ASPSCR1-TFE3 Sarcoma of Young Adults
- ALVEOLAR SOFT PART SARCOMA (ASPS) is a RARE soft-tissue SARCOMA, most often of ADOLESCENTS and YOUNG ADULTS, characterised by a specific genetic abnormality - the ASPSCR1-TFE3 (ASPL-TFE3) GENE FUSION - which produces nuclear TFE3 over-expression that is a hallmark diagnostic marker (confirmed by immunohistochemistry/molecular testing).
- It typically presents as a PAINLESS, SLOW-GROWING, DEEP soft-tissue mass - commonly in the lower limb/thigh in adults (and the head and neck in children) - and is often highly VASCULAR; because it is painless and indolent, it may grow for a long time and is sometimes diagnosed only after METASTASIS is found.
- The defining clinical paradox is that, despite an INDOLENT slow-growing PRIMARY, ASPS has a STRIKING propensity for EARLY HAEMATOGENOUS METASTASIS - to the LUNG (most common), BONE and characteristically the BRAIN - so staging must include the chest and brain, and LATE metastases (years later) occur, mandating long-term surveillance.
- HISTOLOGY is distinctive: ALVEOLAR/ORGANOID nests of large, polygonal, eosinophilic/granular cells separated by thin-walled sinusoidal vascular channels, with characteristic PAS-POSITIVE, diastase-RESISTANT intracytoplasmic CRYSTALS (rod/rhomboid shaped); the diagnosis is confirmed by nuclear TFE3 immunostaining and/or detection of the ASPSCR1-TFE3 fusion (e.g. on next-generation sequencing).
- DIAGNOSIS and STAGING follow soft-tissue-sarcoma principles: MRI of the primary, a properly PLANNED BIOPSY at the treating sarcoma unit, and STAGING that specifically includes the LUNGS and the BRAIN given the metastatic pattern - an unplanned excision of an undiagnosed deep mass must be avoided.
- MANAGEMENT: WIDE surgical RESECTION of the primary is the mainstay in LOCALISED disease, as ASPS is relatively CHEMO-RESISTANT and doxorubicin-based chemotherapy showed no survival benefit in a 120-patient registry. Metastasectomy is offered for resectable deposits but did NOT improve survival in that registry (a comparison confounded by indication) - so do not promise a survival gain from it. PAZOPANIB was associated with prolonged survival and IMMUNOTHERAPY (checkpoint inhibitors) is also active in advanced disease. LONG-TERM SURVEILLANCE of chest and brain is essential because 45 percent of even localised cases metastasise - all within a specialist sarcoma multidisciplinary team.
- “ASPS = rare soft-tissue sarcoma of YOUNG ADULTS; defining ASPSCR1-TFE3 fusion (nuclear TFE3). Painless, slow-growing, deep, vascular limb mass.
- “Paradox: indolent primary but EARLY HAEMATOGENOUS metastasis (LUNG, bone, BRAIN) - stage the chest AND brain; late metastases occur (long-term surveillance).
- “Histology: alveolar/organoid nests + PAS-positive diastase-resistant crystals; TFE3 nuclear stain. CHEMO-RESISTANT -> wide resection (+ metastasectomy); anti-angiogenic TKIs/immunotherapy for advanced disease. Sarcoma-centre care.
Young adult with a painless, slow-growing, deep, vascular limb mass. Histology: alveolar/organoid nests + PAS-positive crystals; nuclear TFE3 / ASPSCR1-TFE3 fusion.
Early haematogenous metastasis - lung, bone, BRAIN - despite an indolent primary. Stage the chest and brain; expect late metastases (long-term surveillance).
Diagnosis, Staging & Management
- Diagnosis: MRI of the primary; planned biopsy at the treating sarcoma unit; nuclear TFE3 / ASPSCR1-TFE3 confirmation.
- Staging: include the lungs and the brain (characteristic metastatic sites).
- Surgery: wide resection of the primary is the mainstay for localised disease. Metastasectomy is offered for resectable deposits, but be careful how it is justified: in a 120-patient national registry, surgery for the primary or the metastatic site did not affect survival in patients who were already metastatic. That comparison is confounded by indication, so it is not a reason to withhold an operation from a patient who will benefit symptomatically or from oligometastatic control - it is a reason not to promise a survival gain.
- Systemic therapy: ASPS is chemo-resistant - doxorubicin-based chemotherapy showed no survival benefit in that registry, whereas pazopanib did (p = 0.045). Immune checkpoint inhibitors are also active in advanced disease.
- Adjuvant treatment in localised disease did not improve survival in the same registry, and 45 percent metastasised anyway - so adjuvant chemotherapy or radiotherapy is not a substitute for surveillance.
- Surveillance: long-term follow-up because of late metastasis, covering the chest and brain; specialist sarcoma MDT throughout.
The defining management lesson in alveolar soft part sarcoma is that the indolent appearance of the primary tumour is dangerously misleading. ASPS grows slowly and is painless, so it can be under-estimated, yet it has a striking propensity for early haematogenous metastasis to the lungs, bone and characteristically the brain - so staging must explicitly include chest and brain imaging, and the patient needs long-term surveillance because metastases can appear years later. Treatment is also different from many sarcomas: it is relatively resistant to conventional cytotoxic chemotherapy, so wide surgical resection is the mainstay in localised disease, while pazopanib and immune checkpoint inhibitors are the active systemic options in advanced disease. Metastasectomy is offered for resectable deposits, but a national registry could not show that surgery for the primary or the metastatic site improved survival once metastases were present - a finding confounded by indication, and one that argues for honest counselling rather than for withholding an operation. As with all soft-tissue sarcomas, an unplanned excision of an undiagnosed deep mass compromises the oncological outcome, so a suspicious deep, slow-growing, vascular mass in a young adult should be imaged, biopsied in a planned way, and managed at a specialist sarcoma centre.
The Translocation and the TFE3 (Xp11) Family
- The translocation. ASPS is defined by an unbalanced translocation, der(17)t(X;17)(p11.2;q25), fusing ASPSCR1 (ASPL) on chromosome 17q25 to TFE3 on chromosome Xp11.2. The chimeric protein acts as an aberrant transcription factor that up-regulates MET signalling and angiogenesis - which is why the tumour is so vascular (and why anti-angiogenic TKIs work).
- The diagnostic marker. Because the fusion drives strong TFE3 expression, the tumour shows strong nuclear TFE3 immunostaining - sensitive but not fully specific (other TFE3-rearranged tumours also stain), so FISH or next-generation sequencing for the fusion confirms it.
- The TFE3/Xp11 family. The same TFE3 (Xp11.2) locus is rearranged in the Xp11 translocation renal cell carcinomas and in a TFE3-rearranged PEComa group - all nuclear-TFE3-positive - so a TFE3-positive tumour must be placed in clinical and morphological context.
Q: What is the defining genetic abnormality of ASPS, and how is it detected?
A: ASPS is defined by an unbalanced translocation, der(17)t(X;17)(p11.2;q25), fusing ASPSCR1 (ASPL) on 17q25 to TFE3 on Xp11.2; the chimeric protein drives MET signalling and angiogenesis (the hypervascularity). It produces strong nuclear TFE3 immunostaining - sensitive but not specific - confirmed by FISH/NGS for the fusion. The same TFE3/Xp11.2 locus is rearranged in Xp11 translocation renal cell carcinoma and TFE3-rearranged PEComa, so nuclear TFE3 is shared across that family.
Presentation, Histology & Behaviour
ASPS is a rare soft-tissue sarcoma of young adults defined by the ASPSCR1-TFE3 gene fusion (nuclear TFE3). It presents as a painless, slow-growing, deep, vascular mass (lower limb/thigh in adults; head/neck in children) and may be found late or via metastasis. Its hallmark is early haematogenous metastasis to the lung, bone and brain despite the indolent primary, with late metastases occurring. Histology shows alveolar/organoid nests of large eosinophilic cells with PAS-positive, diastase-resistant crystals, and the diagnosis is confirmed by nuclear TFE3 staining and/or the ASPSCR1-TFE3 fusion.
What the PAS Crystals Are, and the Histological Differential
- What the crystals are. The pathognomonic PAS-positive, diastase-resistant, rod- or rhomboid-shaped intracytoplasmic crystals are membrane-bound crystalline aggregates of the monocarboxylate transporter MCT1 and its chaperone CD147 (EMMPRIN) - the specific morphological clue to ASPS.
- The histological differential. The organoid nests of large granular/eosinophilic cells mimic several tumours, separated by immunostains:
- Metastatic renal cell carcinoma (clear/granular) - keratin/PAX8-positive; ASPS is keratin-negative.
- Paraganglioma - chromogranin/synaptophysin-positive (neuroendocrine); ASPS is negative.
- Granular cell tumour - S100-positive; ASPS is S100-negative.
- PEComa / melanoma - HMB45 / Melan-A-positive; ASPS is negative.
- Adrenal cortical carcinoma - inhibin/SF1-positive.
- The clincher. ASPS is characteristically negative for keratin, S100, chromogranin and melanocytic markers and positive for nuclear TFE3, with the PAS-positive crystals and the ASPSCR1-TFE3 fusion.
Q: What are the PAS-positive crystals in ASPS, and how do you distinguish it histologically?
A: The pathognomonic PAS-positive, diastase-resistant rod/rhomboid crystals are crystalline aggregates of the monocarboxylate transporter MCT1 with its chaperone CD147. The organoid granular-cell pattern mimics metastatic RCC (keratin/PAX8-positive), paraganglioma (chromogranin-positive), granular cell tumour (S100-positive) and PEComa/melanoma (HMB45-positive); ASPS is negative for all of these and positive for nuclear TFE3 with the crystals and the ASPSCR1-TFE3 fusion, which clinches it.

The Numbers Behind the Paradox - and What Did Not Change Survival
"A striking propensity for early metastasis" understates it, and the survival figures are more favourable than the phrase implies. A national registry of 120 patients puts both halves in proportion.
Of 120 newly diagnosed patients, only 34 (28 percent) had localised disease - 86 (72 percent) were already metastatic at presentation. Yet survival is far better than that implies: 5-year disease-specific survival was 68 percent overall - 86 percent localised against 62 percent metastatic, and a separate institutional series reported 74 percent at 5 years and 51 percent at 10. Metastasis at presentation was the ONLY adverse prognostic factor (hazard ratio 7.65). Metastases were already present more often in patients over 25 years (80 percent), with deep-seated tumours (75 percent) and with tumours larger than 5 cm (81 percent) - so the "young adult" framing should not lower suspicion in an older patient with a large deep mass.
Three negative findings deserve stating as measured. In localised disease, adjuvant chemotherapy or radiotherapy did not affect survival, and 13 of the 29 followed (45 percent) still developed distant metastases - to lung in 12 (92 percent) and brain in 2 (15 percent). In metastatic disease, surgery for the primary or for the metastatic site did not affect survival. And doxorubicin-based cytotoxic chemotherapy showed no survival benefit, whereas pazopanib was associated with prolonged survival (p = 0.045). These are retrospective registry comparisons, heavily confounded by indication - the fittest patients with the most resectable disease get the operation - so they are not an argument against operating; they are an argument against promising a survival benefit from metastasectomy that the data do not show.
The page-level claim that anti-angiogenic tyrosine-kinase inhibitors "have activity" is worth making specific: pazopanib is the agent with a survival signal in that registry, and the underlying rationale is measured - an angiogenesis oligoarray found 18 angiogenesis-related genes up-regulated in ASPS compared with adjacent normal tissue, with an angiogenic signature the authors described as unique among sarcomas. Disease-specific survival for metastatic disease did improve after 2012, when pazopanib became available, from 58 to 65 percent - but that difference was not statistically significant (p = 0.117), so it is a trend and should be quoted as one. Immune checkpoint inhibitors are also active in advanced disease; no head-to-head comparison against a tyrosine-kinase inhibitor was retrieved.
Carry these: 72 percent are metastatic at presentation, yet 5-year disease-specific survival is 68 percent (86 percent localised, 62 percent metastatic) and 10-year around 51 percent - an indolent course with treatment-resistant metastases driving eventual mortality. Metastasis at presentation is the only independent adverse factor (HR 7.65). Even with localised disease, 45 percent go on to metastasise, which is what mandates surveillance measured in years rather than months.
Mnemonics & Memory Aids
ALVEOLAR
Hook:ALVEOLAR: ASPSCR1-TFE3, Limb deep mass, Very vascular, Early lung/bone/brain metastasis, Organoid + crystals, Long-term surveillance, Anti-angiogenic/immunotherapy, Resect widely (chemo-resistant).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A young adult has a slow-growing, painless, vascular thigh mass, and biopsy shows an alveolar pattern with PAS-positive crystals. What is the diagnosis, and what is critical in management?”
What it is
- Rare soft-tissue sarcoma of adolescents/young adults
- Defining ASPSCR1-TFE3 (ASPL-TFE3) gene fusion -> nuclear TFE3
- Painless, slow-growing, deep, vascular mass (thigh in adults; head/neck in children)
Behaviour
- Indolent primary BUT early haematogenous metastasis
- Lung (most common), bone, and characteristically the brain
- Late metastases occur - long-term surveillance
Diagnosis
- Alveolar/organoid nests; PAS-positive, diastase-resistant crystals
- Nuclear TFE3 immunostain; ASPSCR1-TFE3 fusion (NGS)
- MRI primary + planned biopsy; stage chest AND brain
Management
- Chemo-resistant -> wide resection of the primary is the mainstay (localised disease)
- PAZOPANIB had a survival signal; doxorubicin did not. Checkpoint inhibitors also active
- Metastasectomy for resectable deposits did NOT improve survival in registry data (confounded) - counsel honestly
- 72% metastatic at presentation; 5-yr DSS 68% (86% localised / 62% metastatic), 10-yr ~51%
- 45% of localised cases still metastasise - long-term chest AND brain surveillance; sarcoma MDT
Evidence & Key Studies
Alveolar soft part sarcoma with ASPSCR1-TFE3 gene fusion
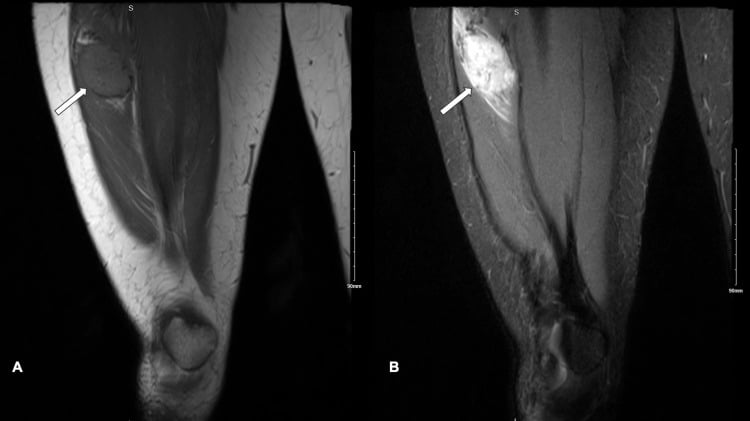
- Alveolar soft part sarcoma is an extremely rare disease characterised by the specific ASPSCR1-TFE3 gene fusion, confirmed in this case by next-generation sequencing.
- Histology showed the characteristic tumour cells - polygonal cells with abundant eosinophilic or transparent cytoplasm arranged in nests (the alveolar/organoid pattern).
- Management centred on surgical resection with close follow-up, reflecting the importance of detailed diagnosis, prompt treatment and monitoring in ASPS.
National registry of 120 patients: 72 percent metastatic at presentation, and what did not change survival
- 120 newly diagnosed patients from the Bone and Soft-Tissue Tumor Registry in Japan, 2006 to 2017, analysed retrospectively: 34 (28 percent) localised and 86 (72 percent) metastatic AT PRESENTATION.
- Five-year disease-specific survival was 68 percent overall - 86 percent for localised and 62 percent for metastatic disease (p = 0.019).
- Metastasis at presentation was the ONLY adverse prognostic factor (hazard ratio 7.65, p = 0.048); metastases were commoner in patients over 25, with deep-seated tumours and with tumours over 5 cm.
- In localised disease, adjuvant chemotherapy or radiotherapy did NOT affect survival, and 45 percent still developed distant metastases (lung 92 percent, brain 15 percent).
- In metastatic disease, surgery for the primary or the metastatic site did NOT affect survival; pazopanib was associated with prolonged survival (p = 0.045) whereas doxorubicin-based chemotherapy was not.
- Disease-specific survival for metastatic disease rose from 58 to 65 percent after 2012 when pazopanib was approved, but the difference was NOT significant (p = 0.117).
- Retrospective national registry from a single country; the surgical comparisons are confounded by indication and cannot be read as evidence against operating.
Angiogenic gene signature and long-term survival in 71 patients
- Records of 71 patients treated at a single cancer centre between 1986 and 2005, with 33 having tissue available for molecular study.
- Actuarial survival was 74 percent at 5 years and 51 percent at 10 years despite frequent metastasis - the authors describe a highly vascular and metastatic tumour with a surprisingly favourable outcome, in which therapeutically resistant metastases drive mortality.
- The ASPSCR1-TFE3 fusion transcript was identified in 16 of 18 samples tested.
- An angiogenesis oligoarray found 18 angiogenesis-related genes up-regulated in tumour compared with adjacent normal tissue, confirmed for jag-1, midkine and angiogenin, with a signature the authors judged unique among sarcomas - the measured basis for targeting angiogenesis.
- Single-centre retrospective series spanning two decades, with molecular work on only three frozen samples for the array.
The defining ASPSCR1-TFE3 gene fusion (confirmed by next-generation sequencing), the characteristic alveolar/organoid histology (polygonal eosinophilic cells in nests), and the central role of surgical resection with close follow-up come from the cited Hu report. The young-adult demographic, the painless vascular deep-mass presentation, the PAS-positive diastase-resistant crystals and nuclear TFE3 marker, the striking early haematogenous metastasis to lung/bone/brain (with late metastases and long-term surveillance), the chemo-resistance, and the activity of anti-angiogenic TKIs and immunotherapy in advanced disease are standard, well-established teaching. The proportion metastatic at presentation, the survival figures, the hazard ratio for metastasis at presentation, the pazopanib signal and the three negative findings (no survival effect from adjuvant therapy in localised disease, from surgery in metastatic disease, or from doxorubicin) come from the cited Fujiwara national registry - a retrospective, single-country series whose surgical comparisons are confounded by indication. The 5- and 10-year survival figures and the measured angiogenic gene signature come from the cited Lazar series, a single centre spanning 1986 to 2005 with array work on only three frozen samples. No randomised trial in this disease was retrieved, and no evidence-based surveillance interval or duration specific to alveolar soft part sarcoma was found - so the recommendation for prolonged chest and brain imaging is given on the metastatic pattern rather than on a validated schedule, and intervals should follow local sarcoma protocol. See also soft-tissue masses and sarcoma referral and biopsy principles and techniques; the library has no dedicated metastasectomy topic.