FDP Avulsion Injury
- Caused by forced extension of a flexed DIPJ (e.g., grabbing a jersey).
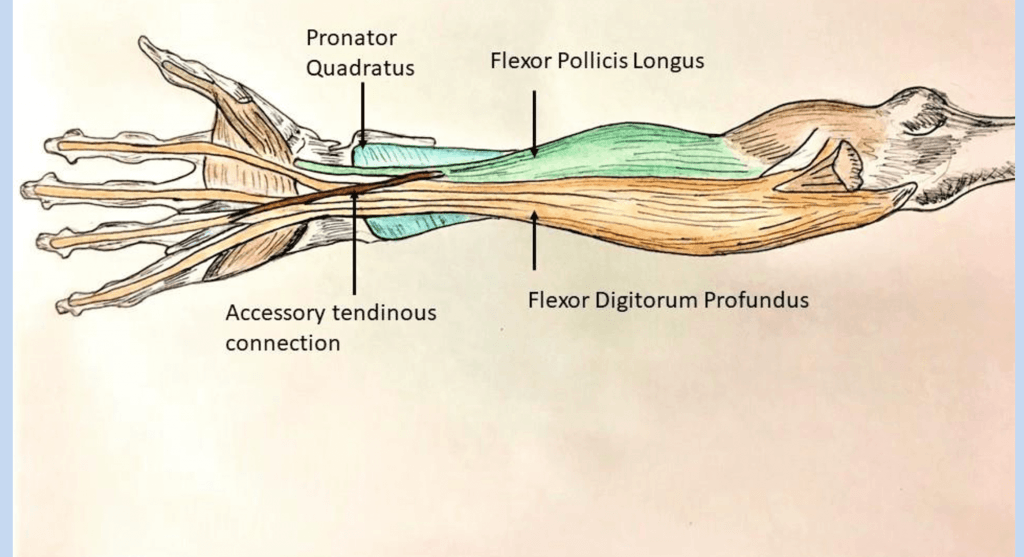
- Ring finger is most commonly affected due to tethering by lumbricals/connections.
- Type I injuries loose blood supply (vincula) and must be repaired within 7-10 days.
- Type II/III retain some blood supply via vincula and can be repaired later (up to 3-6 weeks).
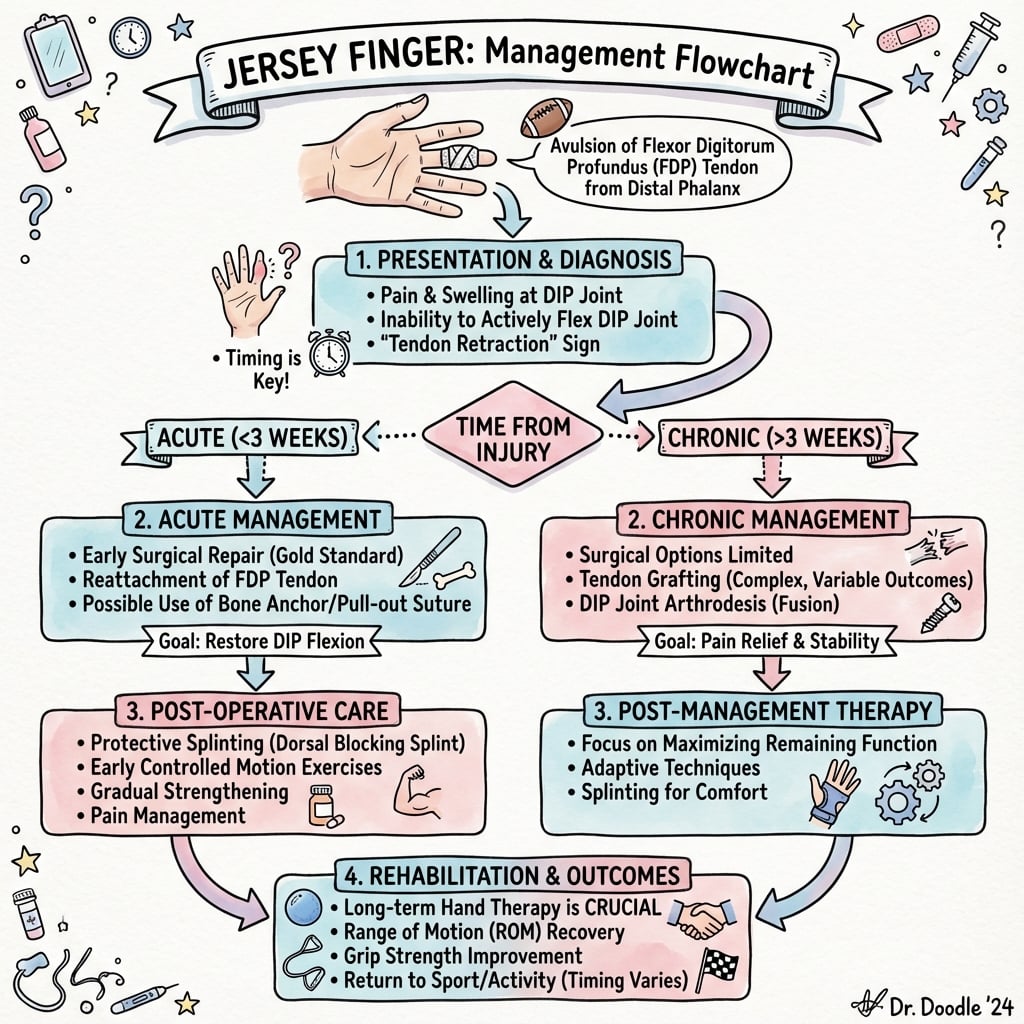
- Clinical sign: Loss of active DIP flexion. Finger lies inextension in resting cascade.
- Repair involves re-attaching tendon to bone (Suture anchor or Pull-out button).
- “Beware the 'sprained finger' diagnosis. Always test active DIP flexion isolation.
- “The FDP avulsion often includes a bony fleck visible on X-ray (Type III).
- “Chronic injuries (greater than 3 months) usually require fusion or 2-stage reconstruction.
"Just a Sprain" The finger is often swollen and painful. The patient can still flex the PIPJ (FDS intact). If you don't isolate the DIPJ, you will miss the FDP rupture. Missing a Type I injury leads to a permanently functionless FDP due to retraction and necrosis.
Isolate DIP Flexion Hold the PIPJ and MCPJ in extension. Ask the patient to flex the fingertip. If they can't then think Jersey Finger. Also check resting cascade: The finger will lie straighter than the others.
- Tendon
- FDP Avulsion
- Deformity
- Loss of DIP Flexion
- Urgency
- High (Type I)
- Tendon
- Extensor Avulsion
- Deformity
- Loss of DIP Extension
- Urgency
- Medium (Splint)
- Tendon
- Stenosing Tenosynovitis
- Deformity
- Locking in Flexion
- Urgency
- Low (Elective)
- Tendon
- Ligament Avulsion
- Deformity
- PIPJ Hyperextension
- Urgency
- Medium (Splint)
IRISPhases of Healing
Hook:The tendon heals like an IRIS opening.
RINGAnatomy of Injury
Hook:The RING finger GRABS.
Overview
Jersey Finger is an avulsion of the Flexor Digitorum Profundus (FDP) tendon from its insertion at the base of the distal phalanx. It typically occurs in contact sports when a player grabs an opponent's jersey, forcing the flexed finger into extension.
The injury is significant because the FDP is the only flexor of the DIP joint. Retraction of the tendon can compromise its vascular supply, dictating the urgency of repair.
Pathophysiology and Mechanisms
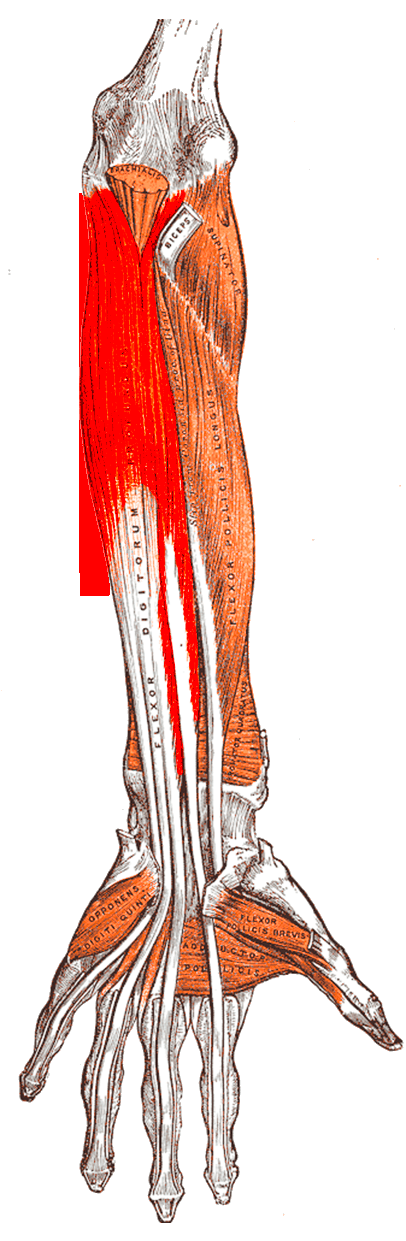
Flexor Digitorum Profundus (FDP)
- Origin: Forearm (Ulna).
- Insertion: Base of Distal Phalanx (Volar).
- Action: Flexes DIPJ, PIPJ, MCPJ, Wrist.
- Blood Supply:
- Vincula Longa: From dorsal mesentery at PIPJ level.
- Vincula Brevia: From volar plate at DIPJ level.
- Diffusion: From synovial fluid within the sheath.
The watershed zone is less relevant here than in Zone II.
Repair must respect the digital flexor sheath pulley system, which holds the tendons against the phalanges and converts excursion into joint flexion:
- Five annular pulleys (A1-A5) and three cruciate pulleys (C1-C3). The annular pulleys sit: A1, A3, A5 over the MCP, PIP and DIP joints (on the volar plates), and A2, A4 over the shafts of the proximal and middle phalanges.
- A2 and A4 are the biomechanically critical pulleys — losing them lets the tendon lift away from the bone (bowstringing), which wastes excursion, reduces the flexion arc and produces a flexion contracture. This is why the avulsed stump must be passed through the intact pulleys during retrieval, never by dividing them.
- The A4 pulley is also the structure on which a Leddy-Packer Type III bony fragment catches, holding the tendon out to length and giving the best prognosis.
Classification Systems
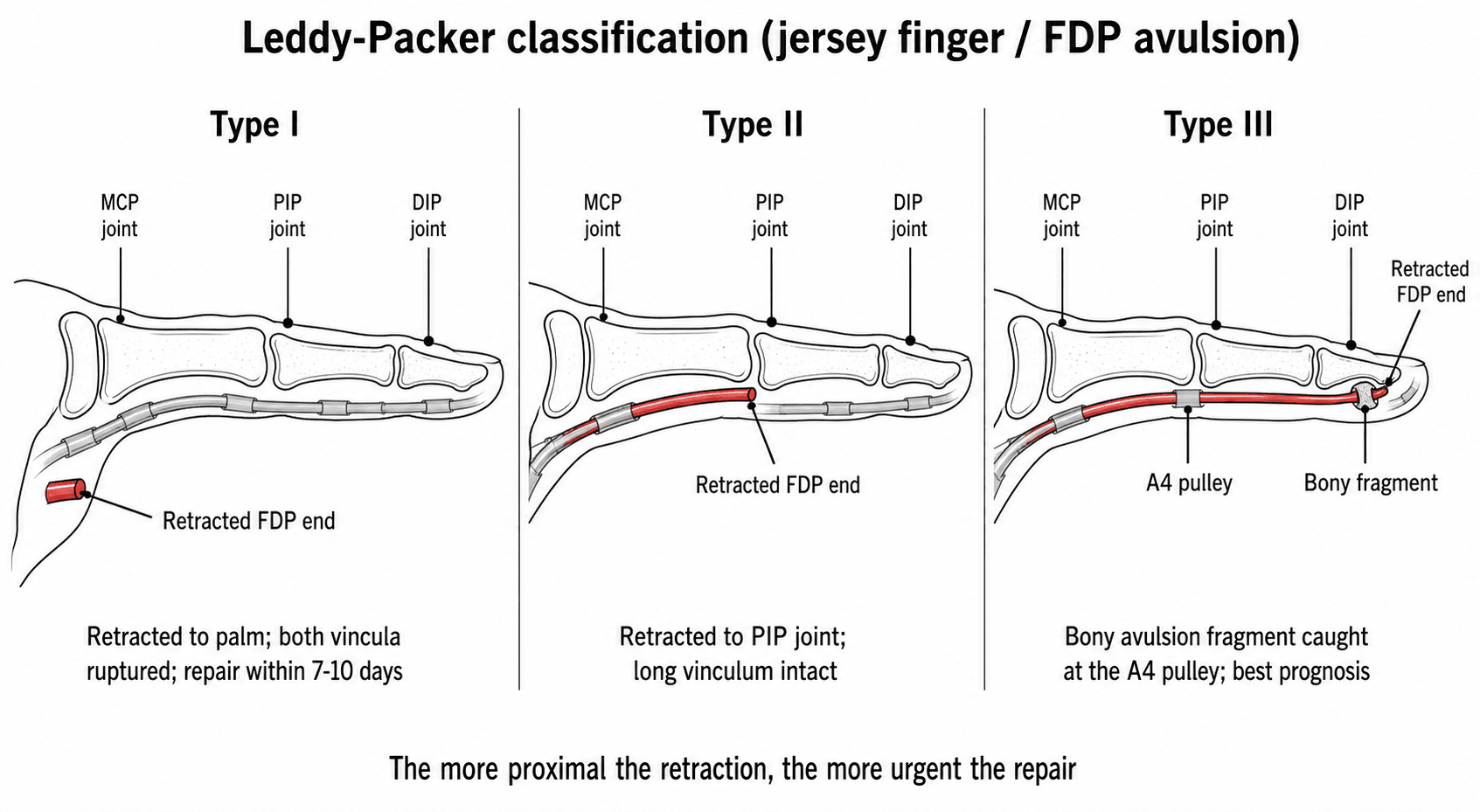
Leddy-Packer Classification
This classification guides urgency of repair.
- Type I: Tendon retracted to Palm. Vincula ruptured. URGENT (less than 1 week).
- Type II: Tendon retracted to PIPJ (Zone II). Held by Vincula Longa. FDS allows some blood supply. Semi-Urgent.
- Type III: Tendon at DIPJ (Zone I). Large bony fragment prevents retraction past A4 pulley. Elective.
- Type IV: (Smith) Avulsion of tendon OFF the fracture fragment. Or double level injury. Rare. Urgent.
- Type V: (Al-Qattan) Extra-articular bony avulsion with comminution.
Usually diagnosed on X-ray.
PALMLeddy-Packer Classification
Hook:Where did the tendon go?
Clinical Presentation
History
- Mechanism: "Grabbed a jersey", "Finger got stuck".
- Sensation: "Pop" or "Snap" felt in the finger or palm.
- Pain: Palm pain (Type I) or Finger pain (Type II/III).
- Sport/Activity: Rugby, American football, AFL, grappling sports, or rock climbing.
Ask about the specific moment of injury (tackle, grip release).
Investigations
Radiology
- Views: AP, Lateral, Oblique.
- Findings:
- Type I/II: Usually negative (pure tendon), unless small fleck visible in tendon sheath.
- Type III: Large bony fragment at DIPJ base.
X-ray is critical to identify the bony fragment location, which reveals the level of retraction.
Treatment
Acute Repair (less than 3 weeks)
- Type I: Repair within 7-10 days. Reattach to bone.
- Type II/III: Repair within 2-3 weeks. Bony fixation (Screw/Wire) for Type III.
- Technique:
- Pull-out Button: Suture passed through bone and tied over a button on the nail plate.
- Suture Anchor: Mitek anchor into P3 base.
- Retraction: Must retrieve the tendon. Carefully pass through pulleys using a catheter or pediatric feeding tube. DO NOT damage the pulleys.
Preserve the A4 pulley at all costs.
Surgical Considerations
Button vs Anchor
- Pull-out Button:
- Pros: Cheap, strong.
- Cons: External hardware, risk of nail bed injury, infection, catching on clothes.
- Suture Anchor:
- Pros: Internal, easy to use, no button complications.
- Cons: Cost, risk of implant prominence/pullout.
Current trend favors Suture Anchors (minilok/micro).
GRIPSurgical Goals
Hook:Surgery restores GRIP.
Complications
- Infection: Especially with button sutures.
- Nail Deformity: If button compresses germinal matrix.
- Flexion Contracture: PIPJ or DIPJ stiffness is very common.
- Rupture: Re-rupture of repair (5-10%).
- Quadriga: If the FDP is shortened too much, it tethers the other fingers (via the common muscle belly), preventing full flexion of the uninjured fingers.
- Bowstringing: If pulleys are sacrificed, the tendon moves away from the bone, increasing the moment arm but causing a flexion contracture and loss of digital tuck.
- Rupture: Highest risk between weeks 3-6 when the patient feels better but the tendon is soft.
- CRPS: Complex Regional Pain Syndrome is a risk with any digit surgery.
- Stiffness: DIPJ stiffness is almost guaranteed. Patients must be warned.
- Pin Site Infection: If K-wires or button used.
- Scar Sensitivity: Volar scars can be painful for gripping.
Distinct from the quadriga effect (and a classic exam pairing), the lumbrical-plus finger is the opposite tethering problem and can follow FDP avulsion, an over-long tendon graft, or a distal FDP laceration:
- Mechanism: the lumbrical originates on the FDP tendon and inserts into the radial lateral band of the extensor mechanism. If the FDP is divided/avulsed distal to the lumbrical origin or is left slack, contraction pulls the lax FDP (and the lumbrical with it) proximally.
- Result — paradoxical extension: attempting to flex the finger tightens the lumbrical and extends the IP joints instead of flexing them.
- Contrast with quadriga: quadriga = an FDP repaired/advanced too tight, causing incomplete flexion of the other fingers (shared muscle belly); lumbrical-plus = an FDP left too loose, causing paradoxical extension of the same finger. Tensioning the repair correctly (and limiting advancement) avoids both.
Rehabilitation
- Splint: Dorsal Blocking Splint (Wrist flexed 30°, MCP flexed 60-70°).
- Protocol: Modified Duran or Belfast (Passive flexion, Active extension within block).
- Therapy: 2-3 times per week with hand therapist.
- Precautions: No active flexion, no resisted motion.
- Splint: Discontinue day splint, night splint continues.
- Motion: Active flexion begins. Blocking exercises for DIP isolation.
- Scar management: Desensitization and scar massage.
- Resistance: Progressive strengthening begins.
- Grip: Therapy putty and grip dynamometer.
- Function: Return to light duties and ADLs.
- Contact sport: Clearance for full contact by 4-6 months.
- Protection: Some athletes wear buddy tape or protection initially.
- Monitoring: Watch for rupture signs during high-load activities.
Prognosis
Outcomes by Leddy-Packer Type
- Prognosis
- Guarded
- Key Factor
- Ischemic if delayed
- ROM Recovery
- 60-80%
- Prognosis
- Good
- Key Factor
- Vincula intact
- ROM Recovery
- 80-90%
- Prognosis
- Excellent
- Key Factor
- Bone-to-bone
- ROM Recovery
- 90-100%
- Prognosis
- Variable
- Key Factor
- Fracture healing
- ROM Recovery
- 70-85%
Expected Range of Motion
Following successful repair:
- DIP flexion: Typically 50-70 degrees (normal 80-90)
- Extension lag: 10-20 degree extension lag is common and acceptable
- Grip strength: Usually recovers to 85-95% of contralateral side
- Sport return: Most athletes return to full contact by 4-6 months
Factors Predicting Outcome
Positive prognostic factors:
- Early presentation (less than 7 days for Type I)
- Type III injury pattern
- Younger patient age
- Compliant rehabilitation
Negative prognostic factors:
- Delayed presentation
- Type I with retraction to palm
- Smoker
- Manual occupation (higher demands)
- Poor therapy compliance
Salvage Options
For failed primary repair or chronic missed injuries:
- DIPJ Fusion: Most reliable salvage, excellent for grip strength
- Two-stage reconstruction: High failure rate (30-40%) but can restore flexion
- Accept dysfunction: Some patients adapt well without intervention
Even with suboptimal outcomes, most patients achieve functional pinch and grip for activities of daily living.
Guidelines, Registries & Global Practice
Global Epidemiology
Jersey finger is the classic closed flexor avulsion and is strongly associated with grappling and jersey-grabbing sports worldwide:
- Rugby union and league (UK, Australia, New Zealand, South Africa, France) - the tackle and shirt-grab mechanism
- American football (the eponymous "jersey" injury) and Australian Rules football (guernsey marking contests)
- Grappling sports - judo, Brazilian jiu-jitsu and wrestling, where forced grip release loads the FDP
- Rock climbing - a recognised cause of closed FDP avulsion from crimp grips, more often involving the middle finger
The ring finger accounts for the large majority of cases, a finding established in the original 36-patient Leddy-Packer series and repeatedly confirmed since. The injury predominates in young, male, athletic populations.
Side-by-Side Guidance (No Single Country Frame)
- Position on Closed Zone I FDP Avulsion
- Operative repair is standard; urgency follows level of retraction; preserve A4/A2 pulleys; early protected motion
- Position on Closed Zone I FDP Avulsion
- Repair Type I within ~7-10 days before retraction/ischaemia; Type II/III may tolerate later repair; chronic/missed - DIPJ fusion, staged graft, or accept deficit
- Position on Closed Zone I FDP Avulsion
- Urgent hand-surgery referral for suspected closed FDP avulsion; protocol-driven hand-therapy rehabilitation
- Position on Closed Zone I FDP Avulsion
- Suture anchor or pullout button both acceptable; anchors avoid button morbidity and allow earlier motion
There is no high-level RCT dictating one fixation over another; recommendations are consensus- and cohort-based. The genuine point of agreement across societies is timing by Leddy-Packer type and pulley preservation, not the specific implant.
Registry & Outcome Evidence
Unlike arthroplasty, jersey finger has no dedicated national implant registry (suture anchors and buttons are not tracked the way joint prostheses are). The evidence base is therefore built from case series, small comparative cohorts, and biomechanical studies. Reported outcomes:
- Re-rupture rates of roughly 5-10%, highest in weeks 3-6 of rehabilitation
- Equivalent clinical ROM and grip between anchor and button techniques, with faster return to work for anchors (McCallister 2006)
- Type III bony avulsions carry the best prognosis (bone-to-bone healing); palm-retracted Type I the worst if delayed
High- vs Limited-Resource Practice Variation
- Well-resourced settings: MRI/ultrasound to localise a retracted stump when unclear; suture anchors; certified hand therapists delivering Duran/Belfast/early-active protocols; rapid access to urgent operating lists for Type I.
- Limited-resource settings: Reliance on clinical examination and plain radiographs (entirely adequate for diagnosis); pullout-button-over-button or transosseous suture techniques where anchors are unaffordable; greater reliance on DIPJ arthrodesis as a definitive, low-cost salvage where staged grafting and intensive therapy are not feasible.
- Common to all settings: The decisive variable is time to diagnosis. Delayed presentation - from initial "sprain" misdiagnosis, distance to specialist care, or athletes playing on - converts a repairable Type I into a salvage problem regardless of resources.
Controversies & Areas of Uncertainty
There is no randomised controlled trial guiding fixation choice. Most recommendations rest on small cohorts, case series, and cadaveric biomechanics. State this openly in the viva - examiners reward candidates who know the limits of the evidence.
- Anchor vs button vs transosseous suture: Clinical outcomes are equivalent (McCallister 2006), and biomechanical superiority of anchors (Putnam 2019) has not translated into a proven clinical advantage beyond faster return to work and avoidance of button morbidity. Implant choice is largely surgeon preference and resource availability.
- The true repair window for Type I: The classic "7-10 days" figure comes from the original series, not from controlled data. Some palm-retracted tendons remain reparable slightly longer if a vinculum is unexpectedly intact; conversely, an ischaemic tendon may be unsalvageable earlier. The number is a guide, not a hard rule.
- Single vs double anchor: A second anchor improves rotational control and pull-out strength biomechanically, but adds bone insult in a small distal phalanx; routine use is not established.
- Chronic reconstruction vs fusion: Staged (Hunter rod) grafting can restore active DIP flexion but carries a high complication and failure rate; many surgeons favour DIPJ arthrodesis or simply accepting the deficit, especially in manual workers. There is no consensus on the threshold for offering reconstruction.
- Quadriga risk in advancement: Advancing a retracted tendon to bridge a gap shortens the FDP and risks quadriga (incomplete flexion of adjacent fingers via the common muscle belly). The acceptable limit of advancement (often cited as ~1 cm) is a rule of thumb rather than an evidence-based threshold.
MCQ Practice Points
Q: Why is the Ring finger most commonly affected (75%)? A: The FDP is tethered by the common muscle belly and lumbricals, limiting independent extension during grip.
Q: Which Vincula are ruptured in a Type I injury? A: Both Vincula Longa and Brevia.
Q: What is the Quadriga effect? A: Incomplete flexion of adjacent fingers due to overtightening of the repaired FDP (shared muscle belly).
Q: What is the maximal delay for primary repair of a Type I injury? A: 7-10 days (before necrosis/contracture).
Q: What is the clinical sign of a jersey finger? A: Loss of isolated DIPJ flexion. The finger lies in extension in the resting cascade.
Q: Which Leddy-Packer type has the best prognosis? A: Type III - bony fragment prevents retraction, vincula intact, bone-to-bone healing.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A rugby player presents 4 weeks after 'spraining' his ring finger. He has no active DIP flexion. X-ray is normal. What is the diagnosis and management?”
“X-ray shows a large bony fragment at the volar aspect of the DIPJ. 10 days post injury.”
“A patient complains of a tender lump in the palm 3 months after a finger injury. No DIP flexion.”
“A 22-year-old rugby player presents 2 days after a tackle. He cannot flex the tip of his ring finger in isolation. X-rays are normal. How do you proceed and what do you tell him?”
Classification (Leddy-Packer)
- Type I: Palm (Urgent)
- Type II: PIP (Semi-Urgent)
- Type III: DIP (Bone)
- Type IV: Fx + Avulsion
Management
- Acute: Repair (Anchor/Button)
- Chronic: Fusion / Graft
- Rehab: Dorsal Block 6w
- Preserve A2/A4 pulleys
Key Concepts
- Ring Finger (75%)
- Vincula Blood Supply
- Quadriga Effect
- Isolate DIP Flexion
Evidence Base
Leddy & Packer: The Original Classification
- Retrospective review of 36 profundus avulsions in athletes over 5 years; the ring finger was the most commonly involved digit
- Classified into 3 types by presence of a bony fragment, level of tendon retraction, and status of the blood supply (vincula)
- Tendons retracting into the palm should be repaired within ~7 days; tendons held at the PIPJ could sometimes be repaired months later
- Late, relatively asymptomatic patients were left alone; unstable DIPJs were treated by fusion or tenodesis
Type IV Injury (Smith)
- Case report describing profundus avulsion with a simultaneous intra-articular fracture of the distal phalanx
- The tendon was avulsed off (separated from) the bony fragment - the basis of the 'Type IV' pattern
- Requires treating two problems: reduction/fixation of the fracture AND reattachment of the tendon
- Recognition matters because treating it as a simple Type III misses the displaced tendon