Pars Defect | Spondylolysis | L5-S1 Slip
- PARS DEFECT (spondylolysis) distinguishes from degenerative type
- L5-S1 most common level (90%) vs L4-5 for degenerative
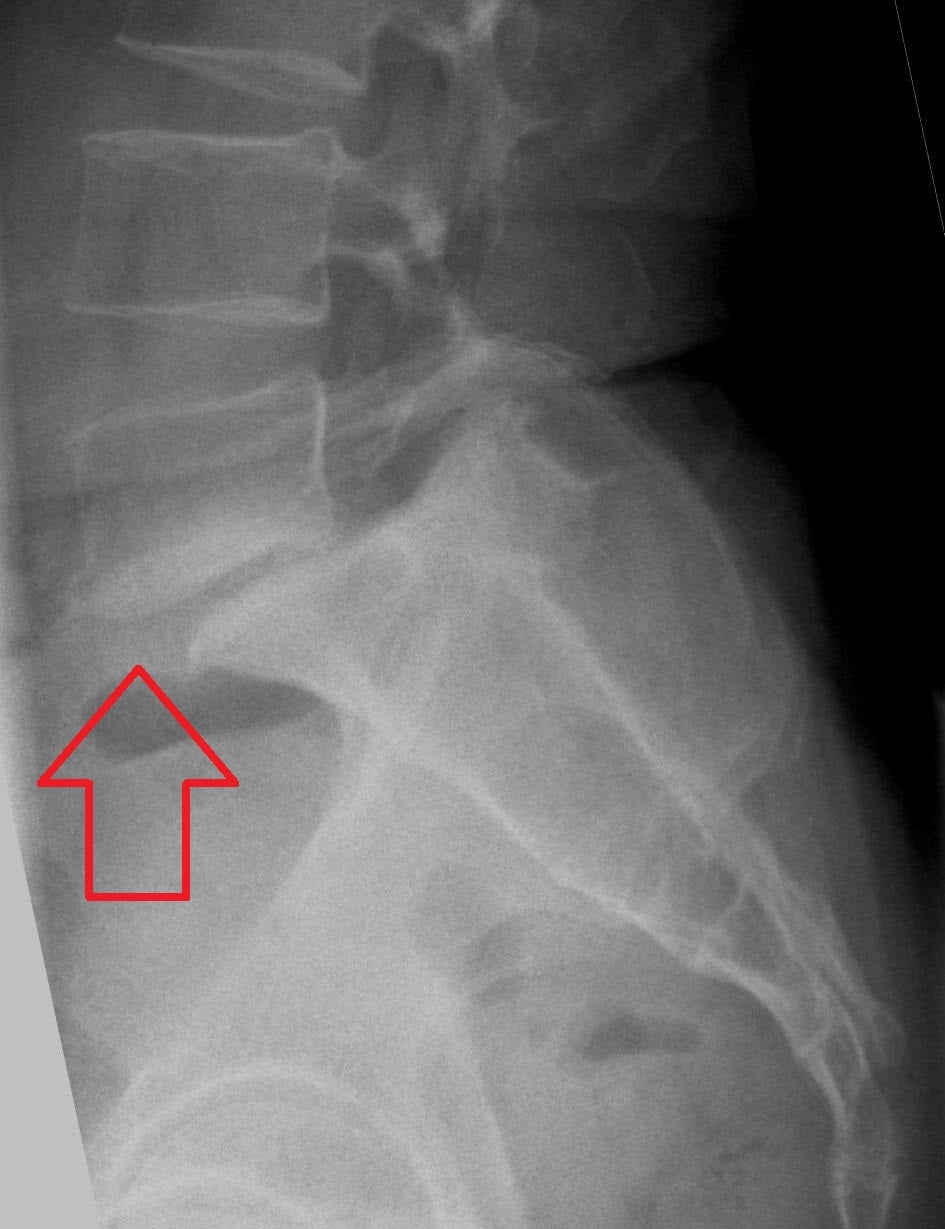
- Scottie dog collar sign on oblique X-ray shows pars defect
- 80% asymptomatic - most patients never need surgery
- CT is gold standard for pars defect visualization
- “Young athlete with extension-related back pain = think pars stress reaction
- “Hamstring tightness common in adolescents with spondylolisthesis
- “High-grade slips may have waddling gait and heart-shaped sacrum
- “SPECT-CT shows metabolic activity in acute/healing pars defect
Isthmic has PARS DEFECT - spondylolysis present on imaging. Occurs at L5-S1 (90%). Young patients (adolescence). Degenerative has NO pars defect, occurs at L4-L5 (70%), older patients.
On oblique X-ray, the posterior elements form a "Scottie dog". The pars defect appears as a "collar" across the dog's neck. CT is more sensitive and specific for pars visualization.
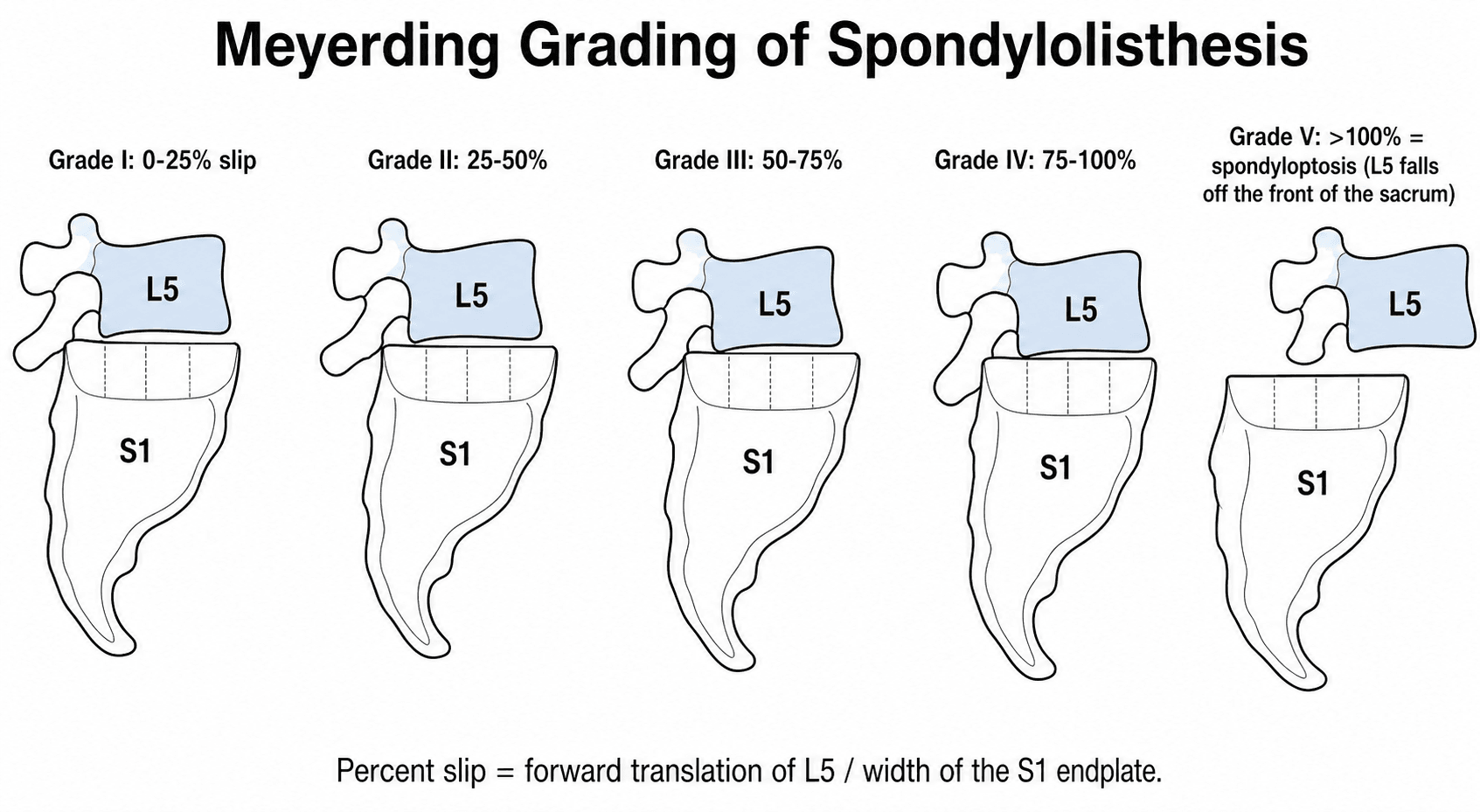
Grade I: Less than 25% slip. Grade II: 25-50%. Grade III: 50-75%. Grade IV: 75-100%. Grade V (Spondyloptosis): Greater than 100% slip. Low-grade (I-II), High-grade (III-V).
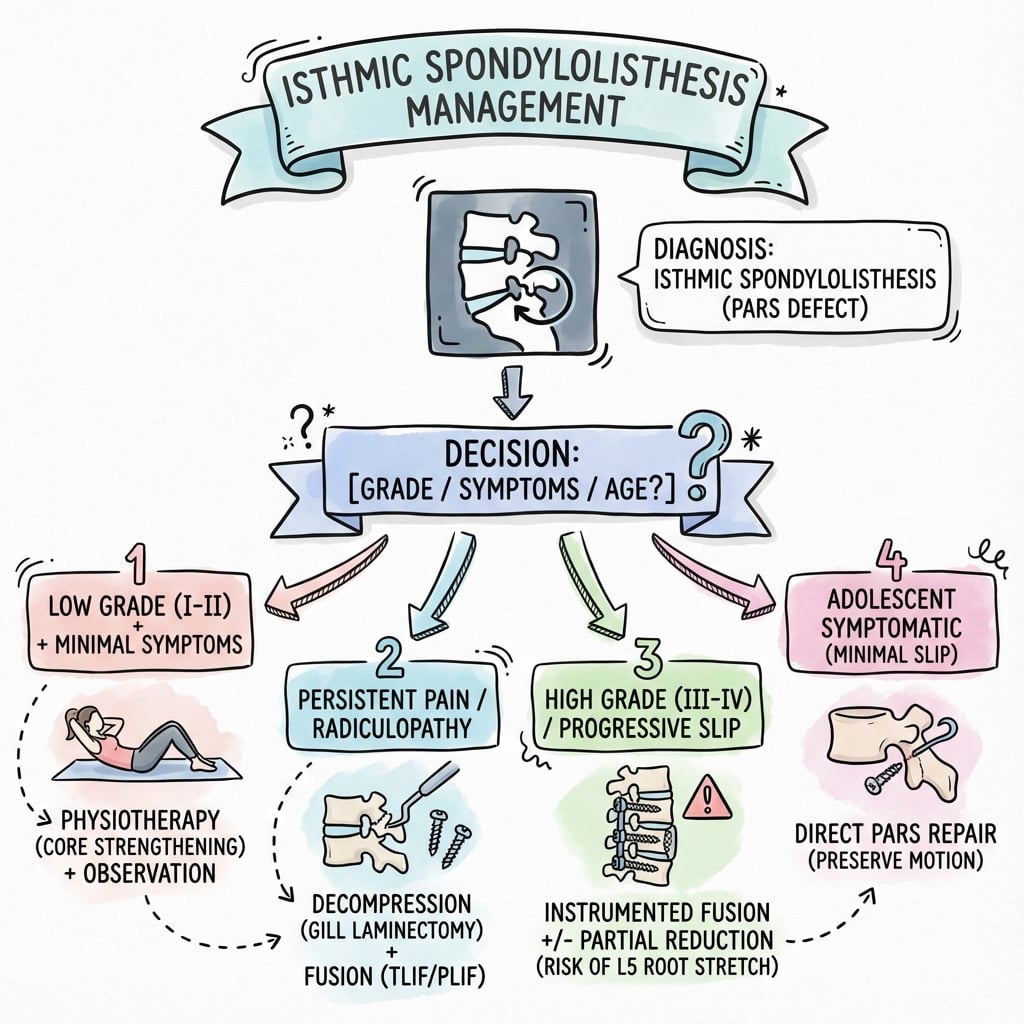
Most are asymptomatic - observation only. Conservative first for symptomatic (physio, activity mod). Surgery if: failed conservative, progressive slip, neurological deficit, high-grade slip.
- Isthmic
- DEFECT present (spondylolysis)
- Degenerative
- Intact (no defect)
- Isthmic
- L5-S1 (90%)
- Degenerative
- L4-L5 (70%)
- Isthmic
- Adolescence/young adult
- Degenerative
- Over 50 years
- Isthmic
- Male predominant (3:1)
- Degenerative
- Female predominant (6:1)
- Isthmic
- Stress fracture of pars
- Degenerative
- Facet and disc degeneration
- Isthmic
- Any grade (up to spondyloptosis)
- Degenerative
- Usually Grade I-II only
- Isthmic
- Pars repair or fusion
- Degenerative
- Decompression with or without fusion
Overview and Epidemiology
Isthmic Spondylolisthesis is forward slippage of a vertebra due to a defect (spondylolysis) or elongation of the pars interarticularis. It is the most common type of spondylolisthesis in patients under 50 years.
Definition:
Spondylolysis refers to a defect in the pars interarticularis (the bony bridge between the superior and inferior articular processes). Spondylolisthesis is forward displacement of one vertebra on another. Isthmic spondylolisthesis occurs when spondylolysis allows this slip.
Epidemiology:
- Details
- 6% of general population
- Details
- Only 20% become symptomatic
- Details
- L5-S1 (90%), L4-L5 (5-10%)
- Details
- Adolescence (15-25 years)
- Details
- Male predominant 3:1
- Details
- Gymnastics, football linemen, weightlifting, cricket fast bowlers
Natural History:
Most patients with pars defects remain asymptomatic throughout life. Progression of slip is most likely in childhood/adolescence and typically stabilizes after skeletal maturity.
Anatomy and Biomechanics
Pars Interarticularis
Anatomical Location:
The pars interarticularis is the portion of the lamina between the superior and inferior articular processes. It is the thinnest and weakest part of the neural arch.
- Relationship
- Inferior margin of superior articular facet
- Relationship
- Superior margin of inferior articular facet
- Relationship
- Lamina
- Relationship
- Transverse process
Why L5?
L5 is predisposed because:
- Maximum lordosis and shear stress at L5-S1
- Orientation of L5 facets resists forward slip less effectively
- Highest compressive and shear loads during extension
- Pars at L5 is anatomically thinner
Biomechanics of Slip
Load Distribution:
The posterior elements (facets, pars) normally resist 25-30% of axial load. When the pars is deficient, this load transfers to the disc, leading to degeneration and progressive slip.
Slip Angle:
The slip angle (lumbosacral kyphosis) is the angle between L5 and S1. High slip angles indicate more kyphosis at the lumbosacral junction and correlate with worse outcomes.
Pathophysiology
Mechanism of Pars Defect
Type IIA - Lytic/Fatigue Fracture
Repetitive hyperextension causes cyclic loading of the pars. The pars experiences tensile stress on the inferior surface and compressive stress superiorly. Fatigue failure occurs when bone remodeling cannot keep pace with microdamage.
Stage 1 is pars stress reaction with bone edema on MRI. Stage 2 is incomplete fracture with a hairline on CT. Stage 3 is complete fracture with visible defect. Stage 4 is established non-union with sclerotic margins.
Gymnastics, cricket fast bowling, diving, weightlifting, football (linemen).
Progression of Slip
Factors Promoting Progression:
- Impact
- Growth remaining allows progression
- Impact
- Higher progression rates
- Impact
- More likely to progress further
- Impact
- Loss of disc height facilitates slip
- Impact
- Indicates unstable mechanics
Neurological Involvement:
L5 radiculopathy can occur by two mechanisms. First is fibrous tissue or callus at the pars defect compressing the L5 root. Second is foraminal narrowing as the L5 vertebra slides forward and the sacral dome rises posteriorly.
Classification
Wiltse-Newman Classification
Congenital Facet Deficiency
Congenital abnormality of the upper sacrum or L5 arch with hypoplastic facets that allow forward slip without pars defect.
No true pars defect. Facets are hypoplastic or abnormally oriented. Rare, accounts for 5-10% of spondylolisthesis.
Higher risk of cauda equina compression because the posterior elements remain attached and can impinge on the canal.
Meyerding Grading
- Slip Percentage
- Less than 25%
- Description
- Low-grade, usually asymptomatic
- Slip Percentage
- 25-50%
- Description
- Low-grade, may be symptomatic
- Slip Percentage
- 50-75%
- Description
- High-grade, often symptomatic
- Slip Percentage
- 75-100%
- Description
- High-grade, typically symptomatic
- Slip Percentage
- Greater than 100%
- Description
- Spondyloptosis (L5 anterior to S1)
Marchetti-Bartolozzi Classification
A simpler, prognostically useful scheme that separates the two mechanisms most relevant to treatment:
- Subtypes
- High-dysplastic and low-dysplastic
- Key point
- Abnormal sacropelvic morphology, often progressive, higher slip grades
- Subtypes
- Traumatic, post-surgical, pathological, degenerative
- Key point
- Normal anlage; slip results from a discrete insult or wear
Classic adolescent isthmic (lytic) spondylolisthesis is generally regarded as part of the developmental (low-dysplastic) spectrum because of its strong association with abnormal spinopelvic morphology.
Spinopelvic Parameters and the SDSG System
Modern decision-making, especially in high-grade slips, is driven by sagittal alignment rather than slip percentage alone:
- Relevance
- Fixed morphological constant; high PI predisposes to development and progression (Labelle 2004)
- Relevance
- Position-dependent; a high SS / low PT pelvis is "balanced", a low SS / high PT (retroverted) pelvis is "unbalanced"
- Relevance
- Global sagittal balance of the trunk
The Spinal Deformity Study Group (SDSG) classification grades L5-S1 slips by (1) Meyerding grade, (2) pelvic incidence and (3) spinopelvic alignment, producing six types with significantly different quality-of-life profiles. Its main clinical message: an unbalanced (retroverted) high-grade pelvis is the subgroup most likely to benefit from reduction, whereas a balanced pelvis may be managed by in situ fusion.
Clinical Presentation
History
Pain Characteristics:
- Pattern
- Low back, may radiate to buttocks
- Pattern
- Aching, mechanical
- Pattern
- Extension, standing, sports
- Pattern
- Flexion, rest
- Pattern
- L5 if nerve compression
Red Flags:
- Concern
- Cauda equina (rare)
- Concern
- Neurological compromise
- Concern
- High-grade instability
Physical Examination
- Step-off palpable at lumbosacral junction in high-grade
- Increased lumbar lordosis
- Vertical sacrum (spondyloptotic crisis)
- Waddling gait in severe cases
- Tenderness over L5-S1
- Hamstring tightness (common finding)
- Limited lumbar flexion
- Pain with extension
- Stiffness from hamstring spasm
- Root
- L5
- Interpretation
- Stretched over sacral dome
- Root
- S1
- Interpretation
- Less common
- Root
- Cauda equina
- Interpretation
- Emergency
Special Tests:
- Technique
- Stand on one leg, extend
- Positive if
- Reproduces ipsilateral LBP
- Technique
- Popliteal angle, SLR
- Positive if
- Tight hamstrings correlate with slip
- Technique
- Standard testing
- Positive if
- L5 radiculopathy
Tight hamstrings are a classic finding in adolescents with isthmic spondylolisthesis. The mechanism is debated but may relate to protective hamstring spasm and postural compensation for the lumbosacral kyphosis and anterior pelvic tilt produced by the slip.
Differential Diagnosis
Adolescent or young-adult mechanical back pain has several mimics that must be excluded before attributing symptoms to a pars lesion:
- Discriminating features
- Extension pain, single-leg hyperextension positive, hamstring tightness
- Key investigation
- CT / MRI: pars defect ± slip
- Discriminating features
- Older patient, intact pars, L4-5, neurogenic claudication
- Key investigation
- MRI: intact pars, facet arthrosis, stenosis
- Discriminating features
- Flexion-aggravated, positive SLR, dermatomal radiculopathy
- Key investigation
- MRI: focal disc protrusion
- Discriminating features
- Rigid kyphosis, anterior wedging ≥5° over 3 vertebrae
- Key investigation
- Lateral X-ray: endplate irregularity, Schmorl nodes
- Discriminating features
- Inflammatory pattern, morning stiffness, raised CRP, HLA-B27
- Key investigation
- MRI SIJ: bone-marrow oedema; inflammatory markers
- Discriminating features
- Constant night pain, fever, raised CRP/ESR
- Key investigation
- MRI with contrast; CRP, ESR, blood cultures
- Discriminating features
- Night pain relieved by NSAIDs (osteoid osteoma), painful scoliosis
- Key investigation
- CT (nidus) / MRI; bone scan
Investigations
Imaging Protocol
X-ray (First Line):
- Purpose
- Overall alignment, transitional vertebra
- Purpose
- Slip percentage (Meyerding grade), slip angle
- Purpose
- Scottie dog - pars defect (collar sign)
- Purpose
- Instability assessment
Measuring Slip:
Meyerding grading divides the sacral endplate into quarters. Slip percentage is how far the posterior corner of L5 has slipped forward.
CT Scan:
Gold standard for pars defect visualization.
- Finding
- Defect, elongation, sclerosis
- Finding
- Sclerotic margins = low healing potential
- Finding
- Foraminal stenosis, facet arthrosis
MRI:
- Assessment
- Disc degeneration, canal stenosis
- Assessment
- Neural compression, foraminal narrowing
- Assessment
- Bone marrow edema (acute pars stress)
SPECT-CT:
Combines CT anatomy with SPECT metabolic activity. Hot spot at pars indicates acute/healing lesion with potential for conservative healing. Cold defect indicates established non-union.
Laboratory Studies
Not routinely required. If concern for pathologic etiology (Type V), check CBC, ESR, CRP, calcium, phosphate, ALP, and tumor markers if indicated.
Management
Treatment Algorithm
Asymptomatic Spondylolysis/Spondylolisthesis:
Most patients (80%) remain asymptomatic. No treatment required. Activity restrictions not routinely indicated for low-grade slips.
Conservative Management (First Line for Symptomatic):
- Details
- Avoid aggravating extension activities
- Details
- Core strengthening, hamstring stretching
- Details
- Anti-lordotic brace for acute pars stress (healing potential)
- Details
- Symptom control
Duration: 6-12 weeks trial before considering surgery.
Indications for Surgery:
- Comment
- Most common indication
- Comment
- Especially in skeletally immature
- Comment
- L5 radiculopathy
- Comment
- Often require surgery
- Comment
- Quality of life indication
Surgical Options
Direct Pars Repair (Scott, Buck)
Young patient (under 25), low-grade slip, minimal or no disc degeneration, single-level defect.
Scott wiring uses a figure-of-8 wire around transverse process and spinous process. Buck's screw is a lag screw across pars defect.
In carefully selected young patients (healthy disc, no associated slip), radiological union is high and satisfactory functional outcomes are reported in roughly 80% (Rajasekaran, satisfactory in 7/9; an associated Grade 1 slip predicted a poor result). Motion-preserving and avoids fusion.
Significant disc degeneration, an established slip, high-grade slip, multilevel disease, sclerotic (terminal-stage) pars margins.
For high-grade slips, the debate between in situ fusion and reduction continues. In situ is technically safer but may not correct sagittal imbalance. Reduction improves alignment but carries a 10-25% risk of L5 radiculopathy from nerve stretch. The modern, examiner-pleasing answer uses the SDSG spinopelvic framework (Labelle, Mac-Thiong): reserve reduction for high-grade slips with an UNBALANCED (retroverted) pelvis to restore global sagittal balance, rather than reducing every high-grade slip. Always consider patient factors, surgeon experience, and use intraoperative neuromonitoring.
Return to Sport After Athletic Spondylolysis
The topic centres on the young athlete (gymnasts, cricket fast bowlers) and the vivas ask "when can he return to cricket?" and "what modifications to bowling technique?", but the return-to-sport framework is never developed. There is no single validated protocol; management is staged and criteria-based.
- Goal
- Settle pain and protect the pars
- Key elements
- Stop the provocative activity; relative rest; anti-lordotic posture; brace if an early, healable defect
- Goal
- Restore control and flexibility
- Key elements
- Lumbopelvic/core stabilisation, hamstring and hip-flexor flexibility, neutral-spine motor control
- Goal
- Reintroduce load safely
- Key elements
- Graded sport-specific drills once pain-free with restored strength and a normal neurological exam
- Goal
- Prevent recurrence
- Key elements
- Full return when asymptomatic and functionally tested; correct the provocative technique (e.g. the cricket mixed bowling action)
Return to sport is driven by SYMPTOMS and FUNCTION, not by radiographic union. An early stress reaction is managed toward bony healing (Sairyo: early CT-stage defects with adjacent pedicle marrow oedema heal best), but many athletes return successfully with an established (fibrous) defect once they are pain-free with restored core and hamstring function — typically around 3 to 6 months. Whatever the imaging shows, the causative load and technique must be corrected (e.g. converting a mixed fast-bowling action) or the lesion recurs.
Spondyloptosis and the Gaines Vertebrectomy
Grade V (spondyloptosis, more than 100% slip) and the "Gaines vertebrectomy" are named in the grading and high-grade tabs but never developed. Spondyloptosis is the extreme of the developmental spectrum, where L5 has translated completely off the front of S1, and it is always a surgical problem with three broad strategies.
- Description
- Fuse without reducing the slip; a fibular or transsacral dowel can be passed from S1 up into the L5 body
- Note
- Lower neurological risk; accepts the deformity
- Description
- Partial or full reduction with L4-S1 instrumentation and interbody support
- Note
- Restores sagittal balance; higher L5 nerve-stretch risk
- Description
- Two-stage removal of the L5 body (anterior) then its posterior elements, reducing L4 onto S1
- Note
- Reserved for severe spondyloptosis; the highest neurological risk
In spondyloptosis the L5 nerve root is at greatest risk during any reduction or vertebrectomy, so intraoperative neuromonitoring is mandatory and a partial reduction is accepted if motor/sensory evoked potentials or EMG deteriorate. The SDSG balanced-versus-unbalanced pelvis decision still applies — reserve aggressive reduction for the unbalanced (retroverted) pelvis, where restoring global sagittal balance justifies the added risk.
Complications
Conservative Management Complications
- Higher risk in young, female, high-grade
- Monitor with standing lateral X-rays
- Skeletal maturity typically stabilizes slip
- May develop despite conservative measures
- Consider surgery if refractory
Surgical Complications
Intraoperative:
- Incidence
- 10-25%
- Prevention
- Neuromonitoring, cautious reduction
- Incidence
- 1-5%
- Prevention
- Careful dissection
- Incidence
- Rare
- Prevention
- Avoid anterior to sacrum
Postoperative:
- Incidence
- 5-15%
- Management
- Revision fusion, bone graft
- Incidence
- 2-5%
- Management
- Revision fixation
- Incidence
- 5-10% long-term
- Management
- May need extension of fusion
- Incidence
- 1-3%
- Management
- Antibiotics, possible washout
High-Grade Specific Complications
- L5 nerve stretch injury (most common)
- Cauda equina injury
- Vascular injury
Staged reduction, intraoperative neuromonitoring, and accepting partial reduction if significant EMG changes are all important strategies.
Guidelines, Registries & Global Practice
Global Epidemiology: Spondylolysis affects roughly 6% of the adult population in unselected radiographic cohorts (Fredrickson/Beutler, USA), with a strong male predominance and an L5-S1 predilection. Prevalence is markedly higher in specific groups: certain Inuit populations report rates exceeding 25-50%, while it is uncommon in some sub-Saharan African populations, pointing to genetic as well as mechanical contributions. Athlete cohorts carry the highest acquired risk, particularly cricket fast bowlers, gymnasts, divers, weightlifters and American-football linemen, in whom repetitive lumbar hyperextension concentrates stress at the pars.
Side-by-Side Guidance (no single high-level guideline dominates this niche):
- Position on isthmic spondylolisthesis
- Non-specific; emphasises non-operative care, exercise and avoiding routine imaging unless surgery is contemplated. Surgery only for correlating radicular symptoms refractory to conservative care
- Evidence level
- Guideline (UK)
- Position on isthmic spondylolisthesis
- Trial of conservative care first; fusion (± decompression) for symptomatic slip with instability or radiculopathy; pars repair for select young patients without disc disease
- Evidence level
- Consensus / Level I-IV evidence
- Position on isthmic spondylolisthesis
- MDT assessment, conservative-first, tertiary referral for high-grade or progressive slips; neuromonitoring for reduction
- Evidence level
- Guideline / consensus
- Position on isthmic spondylolisthesis
- Spinopelvic (PI / balance) assessment central to high-grade decision-making; reduction for unbalanced pelvis
- Evidence level
- Classification / expert consensus
- Position on isthmic spondylolisthesis
- Standardised surgical principles, instrumented circumferential fusion for high-grade, emphasis on sagittal restoration
- Evidence level
- Educational / consensus
Dedicated isthmic-spondylolisthesis registries are limited; most national spine registries (e.g. Swespine, the British Spine Registry) pool degenerative and isthmic fusions. The strongest comparative evidence remains Möller & Hedlund's RCT (surgery superior to exercise in disabling adult isthmic slips) and the SPORT trial (degenerative slip — a frequently mis-cited comparator). High-grade paediatric outcome data come from single-centre prospective series (e.g. the Helenius/Turku group) rather than large registries.
There is genuine international variation in (1) whether to reduce high-grade slips (reduction favoured in North American and SDSG-influenced centres for unbalanced pelves; in situ fusion still widely used elsewhere), (2) use of interbody support versus posterolateral fusion alone for low-grade slips, and (3) the role of direct pars repair, which is offered selectively in younger patients.
MCQ Practice Points
Q: What is the pathological lesion in isthmic spondylolisthesis? A: Defect in the pars interarticularis (spondylolysis). This stress fracture typically occurs at L5 due to the oblique orientation of the pars at this level which concentrates shear forces during extension and rotation.
Q: What is the characteristic radiographic finding on oblique lumbar X-ray? A: "Collar on the Scotty dog" sign - the lucency through the pars appears as a collar on the dog-shaped vertebra on oblique views. The dog's nose is the transverse process, eye is the pedicle, ear is the superior facet, front leg is the inferior facet.
Q: What is the most common level for isthmic spondylolisthesis and why? A: L5-S1 (85-95% of cases). The L5 pars is thinner and more obliquely oriented, concentrating stress at this level. Additionally, L5 bears the maximum shear force at the lumbosacral junction due to sacral inclination.
Q: Which sports have the highest risk for developing spondylolysis? A: Gymnastics, cricket fast bowling, diving, and American football linemen. These activities involve repetitive hyperextension and rotation which concentrate stress at the pars interarticularis. Up to 40% of adolescent gymnasts have pars defects.
At a Glance
Isthmic spondylolisthesis is defined by a pars interarticularis defect (spondylolysis), distinguishing it from degenerative type which has an intact pars. It occurs at L5-S1 in 90% of cases (versus L4-5 for degenerative) with a 6% population prevalence but 80% remain asymptomatic. The classic "Scottie dog collar" sign on oblique X-ray indicates the pars defect, though CT is the gold standard for visualization. Meyerding grading quantifies slip severity (I: less than 25%, II: 25-50%, III: 50-75%, IV: 75-100%, V: spondyloptosis). Wiltse Type IIA (lytic/stress fracture) is most common. Young athletes with extension-related back pain should raise suspicion for pars stress reaction.
PARSPARS - Pars Defect Features
Hook:PARS defect defines isthmic spondylolisthesis
SLIPSLIP - Meyerding Grading
Hook:SLIP grades progress from Slight to Profound
WILTWILT - Wiltse Classification
Hook:WILT classification covers all spondylolisthesis types
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 15-year-old male gymnast presents with 6 months of low back pain worse with extension. Lateral X-ray shows Grade I L5-S1 slip. Oblique view shows bilateral pars defects (collar on Scottie dog).”
“An 18-year-old female presents with severe back pain and bilateral L5 radiculopathy. Standing lateral X-ray shows Grade III L5-S1 slip with high slip angle. She has tight hamstrings and a waddling gait.”
“A 16-year-old cricket fast bowler presents with 3 weeks of acute low back pain. No radiculopathy. X-rays are normal. MRI shows T2 hyperintensity in the left L5 pars. SPECT-CT shows increased uptake at L5.”
KEY DIFFERENTIATORS
- PARS DEFECT present = isthmic type
- L5-S1 level (90%) vs L4-5 for degenerative
- Young patients (adolescence) vs old (degenerative)
- Scottie dog collar sign on oblique X-ray
CLASSIFICATIONS
- Wiltse: Type II = isthmic (IIA lytic, IIB elongated, IIC acute)
- Meyerding: I (less than 25%) to V (spondyloptosis)
- Low-grade: I-II; High-grade: III-V
- CT is gold standard for pars visualization
CLINICAL FEATURES
- Extension-related back pain
- Hamstring tightness (classic finding)
- Step-off palpable in high-grade
- L5 radiculopathy if nerve stretch
MANAGEMENT PRINCIPLES
- 80% remain asymptomatic - observation
- Conservative first: PT, activity modification
- Pars repair: Young, no disc disease, single level
- Fusion: Failed conservative, high-grade, neurological
SURGICAL PEARLS
- In situ fusion is safer for high-grade
- Reduction improves alignment but 10-25% L5 neuropathy risk
- Always use neuromonitoring for reduction
- Pars repair: ~80% satisfactory in young patients with healthy disc and no slip
Evidence Base
Natural History (Original Cohort)
- Prospective radiographic study of 500 unselected first-grade children followed into adulthood
- Spondylolysis incidence 4.4% at age 6, rising to 6% in adulthood
- Maximum slip observed was 28%; progression of olisthesis was unusual
- Strong association with spina bifida occulta; slip never became symptomatic in this cohort
45-Year Natural History
- 45-year follow-up of the same population-based cohort (30 subjects with pars lesions)
- Subjects with UNILATERAL defects never experienced any slippage
- Slip progression slowed with each decade and no subject ever reached a 40% slip
- No association between slip progression and low back pain; SF-36 scores matched the general population
Wiltse-Newman-Macnab Classification
- Defined the five-type aetiological classification still in use: dysplastic, isthmic, degenerative, traumatic, pathological
- Isthmic (Type II) subdivided into IIA lytic/fatigue fracture, IIB elongated pars, IIC acute fracture
- Based on combined aetiological and anatomical factors
Surgery vs Exercise (Adult Isthmic)
- 111 adults (18-55 yr) with isthmic slip and ≥1 year of disabling symptoms randomised to posterolateral fusion (± instrumentation) or an exercise programme
- Function (Disability Rating Index) and pain were significantly better after surgery at both 1 and 2 years (P less than 0.01)
- The exercise group's disability did not change; pain decreased only slightly
- 93% two-year follow-up
Pelvic Incidence & Spinopelvic Balance
- 214 subjects with developmental L5-S1 spondylolisthesis vs 160 normal controls
- Pelvic incidence, sacral slope, pelvic tilt and lumbar lordosis were all significantly greater in spondylolisthesis (P less than 0.01)
- Differences widened linearly as slip severity increased
- High pelvic incidence appears to predispose to development and progression
SDSG Spinopelvic Classification
- Spinal Deformity Study Group classification of L5-S1 slips by (1) grade, (2) pelvic incidence, (3) spinopelvic alignment - six types
- Substantial intra- and inter-observer reliability; HRQOL differed significantly across types
- Distinguishes 'balanced' from 'unbalanced' high-grade pelvis to guide whether reduction is needed
Predictors of Pars Healing (Conservative)
- 23 children/adolescents (41 pars defects) treated with bracing and activity restriction, healing assessed by CT
- Early (hairline) defects healed in 87% (13/15); progressive defects only 32%; terminal (pseudarthrosis) defects 0%
- High signal change in the adjacent pedicle on T2 MRI: 77% healed; no T2-negative defect healed
Direct Pars Repair (Buck Technique)
- 9 young patients (mean age 24) with symptomatic spondylolysis and a normal disc, failing conservative care
- Radiological union achieved in all patients at mean 45-month follow-up
- Satisfactory functional outcome (MacNab) in 78% (7/9); both patients with associated Grade 1 slip did poorly (fair/poor)
Instrumented Reduction in Paediatric Slips
- 26 adolescents (11 low-grade, 15 high-grade) treated by instrumented reduction and circumferential fusion
- Mean slip reduced from 67% to 21% (high-grade) and 25% to 6% (low-grade); non-union in 12%, reoperation 27%
- No persistent neurological deficit; SRS-24 pain and activity improved but stayed below matched healthy controls
SPORT - Degenerative Spondylolisthesis (Comparator)
- 607 patients with DEGENERATIVE spondylolisthesis and stenosis (randomised + observational cohorts)
- As-treated analysis showed a substantial, durable surgical advantage in pain and function at 2 years
- High crossover in the randomised arm (~40% each direction); applies to degenerative, NOT isthmic, disease