Formerly MFH | Diagnosis of Exclusion | Most Common Adult Soft-Tissue Sarcoma
- UPS is a diagnosis of EXCLUSION - a high-grade pleomorphic sarcoma showing NO specific line of differentiation after a full immunohistochemistry and molecular workup
- The term replaced 'malignant fibrous histiocytoma' (MFH) because the cell of origin is not histiocytic; many former MFH cases are reclassified once a lineage is found
- Most common presentation is an enlarging, deep, painless soft-tissue mass in the thigh of an older adult
- Treatment is wide surgical resection; radiotherapy improves LOCAL control for extremity soft-tissue tumours and is timing-dependent (preop lower dose/more wound problems vs postop higher dose)
- Primary UPS of bone behaves like and is treated like osteosarcoma, with neoadjuvant chemotherapy plus wide resection
- “Storiform (cartwheel) and pleomorphic patterns are classic but NOT specific - the diagnosis depends on excluding dedifferentiated liposarcoma, leiomyosarcoma, MPNST, melanoma, sarcomatoid carcinoma
- “Always exclude dedifferentiated liposarcoma with MDM2/CDK4 (FISH or IHC) before settling on UPS, especially retroperitoneal tumours
- “Lung is the dominant metastatic site; staging CT chest is mandatory and lymph node spread is uncommon
- “Grade, tumour size and depth, and margin status are the key prognostic drivers
UPS has no positive defining marker. It is a high-grade pleomorphic sarcoma in which a full immunohistochemistry and molecular panel has failed to show any specific line of differentiation. The biggest trap is calling a tumour UPS without first excluding dedifferentiated liposarcoma (MDM2/CDK4), leiomyosarcoma, MPNST, melanoma and sarcomatoid carcinoma.
'Malignant fibrous histiocytoma' is historical. The cells are not histiocytic; the term has been replaced by undifferentiated pleomorphic sarcoma in the WHO classification. If you say "MFH" in a viva, immediately add that it is now called UPS and explain why.
For extremity soft-tissue UPS, surgery alone is often not enough. Radiotherapy improves local control. Preoperative radiotherapy uses a lower dose but causes more acute wound-healing complications; postoperative radiotherapy uses a higher dose with more late fibrosis. Timing is an active surgical decision.
Primary UPS of bone is treated like high-grade osteosarcoma: neoadjuvant chemotherapy, wide resection, then adjuvant chemotherapy. Prospective data (EURO-B.O.S.S.) show survival comparable to age-matched osteosarcoma with an osteosarcoma-type regimen.
Overview and Epidemiology
Undifferentiated pleomorphic sarcoma (UPS) is a high-grade malignant mesenchymal tumour showing no identifiable line of differentiation on light microscopy, immunohistochemistry, or molecular testing. It was historically called malignant fibrous histiocytoma (MFH) in the belief that it arose from histiocytes, but that origin was disproven, and the entity was renamed undifferentiated pleomorphic sarcoma in the WHO classification. It is best understood not as a single disease but as the default category that remains once every definable sarcoma and non-sarcoma has been excluded.
"MFH" was once the most common adult soft-tissue sarcoma diagnosis, but improved immunohistochemistry and molecular testing showed that a large proportion of these tumours were actually dedifferentiated liposarcoma, leiomyosarcoma, MPNST, or other definable entities. The remaining tumours - truly without a line of differentiation - are now called undifferentiated pleomorphic sarcoma. The clinical importance is that the label is only valid after a thorough exclusion process, and finding a lineage (for example MDM2 amplification) changes both the diagnosis and the prognosis.
- Age: Peak in the 6th-7th decade (most patients over 50 years)
- Sex: Slight male predominance
- Site: Deep soft tissue of the extremities, especially the thigh; also retroperitoneum and, less commonly, primary bone
- Status: One of the most common adult soft-tissue sarcomas even after reclassification
- Prior radiotherapy: UPS is a recognised radiation-associated sarcoma after a latency of years
- Older age: Strongly age-associated, unlike paediatric round-cell sarcomas
- Genetics: Complex karyotype with no single recurrent translocation (contrast synovial sarcoma or Ewing sarcoma)
- Lymph nodes: Nodal spread is uncommon but more frequent than for most other sarcomas
Soft Tissue versus Bone UPS
- Soft-Tissue UPS
- Enlarging deep painless mass, often thigh
- Primary UPS of Bone
- Progressive bone pain, lytic destructive lesion
- Soft-Tissue UPS
- Large heterogeneous mass with necrosis on MRI
- Primary UPS of Bone
- Lytic, permeative, no mineralised matrix
- Soft-Tissue UPS
- Selective (large, high-grade, deep extremity tumours)
- Primary UPS of Bone
- Standard - osteosarcoma-type neoadjuvant and adjuvant
- Soft-Tissue UPS
- Improves local control for extremity tumours
- Primary UPS of Bone
- Adjunct for inadequate margins / unresectable sites
- Soft-Tissue UPS
- Dedifferentiated liposarcoma (MDM2)
- Primary UPS of Bone
- Osteosarcoma (any osteoid changes the diagnosis)
Pathophysiology and Histology
Pathogenesis
UPS arises from primitive mesenchymal cells that fail to differentiate along any recognisable lineage. Cytogenetically it shows a complex karyotype with multiple non-specific chromosomal gains and losses, in contrast to the single recurrent gene fusions seen in synovial sarcoma (SS18-SSX) or Ewing sarcoma (EWSR1-FLI1). There is no diagnostic positive marker, so the diagnosis is reached by exclusion.
A pleomorphic high-grade sarcoma should only be called UPS after a panel has excluded a definable line of differentiation. The essential negatives are: cytokeratin/EMA (carcinoma), S100/SOX10 (melanoma, MPNST), desmin/SMA/h-caldesmon (smooth muscle), myogenin/MyoD1 (rhabdomyosarcoma), and MDM2/CDK4 amplification (dedifferentiated liposarcoma). Missing a dedifferentiated liposarcoma is the classic error because it changes management and prognosis.
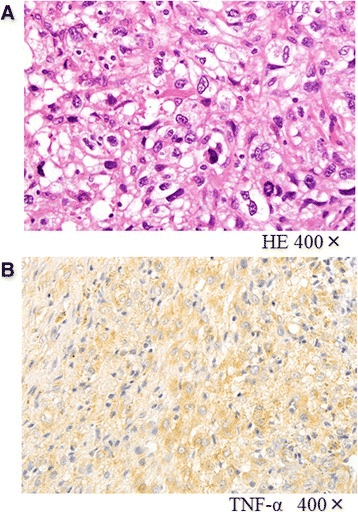
Histological Features
- Pleomorphic cells: Marked nuclear pleomorphism, bizarre giant cells
- Storiform pattern: Cartwheel arrangement of spindle cells (classic but not specific)
- Mitoses: Frequent, often atypical mitotic figures
- Necrosis: Common in high-grade tumours
- No matrix / no lineage: No osteoid, chondroid, lipoblasts or specific differentiation
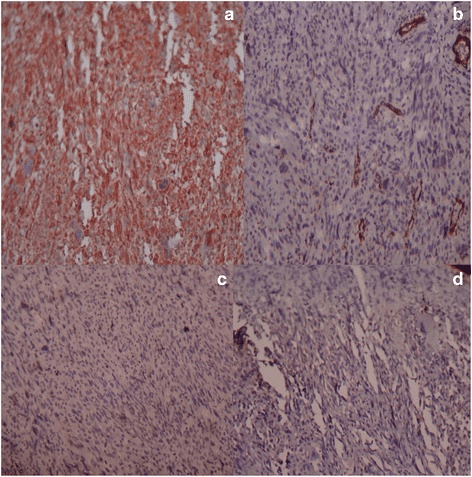
- Vimentin: Positive (non-specific mesenchymal marker)
- Cytokeratin / EMA: Negative (excludes carcinoma)
- S100 / SOX10: Negative (excludes melanoma, MPNST)
- Desmin / SMA / h-caldesmon: Negative (excludes muscle tumours)
- MDM2 / CDK4: Negative (excludes dedifferentiated liposarcoma)
Histological Variants Historically Grouped Under MFH
- Key feature
- Cartwheel pattern, pleomorphic cells
- Modern view
- Core of present-day UPS
- Key feature
- Myxoid stroma, curvilinear vessels
- Modern view
- Now a separate entity - myxofibrosarcoma
- Key feature
- Osteoclast-like giant cells
- Modern view
- Undifferentiated pleomorphic sarcoma with giant cells
- Key feature
- Xanthoma cells, inflammation
- Modern view
- Often reclassified (e.g. dedifferentiated liposarcoma)
- Key feature
- Blood-filled spaces, young patients
- Modern view
- Now angiomatoid fibrous histiocytoma - low malignant potential
The former "myxoid MFH" is now myxofibrosarcoma, the myxoid end of the pleomorphic-sarcoma spectrum, and it earns its own exam answer because of one defining behaviour: it spreads insidiously along fascial planes well beyond the apparent mass, producing a curvilinear infiltrative "tail" of high T2 signal on MRI that is easy to under-resect. As a result it has the highest local-recurrence rate of the soft-tissue sarcomas, and recurrences can be repeated.
Practical consequences:
- Image and resect the tail, not just the obvious lump - take generous margins and use the MRI tail sign to plan the excision; a margin that looks adequate around the bulk can still leave infiltrative disease.
- It is typically a superficial/subcutaneous tumour of elderly limbs, often low-grade for metastasis but high for local recurrence (the opposite emphasis to deep high-grade UPS, where metastasis dominates).
- A positive or close margin warrants re-excision and radiotherapy, and the long natural history means prolonged local surveillance.
Exam point: myxofibrosarcoma = the infiltrative-tail, highest-local-recurrence pleomorphic sarcoma - read the MRI tail, excise widely with the tail, and re-excise/irradiate close margins, because the bulk underestimates the disease.
Clinical Presentation
Symptoms
The most common presentation of soft-tissue UPS is a painless, progressively enlarging deep mass, most often in the thigh. Because the tumour is deep and grows slowly at first, patients frequently present late with a large mass. Pain, when present, is usually due to compression of adjacent structures rather than the tumour itself. Primary UPS of bone presents instead with progressive bony pain and sometimes pathological fracture.
- Mass: Deep, firm, fixed, enlarging
- Pain: Often absent until large or compressing structures
- Size: Frequently over 5 cm at presentation
- Site: Thigh most common, then other extremity sites, retroperitoneum
- Systemic: Usually well; weight loss only with advanced disease
- Pain: Progressive, may be nocturnal
- Fracture: Pathological fracture in a minority
- Lesion: Lytic destructive metaphyseal lesion
- Site: Around the knee (distal femur, proximal tibia) common
- Labs: Usually non-specific (unlike Paget-associated tumours)
The Critical Referral Trap
A deep-seated soft-tissue mass, a mass larger than 5 cm, or any lump that is enlarging should be referred to a sarcoma unit and imaged before any intervention. UPS is frequently mislabelled as a haematoma, lipoma or cyst. Do not perform an unplanned excision ("whoops procedure"), drain it, or biopsy it through a non-excisable track, as this contaminates tissue planes and compromises later limb-salvage surgery.
Physical Examination
Systematic Examination of a Soft-Tissue Mass
- Size and site: Measure; note depth relative to fascia
- Skin: Usually intact; look for prior scars or radiotherapy tattoos
- Overlying changes: Venous prominence with large tumours
- Consistency: Firm, often fixed to deep structures
- Mobility: Reduced if deep to or fixed to fascia
- Tenderness: Often minimal
- Neurovascular: Assess distal pulses, sensation and motor function
- Joint range: May be limited if juxta-articular
- Function: Document baseline for reconstruction planning
- Lymph nodes: Usually not enlarged, but examine (nodal spread possible)
- Chest: Lung is the dominant metastatic site - low threshold for CT chest
Investigations and Imaging
Magnetic Resonance Imaging (MRI)
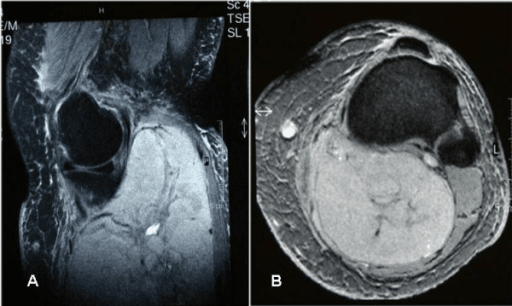
MRI is the imaging modality of choice for a soft-tissue mass. UPS typically appears as a large, deep, heterogeneous mass that is low to intermediate on T1, high and heterogeneous on T2, with internal necrosis and heterogeneous enhancement after gadolinium. MRI defines the compartment, the relationship to neurovascular structures, and the resection plan.
- Signal Intensity
- Low to intermediate (isointense to muscle)
- Clinical Significance
- Defines anatomical extent and fascial relationships
- Signal Intensity
- High and heterogeneous
- Clinical Significance
- Shows necrosis, peritumoral oedema, soft-tissue extent
- Signal Intensity
- Heterogeneous enhancement
- Clinical Significance
- Viable tumour enhances; necrosis does not - helps biopsy targeting
- Signal Intensity
- High signal
- Clinical Significance
- Sensitive for tumour and oedema beyond the gross mass
Staging Workup
- Purpose
- Local staging and surgical planning
- Findings
- Large heterogeneous mass, necrosis, neurovascular relationship
- Purpose
- Detect pulmonary metastases (dominant site)
- Findings
- Lung nodules if metastatic - mandatory in high-grade disease
- Purpose
- Histological diagnosis, grade, exclusion panel
- Findings
- Pleomorphic sarcoma, lineage markers negative
- Purpose
- Characterise lytic lesion, exclude matrix
- Findings
- Permeative lytic lesion with no mineralised matrix
- Purpose
- Exclude dedifferentiated liposarcoma
- Findings
- Negative supports UPS; positive changes the diagnosis
Biopsy Principles
Histological confirmation is mandatory before definitive treatment. The biopsy must be planned so that the track can be excised at the definitive operation, and ideally performed by or in coordination with the sarcoma surgeon.
Essential biopsy considerations:
- Biopsy performed by, or in coordination with, the treating sarcoma surgeon
- Image-guided core needle biopsy preferred over open biopsy (less contamination)
- Track must be placed so it can be excised en bloc at definitive surgery (longitudinal in an extremity)
- Avoid crossing uninvolved compartments, joints or neurovascular bundles
- Multiple cores from enhancing (viable) areas, avoiding necrosis
- Meticulous haemostasis to avoid a contaminating haematoma
- Expert musculoskeletal pathology review with a full immunohistochemistry and molecular panel
An unplanned excision of an unsuspected sarcoma (the "whoops procedure") contaminates the surgical field, leaves microscopic disease, and converts a straightforward wide excision into a re-excision of a larger volume of tissue, frequently requiring adjuvant radiotherapy and worsening function. The correct sequence is image, then biopsy through a planned track, then resect - never excise a deep or large soft-tissue mass without a diagnosis.
The warning is "don't do it"; the examinable follow-up is what to do once an unplanned (marginal/intralesional) excision has already happened - a common real referral. Do not simply observe:
- Re-stage properly: dedicated MRI of the operated bed (interpret with caution - post-surgical change mimics/masks tumour) and a CT chest, with expert pathology review of the resected specimen and margins.
- Plan a re-excision of the entire tumour bed (including all scars and drain sites) even when imaging looks clear, because residual tumour is found in a large proportion (commonly cited as around one-third to one-half) of "whoops" re-excision specimens and residual disease drives recurrence.
- Add radiotherapy to the re-excision in most cases (the contaminated, ill-defined field after an unplanned procedure usually warrants it), and manage through the sarcoma MDT.
- The penalty of the original error is a larger resection, more frequent flap reconstruction, more radiotherapy and worse function than a correctly-staged primary wide excision would have needed.
Exam point: an unplanned sarcoma excision is not salvaged by watching - re-stage, re-excise the whole bed/scars (high residual rate), and irradiate, all via the sarcoma unit.
Differential Diagnosis
- Distinguishing histology
- Pleomorphic, storiform, no lineage
- Immunohistochemistry / molecular
- Vimentin+, all specific markers negative
- Key point
- Diagnosis of exclusion
- Distinguishing histology
- Pleomorphic areas, may lack obvious fat
- Immunohistochemistry / molecular
- MDM2 and CDK4 amplified
- Key point
- Must always exclude - changes prognosis
- Distinguishing histology
- Spindle cells, cigar-shaped nuclei
- Immunohistochemistry / molecular
- SMA+, desmin+, h-caldesmon+
- Key point
- Smooth-muscle markers positive
- Distinguishing histology
- Spindle cells, nerve association
- Immunohistochemistry / molecular
- S100 patchy, SOX10+, H3K27me3 loss
- Key point
- Often arises from a nerve or in NF1
- Distinguishing histology
- Epithelioid or spindled pleomorphic
- Immunohistochemistry / molecular
- S100+, SOX10+, HMB45+, Melan-A+
- Key point
- Can perfectly mimic sarcoma
- Distinguishing histology
- Spindle/pleomorphic, epithelial clues
- Immunohistochemistry / molecular
- Cytokeratin+, EMA+
- Key point
- Look for a known carcinoma primary
A pleomorphic sarcoma that is actually a dedifferentiated liposarcoma has a different prognosis and is biologically distinct, and the distinction is frequently impossible on morphology alone.
Test for MDM2 and CDK4 (amplification by FISH, or overexpression by immunohistochemistry). Amplification indicates dedifferentiated liposarcoma; a negative result supports UPS. This is especially important for retroperitoneal pleomorphic tumours, where dedifferentiated liposarcoma is common.
"Before I would commit to a diagnosis of undifferentiated pleomorphic sarcoma I would confirm that MDM2 and CDK4 are not amplified, because a dedifferentiated liposarcoma can look identical and is the most important mimic, particularly in the retroperitoneum."
Management Algorithm
Soft-Tissue UPS Surgical Management
Goal: Complete tumour resection with wide oncological margins while preserving limb function where possible. Management is delivered through a sarcoma multidisciplinary team.
Treatment Pathway for Extremity Soft-Tissue UPS
- Sarcoma MDT discussion (surgeon, radiologist, pathologist, radiation and medical oncologist)
- Review MRI for extent and neurovascular relationship; CT chest for staging
- Confirm diagnosis and grade on expert pathology with exclusion panel
- Plan resection margins and reconstruction; counsel the patient
- En bloc wide excision through normal tissue, including the biopsy track
- Aim for a clear margin (a fascial or anatomical barrier counts as a margin)
- Preserve major neurovascular structures when oncologically safe
- Reconstruct soft-tissue defect (flap coverage) as needed
- Adds local control for large, deep, high-grade extremity tumours
- Preoperative: lower dose, smaller field, but more acute wound complications
- Postoperative: higher dose, larger field, more late fibrosis and stiffness
- Choice individualised at MDT based on size, site and reconstruction plan
- Not routine; considered for large high-grade deep extremity tumours
- UPS shows some chemosensitivity (anthracycline / ifosfamide based)
- Discuss within MDT and ideally a clinical trial
- Intralesional: through the tumour - unacceptable, gross disease remains
- Marginal: through the reactive pseudocapsule - microscopic disease likely, high recurrence
- Wide: through normal tissue around the tumour - the goal for UPS
- Radical: removal of the whole compartment - rarely needed with modern radiotherapy
A wide margin (a cuff of normal tissue or an intact anatomical barrier such as fascia) combined with radiotherapy gives good local control while preserving the limb.
- Lower dose (around 50 Gy), smaller treatment volume
- More acute wound-healing complications (roughly double in the randomised trial)
- Less late fibrosis and better long-term function
- Easier to define the target before surgery distorts anatomy
- Higher dose (around 60-66 Gy), larger volume to cover the surgical bed
- Fewer acute wound problems
- More late fibrosis, oedema, joint stiffness and fracture risk
- Allows full pathological assessment of margins before treatment
Complications and Outcomes
Complications
- Setting
- Inadequate margins, high-grade tumour
- Management
- Re-excision with wider margins, radiotherapy
- Setting
- High-grade, large, deep tumours
- Management
- Metastasectomy if oligometastatic, systemic therapy
- Setting
- After preoperative radiotherapy especially
- Management
- Vigilant wound care, flap coverage, delayed closure
- Setting
- After postoperative radiotherapy
- Management
- Physiotherapy; fracture risk in irradiated bone
- Setting
- Osteosarcoma-type regimens (bone UPS)
- Management
- Significant haematologic and organ toxicity - supportive care
Prognosis and Surveillance
- Lower grade within the high-grade category
- Small size (under 5 cm)
- Superficial rather than deep tumour
- Wide negative margins at resection
- Extremity rather than axial or retroperitoneal site
- No metastases at presentation
- High grade with necrosis and high mitotic count
- Large size (over 5 cm, and especially over 10 cm)
- Deep location
- Positive or close margins
- Retroperitoneal / axial site (wide margins hard to achieve)
- Older age and metastatic disease
High-grade UPS recurs and metastasises mainly in the first 2-3 years, so surveillance is most intensive early: clinical review with imaging of the primary site and CT chest every few months for the first 2-3 years, then less frequently out to 5-10 years. The lung is the dominant site of metastasis, so chest surveillance is essential. Intensity is tailored to grade, size and margin status.
Clinical Relevance and Controversies
As immunohistochemistry and molecular testing improve, more "UPS" is reclassified to definable entities (dedifferentiated liposarcoma, leiomyosarcoma, MPNST). Whether a true lineage-negative UPS is a distinct biological disease or simply the current limit of our diagnostic tools is debated.
Preoperative and postoperative radiotherapy give similar local control and survival, but trade acute wound complications (preop) against late fibrosis (postop). The "right" choice is individualised, not settled.
The survival benefit of chemotherapy for localised soft-tissue UPS is modest and contested; it is generally reserved for large, deep, high-grade tumours and trial settings, unlike bone UPS where osteosarcoma-type chemotherapy is standard.
UPS is relatively immune-responsive among sarcomas, and PD-1 blockade has produced responses in early trials, but checkpoint inhibition is not yet standard of care and patient selection is unresolved.
Guidelines, Registries & Global Practice
Global Epidemiology
Undifferentiated pleomorphic sarcoma is one of the most common adult soft-tissue sarcomas worldwide, even after the reclassification of many former MFH cases. It is strongly age-associated, peaking in the 6th-7th decade, with the deep soft tissue of the thigh the commonest site. Primary UPS of bone is rare, falling within the group of rare primary malignant bone sarcomas (RPMBS) that together make up 5-10% of high-grade bone tumours (EURO-B.O.S.S.).
Society Guidance, Side by Side
- Diagnostic stance
- UPS is defined by exclusion after IHC/molecular workup; replaces 'MFH'
- Treatment emphasis
- Grade-based risk stratification; defines the entity rather than therapy
- Diagnostic stance
- Mandatory expert sarcoma pathology review at a reference centre
- Treatment emphasis
- Wide excision plus radiotherapy for extremity tumours; chemo selective and case-by-case
- Diagnostic stance
- Referral to a designated sarcoma diagnostic and treatment centre (network model)
- Treatment emphasis
- MDT-directed wide excision and limb salvage with radiotherapy for local control
- Diagnostic stance
- Pleomorphic soft-tissue sarcoma managed on the soft-tissue sarcoma pathway; bone UPS on the osteosarcoma pathway
- Treatment emphasis
- Wide resection plus radiotherapy (soft tissue); osteosarcoma-type chemo for bone UPS
- Diagnostic stance
- Pre-treatment biopsy along an excisable track planned with the resecting surgeon
- Treatment emphasis
- Reconstruction and stable fixation after wide resection of bone tumours
Registries and Evidence Networks
- Cooperative trial groups (EURO-B.O.S.S., COSS, EORTC and SARC networks) pool these relatively uncommon tumours to generate the prospective evidence base for chemotherapy and radiotherapy.
- Population registries such as SEER provide large-scale incidence, metastasis and survival data that complement single-centre series for a tumour distributed across many institutions.
- There is no implant-survivorship registry endpoint specific to UPS; reconstruction outcomes are extrapolated from general limb-salvage endoprosthesis and allograft data.
High- versus Limited-Resource Practice
- Specialist MSK pathology with full IHC and MDM2/CDK4 molecular testing
- MRI and CT chest staging and access to radiotherapy planning
- Limb salvage with custom endoprostheses or allografts and flap coverage
- Multidisciplinary tumour board and clinical-trial enrolment
- Restricted IHC and molecular testing may force a descriptive "pleomorphic sarcoma" diagnosis
- Late presentation with large tumours is common
- Amputation more often the realistic margin-achieving option than complex reconstruction
- Radiotherapy and chemotherapy access constrain multimodal treatment
Memory Aids
LAMMPWhat You Must Exclude Before Diagnosing UPS
Hook:LAMMP lights up the differentials you must switch off before UPS: Liposarcoma, Adenocarcinoma, Melanoma, Muscle, Peripheral nerve!
GRADESAdverse Prognostic Factors in Pleomorphic Sarcoma
Hook:GRADES grades the danger: Grade, Resection margin, Age, Depth, Enlarged size, Site!
VANISHUPS Immunoprofile (Diagnosis of Exclusion)
Hook:UPS makes the lineage VANISH: only vimentin remains positive, everything specific is negative!
MCQ Practice Points
Q: What defines undifferentiated pleomorphic sarcoma? A: A high-grade pleomorphic sarcoma showing no identifiable line of differentiation after a full immunohistochemistry and molecular workup. It is a diagnosis of exclusion. The only positive marker is the non-specific mesenchymal marker vimentin.
Q: Why was 'malignant fibrous histiocytoma' renamed undifferentiated pleomorphic sarcoma? A: Because the tumour is not histiocytic in origin - the proposed histiocytic cell of origin was disproven. With modern testing, many former MFH cases are reclassified as dedifferentiated liposarcoma, leiomyosarcoma, MPNST and other definable entities; the remaining lineage-negative tumours are called UPS.
Q: What is the single most important entity to exclude before diagnosing UPS, and how? A: Dedifferentiated liposarcoma, by testing for MDM2 and CDK4 amplification (FISH) or overexpression (immunohistochemistry). This is especially important for retroperitoneal pleomorphic tumours.
Q: How do preoperative and postoperative radiotherapy differ for extremity soft-tissue sarcoma? A: Preoperative uses a lower dose (around 50 Gy) and smaller field but causes roughly twice the acute wound complications; postoperative uses a higher dose (around 60-66 Gy) with fewer acute wound problems but more late fibrosis and stiffness. Local control and survival are similar (O'Sullivan, Lancet 2002).
Q: How is primary UPS of bone treated? A: On the high-grade osteosarcoma pathway - neoadjuvant chemotherapy, wide resection, and adjuvant chemotherapy. EURO-B.O.S.S. showed survival comparable to age-matched osteosarcoma with an osteosarcoma-type regimen.
Q: What is the dominant site of metastasis in UPS, and is lymph node spread common? A: The lung is the dominant metastatic site, so CT chest is the key staging investigation. Lymph-node spread is uncommon in soft-tissue sarcoma overall, although UPS is one of the subtypes with a relatively higher (still low) nodal risk.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 64-year-old man presents with a deep, firm, painless mass in the anterior thigh that has slowly enlarged over 6 months. It is now 9 cm and fixed to the deep tissues. His GP is about to arrange a list to 'shell it out'. How would you manage this patient?”
“A pathology report from another hospital labels a resected pleomorphic sarcoma as 'malignant fibrous histiocytoma'. The trainee asks you what this means and whether the diagnosis can be trusted. How do you respond?”
“A 45-year-old presents with progressive knee pain. Radiographs show a lytic, permeative, destructive lesion in the distal femur with no mineralised matrix. Biopsy reports a high-grade pleomorphic sarcoma with no osteoid and a negative lineage panel - primary undifferentiated pleomorphic sarcoma of bone. How would you manage this?”
Key Features
- High-grade pleomorphic sarcoma with NO line of differentiation - diagnosis of exclusion
- Formerly 'malignant fibrous histiocytoma' (MFH) - histiocytic origin disproven
- One of the most common adult soft-tissue sarcomas; peaks in the 6th-7th decade
- Deep thigh the commonest site; also retroperitoneum and primary bone
- Complex karyotype, no single recurrent translocation
Histology and Diagnosis
- Pleomorphic cells, bizarre giant cells, storiform pattern (classic but not specific)
- Vimentin positive; cytokeratin, S100/SOX10, desmin, SMA all negative
- MUST exclude dedifferentiated liposarcoma with MDM2/CDK4
- Also exclude leiomyosarcoma, MPNST, melanoma, sarcomatoid carcinoma
- Expert MSK pathology review essential
Imaging and Staging
- MRI of primary with contrast: large deep heterogeneous mass, necrosis (T1 low, T2 high)
- CT chest mandatory - lung is the dominant metastatic site
- Lymph-node spread uncommon (but UPS relatively higher than most subtypes)
- Bone UPS: lytic permeative lesion with NO mineralised matrix
- Whole-bone MRI for skip lesions in bone UPS
Biopsy Principles
- Image-guided core needle biopsy preferred
- Track must be excisable at definitive surgery (longitudinal in a limb)
- Coordinate with the sarcoma surgeon - never an unplanned excision
- Sample enhancing viable areas, avoid necrosis
- Full IHC and molecular panel on the cores
Treatment
- Soft-tissue UPS: wide local excision plus radiotherapy for local control
- Preop RT - lower dose, more acute wound problems; postop RT - higher dose, more late fibrosis
- Chemotherapy selective for large, deep, high-grade soft-tissue tumours
- Bone UPS: osteosarcoma pathway (neoadjuvant chemo, wide resection, adjuvant chemo)
- Metastatic: metastasectomy for oligometastatic lung disease; immunotherapy under study
Prognosis and Surveillance
- Adverse factors: high grade, size over 5 cm, deep, positive margins, axial site, older age
- Localised high-grade UPS ~60-70% 5-year survival; bone UPS ~70% (EURO-B.O.S.S.)
- Lung is the dominant metastatic site
- Most recurrence and metastasis within the first 2-3 years
- Surveillance: clinical and imaging of primary plus CT chest, intensive early then tapering
Evidence Base and Key Studies
Preoperative versus Postoperative Radiotherapy in Soft-Tissue Sarcoma of the Limbs: A Randomised Trial
- Multicentre randomised trial of 190 adults with limb soft-tissue sarcoma allocated to preoperative (50 Gy) or postoperative (66 Gy) external-beam radiotherapy
- Wound complications within 120 days occurred in 35% of the preoperative group versus 17% of the postoperative group (difference 18%, p=0.01)
- Larger tumour size and lower-limb site were also significant risk factors for wound complications
- Overall survival was marginally better with preoperative radiotherapy (p=0.0481)
- Establishes that radiotherapy timing trades higher acute wound complications (preop) against higher dose and later toxicity (postop)
Outcome of Rare Primary Malignant Bone Sarcoma Treated With Multimodal Therapy (EURO-B.O.S.S.)
- Prospective European study of 113 patients aged 41-65 with high-grade spindle cell, pleomorphic or vascular bone sarcoma; 88 were undifferentiated pleomorphic sarcoma (UPS)
- Treated with an osteosarcoma-type regimen (doxorubicin, ifosfamide, cisplatin; methotrexate added for poor responders)
- 5-year overall survival 68.4% for localised disease overall, and 71.7% specifically for UPS
- Better survival with localised disease, complete surgical remission and extremity location
- Grade III-IV haematologic toxicity in 81% of patients - the regimen is intensive
Pembrolizumab in Advanced Soft-Tissue and Bone Sarcoma (SARC028): A Multicentre, Two-Cohort, Single-Arm, Phase 2 Trial
- Phase 2 trial of pembrolizumab in 84 patients with advanced soft-tissue or bone sarcoma across 12 US centres
- Among soft-tissue sarcomas, 4 of 10 patients (40%) with undifferentiated pleomorphic sarcoma achieved an objective response
- Responses were also seen in dedifferentiated liposarcoma, while leiomyosarcoma showed none
- The prespecified overall response endpoint was not met for either cohort, but UPS and dedifferentiated liposarcoma showed encouraging activity
- Immune-related serious adverse events included pneumonitis and adrenal insufficiency
Surgical Resection of the Primary Tumour in the Extremities Improves Survival for Metastatic Soft-Tissue Sarcoma: A SEER Population-Based Study
- SEER analysis of 1453 patients presenting with metastatic extremity soft-tissue sarcoma between 1983 and 2016
- After propensity-score matching, primary tumour resection was associated with improved cancer-specific survival (HR 0.59) and overall survival (HR 0.60)
- The survival benefit held for undifferentiated pleomorphic sarcoma specifically (cancer-specific survival HR 0.60, overall survival HR 0.61)
- High-grade tumours, leiomyosarcoma and synovial sarcoma also benefited from primary resection
- Supports considering primary resection even in selected metastatic UPS
Pan-Soft-Tissue Sarcoma Analysis of Incidence, Survival and Metastasis: A SEER Population-Based Study
- SEER study of 35,987 soft-tissue sarcoma patients diagnosed 2000-2018
- Distant metastasis was present in 11.9% and isolated lymph-node metastasis in only 3.4%, confirming nodal spread is uncommon in soft-tissue sarcoma
- Undifferentiated pleomorphic sarcoma was among the subtypes with a higher relative risk of lymph-node metastasis
- Larger tumour size and axial sites (head and neck, viscera, retroperitoneum) carried higher metastatic risk
- Patients with isolated nodal disease fared better than those with distant metastasis but worse than node-negative patients