Tibiofemoral Mechanics | Patellofemoral Tracking | Ligament Function
- Screw-home mechanism: Automatic tibial external rotation 10° during terminal extension locks knee
- Femoral rollback 20-25mm at 90° flexion prevents posterior impingement, maintained by PCL and posterolateral corner
- ACL resists 85% of anterior tibial translation, secondary restraints resist remaining 15%
- Patellofemoral reaction force = 3-4x body weight during stair climbing, 7-8x during squatting
- Medial femoral condyle contacts 60% of tibial plateau, lateral 40% (medial bias in load distribution)
- “Q-angle averages 14° males, 17° females (increased angle raises patellofemoral stress)
- “Instant center of rotation shifts posteriorly with flexion (crucial for TKA design)
- “MCL is primary valgus restraint at 30° flexion (ACL at full extension)
- “Coupled motion: Tibial internal rotation with knee flexion, external rotation with extension
Terminal extension locks knee via tibial ER. Occurs due to asymmetric femoral condyles (lateral shorter). Popliteus unlocks knee to initiate flexion.
20-25mm posterior translation at 90° flexion. Maintains extensor mechanism leverage. PCL and posterolateral corner are critical restraints.
Primary restraint to anterior tibial translation (85%). Secondary function resists internal rotation and valgus. Failure mechanism: pivot-shift injury.
Increases with knee flexion angle. 0.5x BW at 30°, 3-4x BW at 90° (stairs), 7-8x BW at 135° (deep squat). Explains anterior knee pain in flexion.
Overview and Introduction
Knee biomechanics encompasses the study of mechanical forces, motion patterns, and structural relationships within the knee joint complex. Understanding these principles is fundamental to orthopaedic practice, informing diagnosis, surgical technique, rehabilitation, and implant design.
The knee is the largest joint in the body, bearing forces up to 6x body weight during activities. It must balance mobility (0-140° flexion) with stability for weight-bearing. This is achieved through the complex interplay of bone geometry, ligaments, menisci, and surrounding musculature.
Concepts and Principles
Key Biomechanical Principles:
- Four-Bar Linkage Model: The ACL and PCL form a crossed linkage system that constrains motion while allowing rollback
- Screw-Home Mechanism: Terminal tibial external rotation locks the knee in extension
- Coupled Motion: Flexion couples with internal rotation; extension couples with external rotation
- Instant Center of Rotation: Shifts posteriorly with flexion, important for implant design
Tibiofemoral Biomechanics
Joint Geometry and Congruency
The tibiofemoral joint is incongruent - the convex femoral condyles articulate with relatively flat tibial plateaus. This geometry allows large range of motion but requires menisci and ligaments for stability.
- Medial condyle: Longer (60% load), larger radius, extends further distally
- Lateral condyle: Shorter (40% load), smaller radius, flattens posteriorly
- Asymmetry: Drives screw-home mechanism in terminal extension
- Articular surface: Spherical anteriorly, flattens posteriorly
- Medial plateau: Concave, larger surface area, more conforming
- Lateral plateau: Convex or flat, smaller, less conforming
- Posterior slope: 5-10° posteroinferior (sagittal plane)
- Role: Minimal intrinsic stability without soft tissues
Low native congruency makes knee dependent on soft tissues. Meniscectomy or ligament injury significantly increases contact stress. ACL-deficient knee loses anterior restraint and develops abnormal kinematics. This is why ACL reconstruction restores both stability and normal motion patterns.
Tibiofemoral Motion Patterns
Knee motion combines rolling and gliding (sliding) of femoral condyles on tibial plateaus. The ratio changes with flexion angle.
- Dominant Motion
- Rolling dominant
- Femoral Contact Point
- Moves posteriorly on tibia
- Clinical Significance
- Gait cycle, stance phase
- Dominant Motion
- Mixed rolling and gliding
- Femoral Contact Point
- Progressive posterior shift
- Clinical Significance
- Stair climbing, chair rise
- Dominant Motion
- Gliding dominant
- Femoral Contact Point
- 20-25mm posterior rollback
- Clinical Significance
- Squatting, kneeling
Femoral rollback is the posterior translation of the femoral condyles on the tibial plateau during flexion. This is critical for:
- Maintaining extensor mechanism moment arm (prevents quadriceps insufficiency)
- Preventing posterior soft tissue impingement
- Allowing deep flexion without bony contact
The PCL and posterolateral corner resist excessive rollback. Loss of PCL leads to excessive posterior translation and abnormal kinematics.
Screw-Home Mechanism
The screw-home mechanism is the automatic external rotation of the tibia (10°) during the last 20-30° of extension. This locks the knee in full extension for energy-efficient standing.
Anatomical Basis
- Asymmetric condyles: Lateral condyle shorter than medial
- Geometry: Tibial ER aligns femoral condyles with tibial plateaus
- Result: Maximum bony congruency at full extension
- Stability: Locked position for standing without muscle effort
- Popliteus muscle contracts
- Action: Internally rotates tibia, "unlocks" knee
- Timing: Must occur before knee can flex from extension
- Clinical: Popliteus injury causes "unlocking" difficulty
Q: How do you demonstrate screw-home mechanism clinically? A: Place patient supine with knee flexed 20°. Passively extend knee while palpating tibial tuberosity. Feel tibial external rotation during terminal extension. Absence suggests ACL or meniscal pathology affecting normal kinematics.
Ligament Function and Load Sharing
Anterior Cruciate Ligament (ACL)
The ACL is the primary restraint to anterior tibial translation, resisting 85% of anterior drawer force at 30° flexion.
- Anterior translation: Resists 85% of anterior tibial displacement
- Peak tension: 30° flexion (Lachman position)
- Secondary functions: Resists internal rotation, valgus stress
- Bundles: Anteromedial (tight in flexion), posterolateral (tight in extension)
- Pivot-shift injury: Valgus + internal rotation + anterior translation
- Non-contact: Deceleration with foot planted, knee near extension
- Result: Abnormal anterior translation, rotatory instability
- Compensation: Secondary restraints insufficient alone
Secondary restraints to anterior translation include:
- Medial and lateral menisci (posterior horns)
- MCL (medial capsule)
- Posterolateral corner
- Iliotibial band
These resist approximately 15% of anterior drawer force combined. ACL reconstruction restores primary restraint and normal kinematics.
Posterior Cruciate Ligament (PCL)
The PCL resists posterior tibial translation and maintains femoral rollback during flexion.
PCL-deficient knees develop excessive posterior translation and loss of femoral rollback, leading to:
- Patellofemoral pain (loss of extensor mechanism leverage)
- Increased medial compartment load
- Difficulty descending stairs or slopes
Collateral Ligaments
- Primary Restraint
- Valgus stress (30° flexion)
- Peak Load Angle
- 25° flexion for superficial MCL
- Associated Structures
- Medial meniscus, posterior capsule
- Primary Restraint
- Varus stress (30° flexion)
- Peak Load Angle
- 30° flexion for LCL
- Associated Structures
- Posterolateral corner, lateral meniscus
At full extension, the ACL and posterior capsule become primary restraints to valgus/varus stress. At 30° flexion, collaterals are isolated and maximally stressed.
Patellofemoral Biomechanics
Patellofemoral Joint Forces
The patella functions as a mechanical lever to increase the moment arm of the quadriceps, improving extension efficiency. However, this creates large compressive forces at the patellofemoral joint.
- Walking: 0.5x body weight
- Stair climbing: 3-4x body weight
- Squatting (90°): 7-8x body weight
- Deep squat (135°): Up to 8-10x body weight
- Flexion angle: Greater flexion = greater quadriceps force needed
- Moment arm: Patellar tendon lever arm decreases in deep flexion
- Contact area: Peak stress at 60-90° flexion
- Clinical: Explains anterior knee pain with stairs/squats
Patellar Tracking
Normal patellar tracking requires balance between medial and lateral stabilizers.
- Restraint Direction
- Resists lateral displacement
- Contribution
- 50-60% of medial restraint
- Failure Pattern
- Patellar dislocation (lateral)
- Restraint Direction
- Dynamic medial stabilizer
- Contribution
- Active stabilization in extension
- Failure Pattern
- VMO atrophy worsens tracking
- Restraint Direction
- Passive lateral tether
- Contribution
- Balanced by medial structures
- Failure Pattern
- Tightness causes lateral tilt/compression
Q-angle (quadriceps angle) measures the vector of quadriceps pull relative to patellar tendon. Normal values:
- Males: 14° average
- Females: 17° average (wider pelvis)
Increased Q-angle raises lateral patellar stress and predisposes to lateral tracking disorders.
Load Distribution and Contact Mechanics


Tibiofemoral Contact Stress
The menisci are critical for load distribution. They transmit 40-60% of knee joint load and reduce peak contact stress on articular cartilage.
Meniscectomy consequences:
- Total meniscectomy: 200-300% increase in peak contact stress
- Partial meniscectomy: 65-100% increase (depends on amount removed)
- Increased risk of osteoarthritis
Alignment effects:
- Varus alignment: Shifts load medially (medial compartment overload)
- Valgus alignment: Shifts load laterally (lateral compartment overload)
- Neutral alignment: 60% medial, 40% lateral load distribution
Meniscal Hoop Stress
The menisci transmit load not just by filling the joint space but through a specific mechanism - circumferential (hoop) stress - and understanding it explains why some meniscal tears are biomechanically catastrophic while others are tolerated.
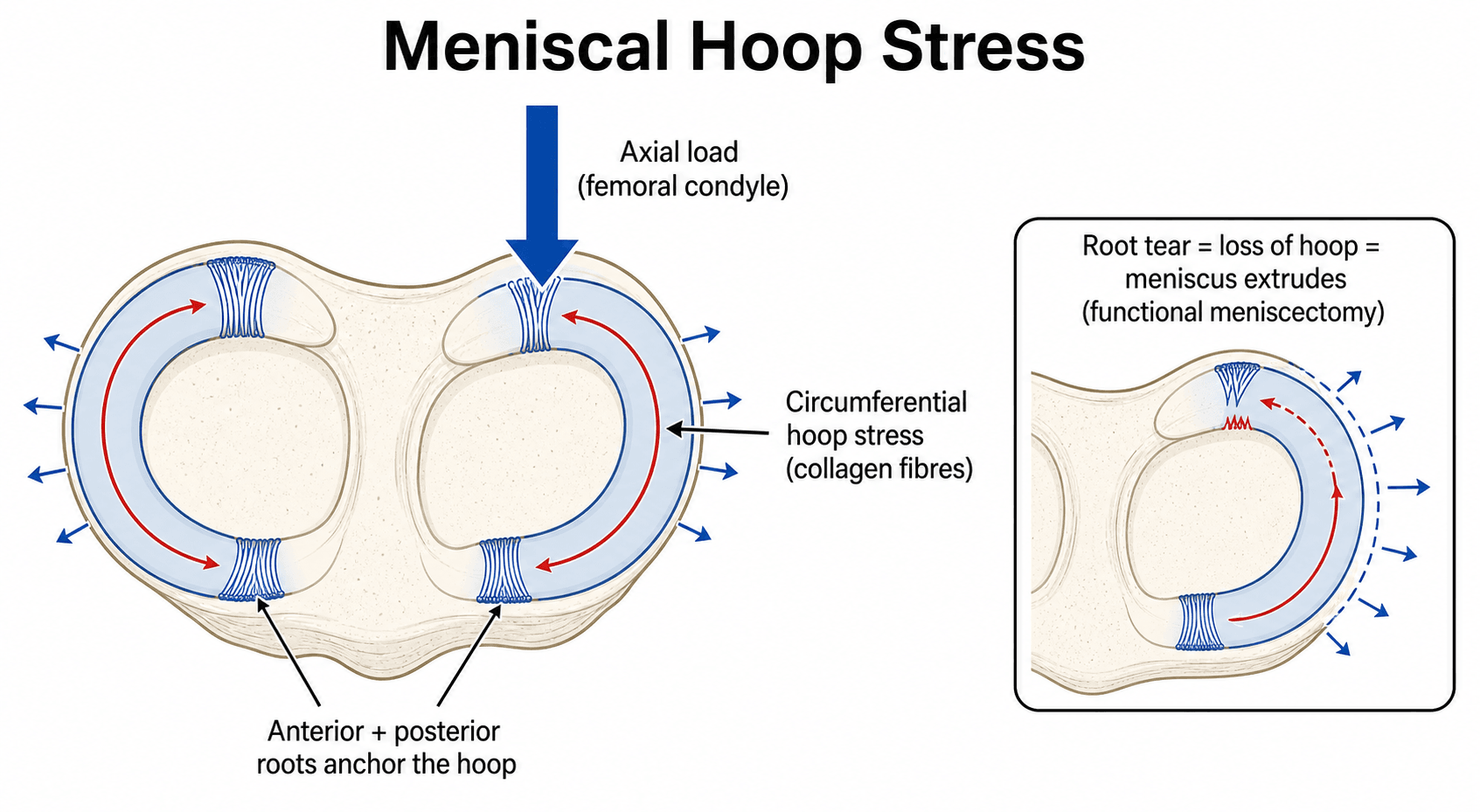
The mechanism:
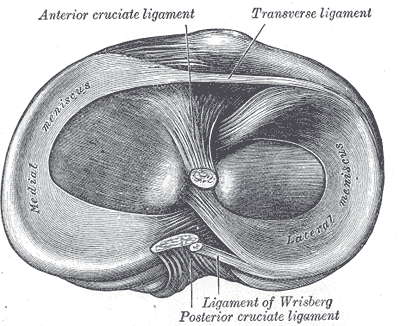
- The meniscus is built from circumferentially oriented collagen fibres (with a few radial "tie" fibres), anchored to the tibia at the anterior and posterior meniscal roots.
- Under axial compression the wedge-shaped meniscus tends to be extruded peripherally; the circumferential fibres, held by the roots, resist this by developing circumferential tensile (hoop) stress.
- This converts vertical compressive load into circumferential tension, spreading load over a larger area and protecting the articular cartilage.
Why the tear pattern matters:
- Effect on hoop stress
- Largely PRESERVES the circumferential fibres
- Biomechanical consequence
- Hoop function maintained; repairable, better prognosis
- Effect on hoop stress
- DISRUPTS the circumferential fibres
- Biomechanical consequence
- Abolishes hoop stress in that segment - functionally like a meniscectomy
- Effect on hoop stress
- Detaches the anchor, so no hoop tension can develop
- Biomechanical consequence
- Equivalent to a total meniscectomy; causes meniscal extrusion and rapid cartilage loss
Hoop stress is the key: the meniscus converts axial load into circumferential tension held by its roots. A radial tear that reaches the rim, or a root avulsion, abolishes hoop stress and is biomechanically equivalent to total meniscectomy - the meniscus extrudes and contact stress rises sharply, which is why root repair is emphasised. Longitudinal tears spare the circumferential fibres and carry a better prognosis.
Clinical Applications
Total Knee Arthroplasty Design Considerations
Understanding knee biomechanics guides TKA design:
- Rollback: Must replicate normal posterior translation
- J-curve: Matches native femoral condyle geometry
- Asymmetric condyles: Replicates medial/lateral differences
- Goal: Restore normal kinematics and ROM
- Posterior slope: 0-7° to facilitate rollback
- Conformity: More conforming = lower contact stress but less mobility
- Flat vs dished: Trade-off between stability and constraint
- Polyethylene: Must withstand 3-6x BW cyclically
Cruciate-retaining vs posterior-stabilized TKA:
- CR-TKA: Preserves PCL, maintains femoral rollback naturally
- PS-TKA: Resects PCL, uses cam-post mechanism to replicate rollback
- Both aim to restore 20-25mm posterior translation at 90° flexion
Gait and the Knee Adduction Moment (KAM)
Static load distribution (the 60:40 medial bias) is amplified dynamically during gait, and the examiner-relevant concept is the knee adduction moment (KAM) - the single most important gait-derived determinant of medial-compartment load.
The concept:
- During the stance phase the ground reaction force passes medial to the knee joint centre, creating an external knee adduction moment that loads the medial compartment (the dynamic counterpart of the static medial bias).
- The magnitude of the KAM (and the KAM impulse over stance) correlates with medial-compartment load and predicts progression of medial knee osteoarthritis; a varus thrust during gait increases it.
Offloading the medial compartment therefore works by reducing the KAM:
- How it reduces medial load
- Shifts the mechanical axis laterally, moving load off the medial compartment
- How it reduces medial load
- Applies a corrective valgus moment across the knee
- How it reduces medial load
- Moves the ground reaction force vector laterally (modest, variable effect)
- How it reduces medial load
- Reduces the moment arm or the magnitude of the ground reaction force
In stance the ground reaction force passes medial to the knee, producing an external adduction moment that loads the medial compartment - and its magnitude predicts medial OA progression. Every medial-offloading strategy (HTO, valgus brace, lateral wedge, gait retraining, weight loss) works by lowering the KAM, the dynamic link between alignment and compartment load.
Mapping Kinematics to Instability Patterns
A frequent viva failure is reciting ligament functions in isolation. Examiners reward candidates who translate the biomechanics into the clinical instability pattern, its provocative test, and the abnormal motion produced. This is effectively the biomechanical "differential diagnosis" of the unstable knee.
- Abnormal Motion
- Anterior translation + anterolateral rotatory instability
- Key Clinical Test
- Lachman (most sensitive), pivot-shift
- Distinguishing Feature
- Pivot-shift reproduces the giving-way; Lachman soft end-point
- Abnormal Motion
- Posterior translation, loss of rollback
- Key Clinical Test
- Posterior drawer, quadriceps active test, posterior sag
- Distinguishing Feature
- Sag sign at 90°; difficulty descending stairs/slopes
- Abnormal Motion
- Valgus laxity (maximal at 30°)
- Key Clinical Test
- Valgus stress at 0° and 30°
- Distinguishing Feature
- Laxity at 30° only = isolated MCL; laxity at 0° implies cruciate/capsule too
- Abnormal Motion
- Varus + external rotation instability
- Key Clinical Test
- Dial test (asymmetric ER at 30°), varus stress, external rotation recurvatum
- Distinguishing Feature
- Increased ER at 30° but not 90° suggests isolated PLC; both implies PCL involvement
- Abnormal Motion
- Lateral patellar translation/dislocation
- Key Clinical Test
- Patellar apprehension, glide test, J-sign
- Distinguishing Feature
- Apprehension near extension; positive lateral glide over 50% of patellar width
Guidelines, Registries & Global Practice
Knee biomechanics is examined across every major fellowship (FRCS Tr&Orth, FRACS, EBOT/FEBOT, ABOS, DNB/MS, MRCS, SICOT). The numbers and mechanisms are universal; the clinical translation differs mainly in implant selection and alignment philosophy, where the national arthroplasty registries provide the strongest comparative evidence.
Global Epidemiology and Examination Relevance
- The knee is the largest synovial joint and the most commonly replaced joint worldwide; symptomatic knee osteoarthritis affects a large and rising share of adults over 60, driven by ageing and obesity.
- Core examined concepts are consistent globally: ACL load sharing (approximately 85% primary restraint), femoral rollback (20-25mm at 90°), the screw-home mechanism (around 10° tibial external rotation), and patellofemoral force escalation with flexion.
- The four-bar cruciate linkage, instant centre of rotation, and coupled rotation are standard basic-science viva material in all curricula.
Alignment Philosophy: Side-by-Side
- Emphasis
- Evidence-based OA management; implant selection by surgeon and registry data
- Practical Position
- Mechanical alignment remains the reference standard; kinematic alignment is an accepted alternative under study
- Emphasis
- Cost-effectiveness and non-operative optimisation before arthroplasty
- Practical Position
- Mechanical-alignment TKA with proven implants (NJR-monitored); restricted indications for newer techniques
- Emphasis
- Articular restoration and joint-line preservation in trauma/periarticular fixation
- Practical Position
- Restore native posterior slope and coronal alignment to recreate normal kinematics after fracture
- Emphasis
- Personalised/functional alignment debate; meniscus preservation
- Practical Position
- Growing interest in kinematic and functional alignment; strong consensus favouring meniscus repair over resection
Registry Evidence (Arthroplasty Kinematics)
- NJR (UK), AJRR (US), AOANJRR (Australia), SHAR (Sweden), Norwegian and NZJR all track TKA implant survival and revision by design.
- Registries consistently show that cruciate-retaining (CR) and posterior-stabilised (PS) TKA achieve comparable long-term survivorship; the choice is driven by PCL competence, deformity and surgeon preference rather than a clear kinematic superiority.
- Registry surveillance was central to identifying poorly performing designs early, reinforcing the principle that kinematic theory must be validated by real-world revision data.
High- vs Limited-Resource Practice Variation
- High-resource settings: fluoroscopic and optical gait analysis, robotic/navigated alignment, and routine MPFL reconstruction for patellar instability are available; meniscus repair is prioritised over resection.
- Limited-resource settings: clinical kinematic assessment (Lachman, pivot-shift, screw-home palpation) and plain radiographs carry the diagnostic load; meniscectomy may still be performed where repair facilities or follow-up are unavailable, accepting the higher long-term osteoarthritis risk demonstrated by contact-mechanics studies.
- The biomechanical reasoning is identical everywhere; resource constraints alter how aggressively native kinematics can be restored.
Controversies and Areas of Uncertainty
Knee biomechanics is mature but several practice-relevant debates remain genuinely unsettled and are favourite higher-order viva probes:
- Alignment philosophy in TKA. Mechanical alignment is the validated reference standard, but kinematic and functional alignment aim to better reproduce native rollback and soft-tissue balance. Registry-level evidence of superior survivorship for kinematic alignment is not yet established, so it remains under evaluation rather than standard of care.
- CR versus PS TKA. Both replicate rollback differently (intact PCL versus cam-post), and registries show comparable survivorship. The "correct" choice is patient-specific (PCL competence, deformity) rather than universally superior.
- The medial-pivot concept. Although described as the "normal" kinematic pattern, in-vivo fluoroscopy shows a true medial pivot in only about half of normal knees during deep flexion, questioning how faithfully any single implant design should enforce it.
- Posterior tibial slope. Increased slope facilitates rollback and flexion but raises ACL/graft strain and anterior tibial translation; the optimal slope, especially in ACL-deficient and revision knees, is debated.
- The "isometric" ACL. The ACL is not truly isometric; anteromedial and posterolateral bundles tension reciprocally, fuelling the single- versus double-bundle reconstruction debate, where double-bundle has not shown consistent clinical superiority.
MCQ Practice Points
Q: What percentage of knee joint load is transmitted through the menisci in a healthy knee? A: 40-60% - The menisci are critical load distributors. Total meniscectomy increases peak contact stress by 200-300%, significantly raising osteoarthritis risk.
Q: What percentage of anterior drawer restraint does the ACL provide at 30° flexion? A: 85% - The ACL is the primary anterior restraint. Secondary restraints (menisci, MCL, capsule) resist only 15%, which is insufficient to prevent abnormal kinematics when ACL is torn.
Q: How much posterior femoral translation (rollback) occurs at 90° knee flexion? A: 20-25mm - Femoral rollback is critical for maintaining extensor mechanism leverage and preventing posterior impingement. PCL and posterolateral corner resist excessive rollback.
At a Glance
The knee experiences forces of 2-3× body weight during walking (up to 6× running) and 3-4× body weight patellofemoral force during stair climbing, making biomechanical understanding crucial for clinical practice. The screw-home mechanism automatically externally rotates the tibia 10° during terminal extension due to asymmetric femoral condyles (lateral shorter), locking the knee for standing stability—the popliteus unlocks this to initiate flexion. Femoral rollback (20-25mm at 90° flexion) prevents posterior impingement and maintains extensor mechanism leverage, controlled by the PCL and posterolateral corner. The ACL resists 85% of anterior tibial translation, with secondary restraints handling the remaining 15%; the MCL is the primary valgus restraint at 30° flexion while the ACL assumes this role at full extension. Patellofemoral reaction force increases exponentially with flexion, reaching 7-8× body weight during deep squatting, explaining anterior knee pain in flexion-loading activities.
APMRFour Major Knee Ligaments and Primary Functions
Hook:APMR keeps knees stable: Anterior/Posterior translation, Medial/Lateral (Rotational) stability!
LEAPScrew-Home Mechanism Components
Hook:LEAP into extension: Lateral condyle shorter drives External rotation for Automatic locking, Popliteus unlocks!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“Examiner asks: Describe the screw-home mechanism of the knee. Why does it occur and what is its clinical significance?”
“Examiner shows fluoroscopy of ACL-deficient knee and asks: Explain the biomechanical functions of the ACL and what happens when it is torn.”
“Examiner asks: A patient describes anterior knee pain that is worst going down stairs and rising from a chair, but minimal on level walking. Explain the biomechanics, and how patellar stability is maintained.”
Tibiofemoral Motion
- Screw-home mechanism = 10° tibial ER in terminal extension (locks knee)
- Femoral rollback = 20-25mm posterior at 90° flexion (PCL maintains)
- Rolling dominant 0-30°, gliding dominant 30-140°
- Functional ROM for ADLs = 0-110° flexion
Ligament Functions
- ACL: 85% anterior translation restraint, secondary IR/valgus
- PCL: 95% posterior translation restraint, maintains rollback
- MCL: Primary valgus restraint at 30° flexion
- LCL/PLC: Primary varus restraint, posterolateral stability
Patellofemoral Mechanics
- PF force: 0.5x BW walking, 3-4x BW stairs, 7-8x BW squatting
- Q-angle: 14° males, 17° females (higher = more lateral stress)
- MPFL provides 50-60% medial restraint to patellar dislocation
- Contact stress peaks at 60-90° flexion
Load Distribution
- Menisci transmit 40-60% of joint load
- Total meniscectomy increases peak stress 200-300%
- Medial:lateral load ratio = 60:40 in neutral alignment
- Varus shifts load medially, valgus shifts laterally
TKA Design Principles
- Must replicate 20-25mm femoral rollback at 90° flexion
- Tibial slope 0-7° facilitates rollback
- CR-TKA preserves PCL, PS-TKA uses cam-post mechanism
- Goal: restore normal kinematics and ROM 0-120°
Key Numbers
- Joint forces: 2-3x BW walking, up to 6x BW running
- Popliteus unlocks knee (IR tibia) to initiate flexion
- PCL is 2x stronger than ACL
- Secondary restraints resist only 15% anterior drawer
Evidence Base
The biomechanical principles in this topic rest on a small number of classic cadaveric and in-vivo studies that remain the most-cited primary sources in knee biomechanics. Each card below is linked to its PubMed record for independent verification.
ACL is the Primary Restraint to Anterior Drawer (85%)
- Cadaveric selective-cutting study quantifying primary vs secondary restraints
- ACL provided approximately 85% of the total restraining force to anterior drawer
- Remaining restraint shared by iliotibial tract, mid-medial and mid-lateral capsule, and collaterals
- PCL was the primary restraint (approximately 90%) to posterior drawer
PCL and Posterolateral Structures: Selective-Cutting Stability Study
- Seventeen cadaveric knees tested at 0-90° with sequential ligament sectioning
- PCL was the principal restraint to posterior tibial translation at all flexion angles
- LCL and deep posterolateral (popliteus-arcuate) complex were principal restraints to varus and external rotation
- Isolated PCL section did not increase varus or external rotation - combined injury required for major rotatory instability
Multicentre In-Vivo Kinematics: Femoral Rollback and Paradoxical Motion
- Summation of over 70 fluoroscopic studies: 811 knees, 733 subjects, 33 TKA designs
- Normal and ACL-retaining knees showed the greatest posterior femoral translation (rollback)
- PCL-retaining TKA most commonly showed paradoxical ANTERIOR femoral translation in deep flexion
- A medial-pivot pattern was seen in only about 55% of knees during deep flexion (substantial variability)
Menisci Transmit a Major Fraction of Tibiofemoral Load
- In-vitro micro-indentation transducer mapping of tibial-surface pressure in 18 cadaveric knees
- A significant fraction of joint compressive load is transmitted through the menisci
- Total (medial) meniscectomy caused a drastic alteration in tibial pressure distribution
- Findings link meniscectomy to elevated contact stress and post-meniscectomy degeneration
MPFL is the Primary Soft-Tissue Restraint to Lateral Patellar Translation (60%)
- Nine fresh-frozen cadaveric knees, sequential sectioning at 20° flexion
- MPFL provided 60% of the total restraint to lateral patellar translation
- Medial patellomeniscal ligament contributed 13%, lateral retinaculum 10%
- Superficial medial retinaculum and patellotibial ligament were not functionally important
Patellofemoral Contact Mechanics and the Odd-Facet Phenomenon
- Cadaveric dye-staining of patellofemoral contact under simulated weight-bearing through the arc of motion
- Contact band sweeps inferior-to-superior across the patella as flexion increases
- The medial 'odd facet' is a habitual non-contact area until very deep flexion (around 135°)
- Patella holds the quadriceps tendon off the femur until tendofemoral contact forms in deep flexion