from the cited Hama report; the presentation of a lunate intraosseous ganglion as carpal tunnel syndrome from the cited Heading report. Both are single case reports, so they establish that these things happen and not how often. No cohort gives a prevalence for this lesion, the proportion that become symptomatic, or a recurrence rate after curettage and grafting, and no study compares curettage with observation or with grafting alternatives - so the page describes the lesion as benign and generally responsive to curettage without quoting figures that do not exist. The benign mucin-filled subchondral nature, the other common sites (medial malleolus, femoral head/acetabulum, knee), the well-defined lytic-with-sclerotic-rim appearance, the distinction from a degenerative geode, and observation-versus-curettage-and-grafting management are standard, well-established teaching.