Rare Benign Fibrous Bone Tumour
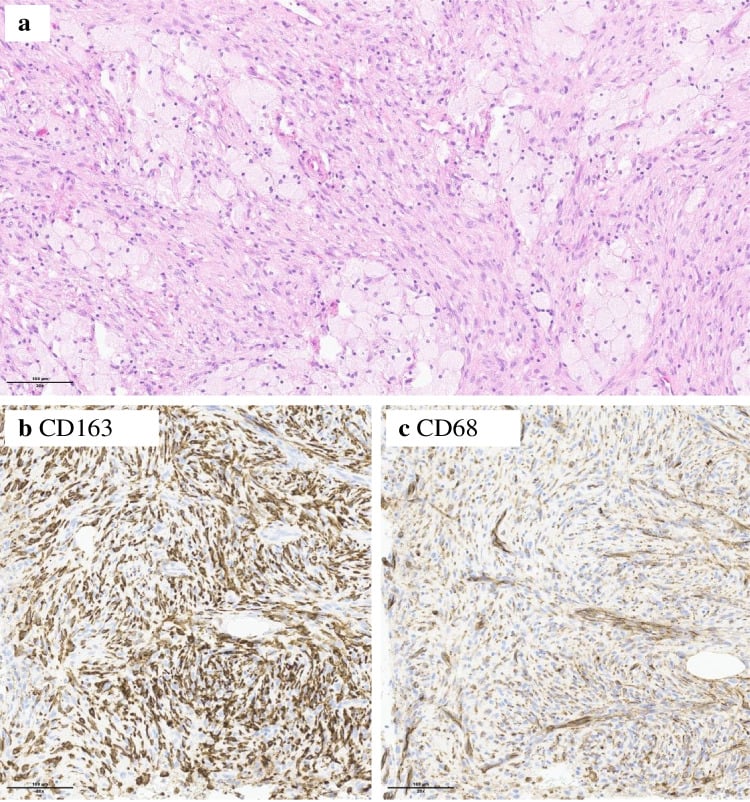
- BENIGN FIBROUS HISTIOCYTOMA OF BONE (BFHB) is a RARE benign mesenchymal tumour - representing less than 1% of all benign bone tumours - and is a somewhat CONTROVERSIAL entity, histologically characterised by a mixture of FIBROBLASTS arranged in a STORIFORM (cartwheel) pattern with varying amounts of OSTEOCLAST-TYPE GIANT CELLS and FOAMY (lipid-laden) MACROPHAGES.
- Its histology is essentially IDENTICAL to that of the common NON-OSSIFYING FIBROMA (NOF)/fibrous cortical defect, so BFHB is distinguished from NOF on CLINICAL and radiological grounds rather than histology alone: it tends to occur in ATYPICAL LOCATIONS (pelvis, axial skeleton, and the diaphysis or epiphysis of long bones) and in OLDER patients who are usually SYMPTOMATIC (painful), in contrast to the typical young, asymptomatic, metaphyseal NOF that regresses.
- The ENTITY ITSELF IS CONTESTED: because the histology is identical to NOF and it shares NOF's MAPK-pathway mutations (KRAS, FGFR1), the current WHO classification places it WITHIN THE NOF SPECTRUM - an atypically sited or symptomatic NOF - rather than treating it as a separate tumour. Answer the question both ways: know the classical clinical distinction, and know that the separate label is no longer regarded as a distinct entity.
- It is a BENIGN tumour, and CURETTAGE or simple RESECTION is usually CURATIVE; a LOCAL RECURRENCE figure of up to about 11% is widely quoted, but it is repeated from earlier literature by a single case report with no stated denominator, so treat it as an indication that recurrence is not rare rather than a firm risk. RARE reports of MALIGNANT TRANSFORMATION exist - one following prolonged stabilisation on denosumab - so follow-up is warranted.
- DIAGNOSIS is largely one of EXCLUSION: because the histology overlaps with other lesions, the differential (giant cell tumour of bone, non-ossifying fibroma, fibrous dysplasia, aneurysmal bone cyst, chondromyxoid fibroma) must be excluded by correlating the clinical picture, imaging (a well-defined lytic lesion, often with a sclerotic rim) and histology, ideally at a specialist bone-tumour centre.
- It is worth noting that the historical term 'malignant fibrous histiocytoma' is a SEPARATE, MALIGNANT entity now largely reclassified as UNDIFFERENTIATED PLEOMORPHIC SARCOMA - it must NOT be confused with benign fibrous histiocytoma of bone, which is benign.
- MANAGEMENT is therefore: confirm the diagnosis (excluding mimics) on imaging and biopsy, treat by CURETTAGE (with grafting) or simple resection, with bone grafting/fixation as needed for structural lesions, and FOLLOW UP for recurrence; the rare aggressive/recurrent or transformed lesion is managed more aggressively at a sarcoma unit.
- “Benign fibrous histiocytoma of bone (BFHB) = rare (under 1% of benign bone tumours), histologically IDENTICAL to non-ossifying fibroma (storiform fibroblasts + osteoclast-type giant cells + foamy macrophages).
- “Distinguished from NOF CLINICALLY: ATYPICAL site (pelvis/axial/diaphysis-epiphysis) + OLDER, SYMPTOMATIC patients (vs young, asymptomatic, metaphyseal NOF).
- “Benign; curettage/resection usually curative but recurrence is not rare (~11% quoted, no published denominator - follow up); RARE malignant transformation. Diagnosis of exclusion. WHO now places it within the NOF SPECTRUM. Do NOT confuse with 'malignant fibrous histiocytoma' (= undifferentiated pleomorphic sarcoma, malignant).
Histology like a non-ossifying fibroma (storiform fibroblasts + giant cells + foamy macrophages) but in an atypical site (pelvis/axial/diaphysis-epiphysis) and an older, symptomatic patient = BFH of bone.
Malignant fibrous histiocytoma is a different, malignant tumour (now undifferentiated pleomorphic sarcoma). BFH of bone is benign (but up to ~11% recur; rare transformation).
What It Is & How It Differs from NOF
Benign fibrous histiocytoma of bone is a rare benign fibrous tumour (less than 1% of benign bone tumours), histologically a storiform proliferation of fibroblasts with osteoclast-type giant cells and foamy macrophages - identical to non-ossifying fibroma. It is separated from NOF clinically: it occurs in atypical locations (pelvis, axial skeleton, long-bone diaphysis/epiphysis) and in older, symptomatic patients, whereas NOF is typically young, asymptomatic and metaphyseal. It is benign but recurs in a notable minority (up to ~11%) after curettage, with rare malignant transformation, and the diagnosis is largely one of exclusion of other giant-cell-rich/fibrous lesions.
- Benign fibrous histiocytoma of bone
- Storiform fibroblasts + giant cells + foamy macrophages
- Non-ossifying fibroma
- Identical
- Benign fibrous histiocytoma of bone
- Older (adults)
- Non-ossifying fibroma
- Children/adolescents
- Benign fibrous histiocytoma of bone
- Atypical (pelvis/axial/diaphysis-epiphysis)
- Non-ossifying fibroma
- Metaphysis of long bones (eccentric, cortical)
- Benign fibrous histiocytoma of bone
- Usually symptomatic (painful)
- Non-ossifying fibroma
- Usually asymptomatic/incidental
- Benign fibrous histiocytoma of bone
- Benign; up to ~11% recur; rare transformation
- Non-ossifying fibroma
- Benign; regresses/heals spontaneously
Imaging Features and the Radiographic Differential
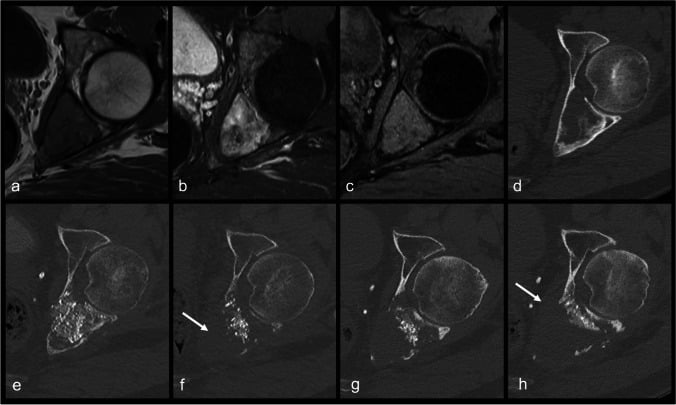
- BFHB on imaging. A geographic, well-defined lytic lesion, usually with a thin sclerotic rim (a marginated, non-aggressive pattern), eccentric or central, sometimes mildly expansile/multiloculated; no matrix mineralisation and no aggressive periosteal reaction (unless there is a pathological fracture). MRI is non-specific (low-to-intermediate T1, variable T2, enhances) but defines extent.
- The imaging differential.
- Giant cell tumour (the key one): epi-metaphyseal, subarticular (abutting the joint), eccentric, purely lytic, with an ill-defined / non-sclerotic margin in a skeletally-mature adult - the lack of a rim and the subarticular site favour GCT.
- Non-ossifying fibroma: metaphyseal, cortically based, well-defined sclerotic scalloped margin, "bubbly", in a child - and it regresses.
- Fibrous dysplasia: medullary, "ground-glass" matrix, often long-segment with bowing.
- Aneurysmal bone cyst: markedly expansile with fluid-fluid levels.
- Chondromyxoid fibroma: eccentric metaphyseal, lobulated with a sclerotic scalloped margin.
Q: What are the imaging features of BFHB, and how does imaging help exclude the mimics?
A: BFHB is a geographic, well-defined lytic lesion, usually with a thin sclerotic rim, no matrix and no aggressive periosteal reaction. The key mimic is giant cell tumour - epi-metaphyseal, subarticular, eccentric, with a non-sclerotic margin (the lack of a rim + the subarticular site favour GCT). NOF is metaphyseal/cortical/sclerotic-rimmed in a child; fibrous dysplasia has a ground-glass matrix; ABC is expansile with fluid-fluid levels; chondromyxoid fibroma is lobulated/eccentric.
Management
- Diagnosis: correlate clinical picture, imaging (well-defined lytic lesion +/- sclerotic rim) and histology; exclude giant cell tumour, NOF, fibrous dysplasia, aneurysmal bone cyst, chondromyxoid fibroma - ideally at a specialist bone-tumour centre.
- Treatment: curettage (with bone grafting) or simple resection, with grafting/fixation for structural lesions - usually curative.
- Follow up: for local recurrence. The figure usually quoted is up to about 11 percent, but treat it with caution - it is a number repeated from earlier literature by a single case report, without a stated denominator or source cohort, so it indicates that recurrence is not rare rather than giving a reliable risk to quote at consent.
- Aggressive/recurrent/transformed lesions: managed at a sarcoma unit. Denosumab has been used for unresectable or recurrent disease and produced prolonged stabilisation in a reported case - but that same patient subsequently underwent malignant transformation, so it is a specialist decision under oncological supervision, not a routine option, and continued surveillance is required whatever the initial response.
Two cautions matter with benign fibrous histiocytoma of bone. First, because its histology is identical to the common non-ossifying fibroma and overlaps with several giant-cell-rich lesions, the diagnosis is essentially one of exclusion: the clinical setting (older, symptomatic patient; atypical location), the imaging and the histology must be correlated, ideally at a specialist bone-tumour centre, so that more significant lesions - particularly giant cell tumour of bone - are not missed. Second, the nomenclature is a trap: 'malignant fibrous histiocytoma' is a wholly different, malignant tumour, now largely reclassified as undifferentiated pleomorphic sarcoma, and must not be conflated with the benign entity. While BFH of bone is benign and usually cured by curettage or simple resection, it recurs in a notable minority and has rare reports of malignant transformation, so follow-up is appropriate and any aggressive, recurrent or transformed lesion should be referred for specialist management.
Immunohistochemistry, Molecular Basis, and Why the Entity Is Contested
- Immunophenotype. The histiocytic cells and foamy macrophages are CD68/CD163-positive; the giant cells are osteoclast-type (CD68+). There is no specific defining marker - so immunohistochemistry is used mainly to exclude mimics.
- The discriminator from giant cell tumour. GCT of bone carries the H3F3A (H3.3) G34W mutation, so an H3.3 G34W immunostain is positive in GCT and negative in BFHB/NOF - the single most useful marker for that critical distinction.
- Why it is "controversial". Non-ossifying fibroma (and hence BFHB, being histologically identical) carries activating MAPK-pathway mutations (KRAS, FGFR1); this shared molecular basis, together with the identical histology, has led many - and the current WHO classification - to regard BFHB as within the NOF spectrum (an "atypical" or symptomatic/atypically-sited NOF) rather than a truly separate entity.
Q: How is BFHB confirmed and separated from giant cell tumour, and why is it "controversial"?
A: The histiocytic cells/foamy macrophages are CD68/CD163-positive with no specific marker, so IHC is used to exclude mimics. The key one is giant cell tumour, which carries the H3.3 (H3F3A) G34W mutation - the H3.3 G34W immunostain is positive in GCT, negative in BFHB/NOF. BFHB is "controversial" because it is histologically identical to NOF and shares NOF's MAPK-pathway mutations (KRAS/FGFR1), so the WHO now regards it as within the NOF spectrum rather than a distinct entity.
Mnemonics & Memory Aids
STORIFORM
Hook:STORIFORM: Storiform/giant cells/foamy macrophages, aTypical site+older, exclude Other lesions, Infrequent, curette/resect, recur ~11%, not Malignant FH.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A biopsy of a painful pelvic lytic lesion in an adult shows storiform fibroblasts with giant cells and foamy macrophages. What is the diagnosis and how do you manage it?”
What it is
- Rare benign fibrous bone tumour (under 1% of benign bone tumours)
- Histology = storiform fibroblasts + osteoclast-type giant cells + foamy macrophages (like NOF)
- Controversial entity
Distinguished from NOF
- Atypical site: pelvis, axial skeleton, long-bone diaphysis/epiphysis
- Older, usually symptomatic (painful) patients
- NOF = young, asymptomatic, metaphyseal, regresses
Behaviour & management
- Benign; curettage (+graft) or simple resection usually curative
- Recurrence not rare (~11% quoted, no published denominator) - follow up; rare malignant transformation
- WHO now places it within the NOF spectrum (shared KRAS/FGFR1) - not a distinct entity
- Denosumab reported for recurrent disease: stabilised, then transformed - specialist decision only
- Diagnosis of exclusion; don't confuse with malignant fibrous histiocytoma (UPS)
Evidence & Key Studies
Recurrent benign fibrous histiocytoma of bone with later malignant transformation
- A SINGLE CASE REPORT - of a pelvic benign fibrous histiocytoma of bone that recurred, stabilised for a prolonged period on denosumab, and then underwent malignant transformation.
- Describes the entity as rare (less than 1 percent of all benign bone tumours) and explicitly as CONTROVERSIAL, with the storiform fibroblastic histology, osteoclast-type giant cells and foamy macrophages.
- The often-quoted relapse figure of up to 11 percent is cited BY this report from earlier literature - it is not a rate this paper measured, and no denominator or source cohort is given with it.
- Denosumab produced long-lasting disease stabilisation before transformation occurred; whether that sequence is causal or coincidental cannot be determined from one case.
- A single patient: it establishes that malignant transformation can happen, and nothing about how often.
The rarity (less than 1% of benign bone tumours), the storiform fibroblastic histology with osteoclast-type giant cells and foamy macrophages, the usual cure by curettage/simple resection with up to about 11% relapse, and the rare malignant transformation come from the cited Wetterwald report. The histological identity with non-ossifying fibroma and the clinical distinction (atypical site, older/symptomatic patients), the status as a diagnosis of exclusion, and the separation from 'malignant fibrous histiocytoma' (undifferentiated pleomorphic sarcoma) are standard, well-established teaching. The cited source is a single case report, so it establishes that malignant transformation and a denosumab response can occur, and nothing about how often; the 11 percent relapse figure is one that report quotes from earlier literature rather than measures, and no cohort with a stated denominator supporting it was retrieved - so it is given here with that caveat and should not be quoted as a firm consent figure. No trial of any treatment in this entity exists, and no evidence-based follow-up interval or duration was found. See also non-ossifying fibroma, giant cell tumour of bone, fibrous dysplasia, aneurysmal bone cyst, chondromyxoid fibroma and, for the malignant tumour whose old name causes the confusion, undifferentiated pleomorphic sarcoma.