Motion Segments | Load Distribution | Three-Column Theory
- Functional spinal unit = two adjacent vertebrae plus intervening disc and ligaments
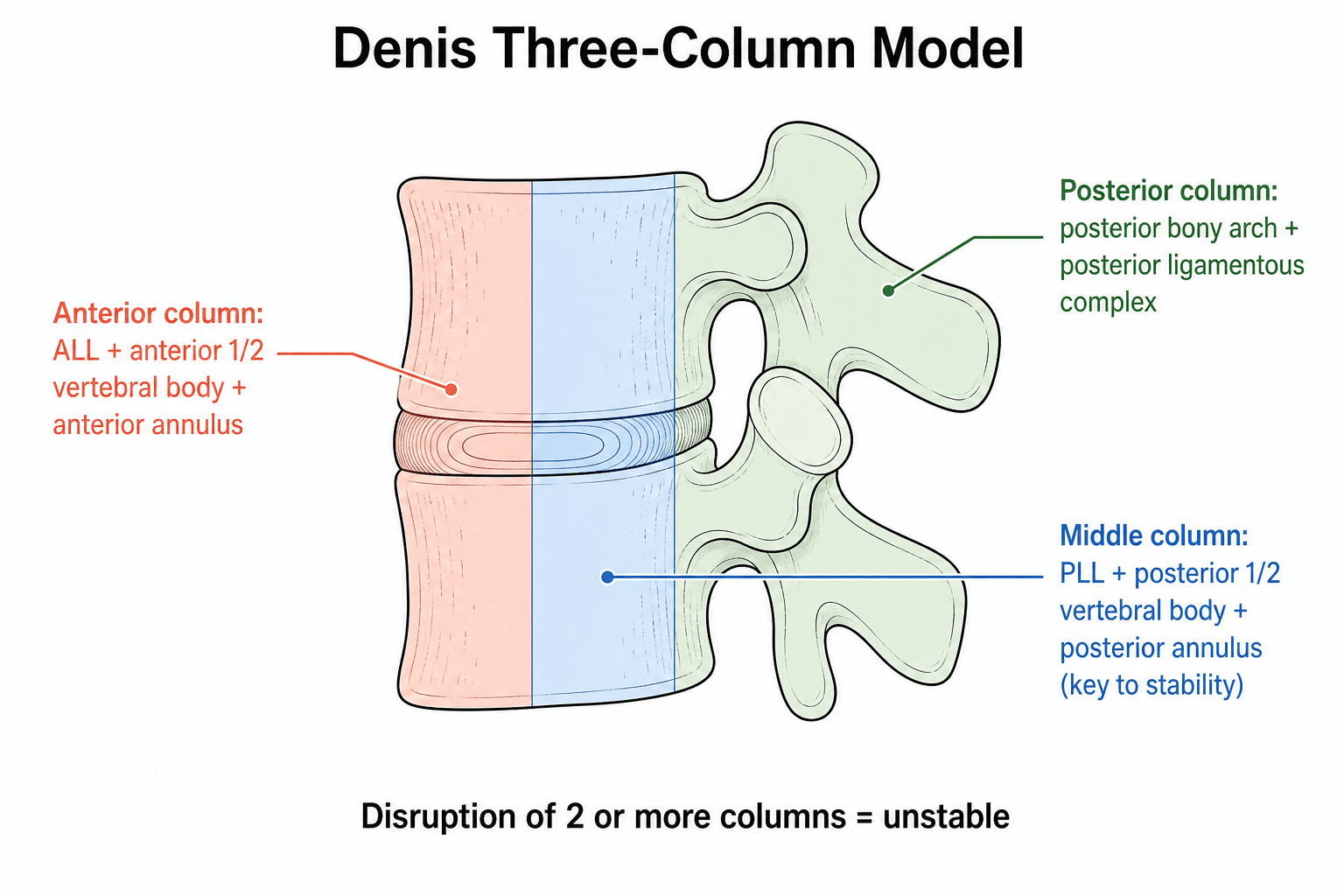
- Denis three-column theory: Anterior (ALL + anterior 50% body), Middle (posterior 50% body + PLL), Posterior (pedicles to spinous processes)
- Instantaneous axis of rotation (IAR) varies with spinal level and loading
- Nucleus pulposus behaves as incompressible fluid under axial load
- Facet joints resist shear and guide motion in sagittal or coronal plane
- “White and Panjabi criteria for clinical instability
- “Intradiscal pressure highest in sitting flexion position
- “Cervical lordosis averages 40 degrees, lumbar lordosis 60 degrees
- “Coup and contrecoup injury patterns in spinal trauma
Two adjacent vertebrae plus intervening structures. Includes disc, facet joints, ligaments. Smallest functional unit of spine motion.
Instability if 2 or more columns disrupted. Anterior = ALL + anterior 50% body. Middle = PLL + posterior 50% body. Posterior = neural arch.
IAR location determines motion pattern. Normal IAR in disc space. Abnormal IAR indicates instability or degeneration.
70% load through anterior column. Disc bears majority of axial load. Facets bear 10-30% depending on posture.


Overview and Introduction
What is Spinal Biomechanics?
Spinal biomechanics is the study of mechanical principles governing spinal motion, load distribution, and stability. Understanding these principles is essential for interpreting spinal pathology, assessing instability, and planning surgical interventions. The spine functions as a flexible column that must balance competing demands: mobility for daily activities and stability to protect neural elements.
The Functional Spinal Unit
The functional spinal unit (FSU), also called a motion segment, is the smallest physiological unit of the spine capable of exhibiting biomechanical characteristics similar to the entire spine. It consists of two adjacent vertebrae, the intervening intervertebral disc, all adjoining ligaments, and the paired facet joints.
- Anterior elements: Vertebral bodies, intervertebral disc, anterior/posterior longitudinal ligaments
- Posterior elements: Pedicles, facet joints, laminae, spinous process, ligamentum flavum, interspinous/supraspinous ligaments
- Neurovascular: Nerve roots, spinal cord (if present), blood supply
- Load bearing: Anterior column (70%), posterior column (10-30%)
- Motion control: Six degrees of freedom (3 translations, 3 rotations)
- Stability: Resists excessive displacement under physiological loads
- Protection: Neural elements housed within spinal canal
Degrees of Freedom
Each spinal motion segment has six degrees of freedom: three translations (anterior-posterior, lateral, vertical) and three rotations (flexion-extension, lateral bending, axial rotation). The range of motion varies by spinal region.
Understanding degrees of freedom is critical for analyzing instability.
Concepts in Spinal Biomechanics
Load Transmission Through the Spine
The spine transmits load through two parallel systems: the anterior column (vertebral bodies and discs) and the posterior column (facet joints and neural arch). In neutral standing, approximately 70% of axial load passes through the anterior column, while the posterior elements bear 10-30%. This distribution changes with posture, increasing posterior load in extension and anterior load in flexion.
Three-Column Stability Model
Denis proposed a conceptual framework dividing the spine into three structural columns to assess stability. This model recognizes that the middle column is the critical determinant of spinal stability.
Motion Control and the Instantaneous Axis of Rotation
During spinal motion, each vertebra rotates about a point called the instantaneous axis of rotation (IAR). In a healthy spine, the IAR is located within the disc space or adjacent vertebral body. Abnormal IAR location outside these boundaries indicates instability or degeneration. Understanding IAR is crucial for evaluating pathological motion patterns.
Denis Three-Column Theory
Denis proposed a three-column model in 1983 to classify thoracolumbar fractures and predict stability. Disruption of two or more columns indicates spinal instability.
- Anatomical Structures
- ALL, anterior 50% vertebral body, anterior annulus
- Primary Function
- Resists extension and axial load
- Failure Mode
- Compression fracture
- Anatomical Structures
- PLL, posterior 50% vertebral body, posterior annulus
- Primary Function
- Resists flexion, critical for stability
- Failure Mode
- Burst fracture with canal compromise
- Anatomical Structures
- Pedicles, facets, laminae, spinous processes, ligaments
- Primary Function
- Resists flexion and rotation, tension band
- Failure Mode
- Distraction injury (Chance fracture)
Middle column integrity determines spinal stability. Isolated anterior or posterior column injury is often stable. Middle column failure with one other column = unstable. This guides surgical decision-making for thoracolumbar fractures.
Spinal Stability: The Neutral Zone and Panjabi's Three Subsystems
Denis describes the structural anatomy of stability; Panjabi describes its functional control. Panjabi defined the neutral zone as the small region of intervertebral motion around the neutral posture within which the passive osteoligamentous spine offers minimal resistance. Beyond it lies the elastic zone, where resistance rises steeply up to the physiological limit. The neutral zone, not total range of motion, is the more sensitive marker of instability: it enlarges with injury, disc degeneration and ligamentous laxity, and it shrinks with muscle activation across the segment and with instrumented fixation or fusion.
Panjabi conceived spinal stability as three interacting subsystems.
- Components
- Vertebrae, discs, facet joints, capsules and ligaments
- Role
- Provides intrinsic restraint, mainly near the end of range; defines the neutral zone
- Components
- Muscles and tendons and the tension they generate
- Role
- Generates force to control the neutral zone and respond to changing load
- Components
- Central nervous system, proprioceptors and feedback pathways
- Role
- Senses position and load and coordinates the muscle response in real time
Clinical instability is best understood as loss of control of the neutral zone rather than simply excessive total range of motion. This is why a segment can be unstable yet retain near-normal end-range motion, and why both muscle rehabilitation and segmental fixation reduce the neutral zone and restore stability.
Load Distribution and Disc Mechanics
Axial Load Sharing
The anterior column (vertebral body and disc) bears approximately 70% of axial load in neutral standing. The posterior elements (facet joints) bear 10-30%, increasing with extension.
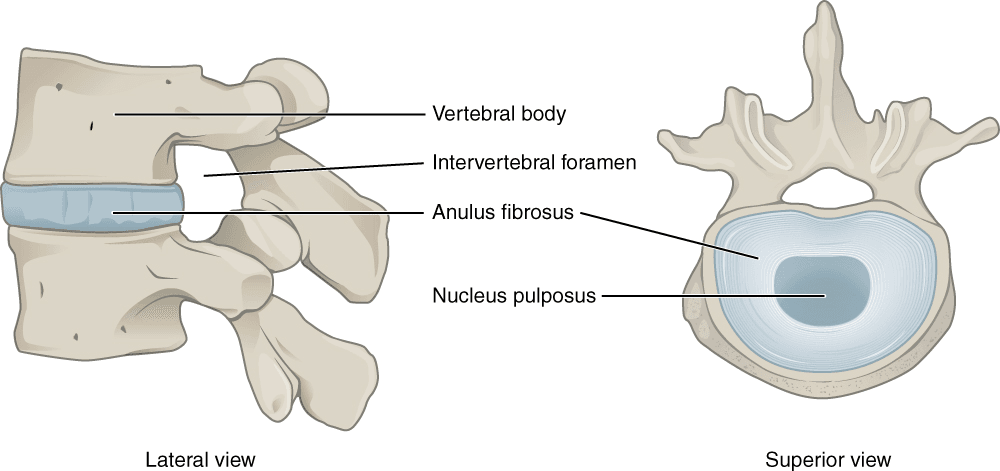
- Nucleus pulposus: 80% water (young), behaves as incompressible fluid
- Annulus fibrosus: Concentric lamellae of type I collagen
- Hydrostatic pressure: Distributes load, increases with axial compression
- Degeneration: Water loss reduces shock absorption
- Orientation: Sagittal (cervical/lumbar) allows flexion-extension
- Orientation: Coronal (thoracic) allows lateral bending
- Load bearing: Increases with extension and disc degeneration
- Shear resistance: Prevents anterior translation
Intradiscal Pressure
Nachemson demonstrated that intradiscal pressure is highest in sitting flexion (275% of standing), intermediate in standing (100%), and lowest in supine (25%). This has implications for patient positioning and rehabilitation.
Instantaneous Axis of Rotation
The instantaneous axis of rotation (IAR) is the point about which a vertebra rotates during motion. In a healthy spine, the IAR is located within the disc space or adjacent vertebral body. Abnormal IAR location indicates instability or degeneration.
Clinical Significance
- Normal IAR: Within disc space, consistent motion pattern
- Abnormal IAR: Outside disc space, indicative of instability
- Degenerative changes: IAR shifts posteriorly with disc height loss
- Fusion effect: Eliminates motion at that segment, IAR moves to adjacent levels
Q: Where is the normal IAR in the cervical spine? A: In the posteroinferior quadrant of the lower vertebral body. Abnormal IAR location outside the vertebral body suggests instability or pathology.
Regional Spinal Biomechanics
Cervical Spine Biomechanics
The cervical spine exhibits the highest mobility of all spinal regions. C5-C6 is the most mobile segment.
- Characteristic
- 40 degrees average
- Clinical Implication
- Maintains horizontal gaze
- Characteristic
- 45 degrees to horizontal
- Clinical Implication
- Allows flexion-extension and rotation
- Characteristic
- Posteroinferior body
- Clinical Implication
- Abnormal IAR = instability
- Characteristic
- 50% cervical rotation
- Clinical Implication
- At risk in RA, Down syndrome
Atlanto-axial joint allows approximately 50% of total cervical rotation. The odontoid peg is the pivot point.
Sagittal Balance and Spinopelvic Parameters
The regional curvatures above (cervical lordosis, thoracic kyphosis, lumbar lordosis) exist to keep the head balanced over the pelvis with minimal muscular energy. Global sagittal balance is governed by a small set of spinopelvic parameters, and a mismatch between them predicts pain, disability and the outcome of deformity surgery.
- Definition
- Angle between a line perpendicular to the sacral end plate at its midpoint and a line from that midpoint to the femoral head axis
- Significance
- A fixed morphological value (averages about 50 to 55 degrees) that sets the lordosis the spine should have
- Definition
- Angle between the sacral end plate and the horizontal
- Significance
- Positional; a higher sacral slope accompanies greater lumbar lordosis
- Definition
- Angle between the vertical and the line from the sacral end-plate midpoint to the femoral head axis
- Significance
- Positional; rises as the pelvis retroverts to compensate for sagittal imbalance
- Definition
- Horizontal offset of a C7 plumb line from the posterosuperior corner of S1
- Significance
- Should sit within about 5 cm; larger positive values mean forward imbalance and correlate with disability
The fundamental identity is PI equals PT plus SS. Because pelvic incidence is fixed for an individual, it dictates the ideal lumbar lordosis: a PI minus lumbar lordosis mismatch (ideally kept within about 10 degrees) is one of the strongest predictors of disability and of revision after adult deformity correction. When the spine drifts forward, the pelvis retroverts so pelvic tilt rises and the knees flex to bring the head back over the pelvis, compensation that is energy-costly and eventually fails.
Pelvic incidence is a fixed anatomical constant for each person; pelvic tilt and sacral slope are the positional variables that sum to it. Restoring lumbar lordosis to match pelvic incidence (a low PI minus lumbar lordosis mismatch) and bringing the C7 plumb line back over the sacrum are the goals of sagittal realignment.
Clinical Applications and Relevance
Application to Spinal Trauma
Understanding spinal biomechanics is essential for interpreting fracture patterns and assessing stability. The Denis three-column theory guides surgical decision-making: isolated anterior column fractures (simple compression) are often stable, while burst fractures involving anterior and middle columns require careful evaluation. Two-column disruption is the threshold for surgical stabilization in most cases.
Application to Degenerative Disease
Biomechanical principles explain the natural history of spinal degeneration. Disc degeneration leads to loss of disc height, which shifts the IAR posteriorly and increases facet loading. This creates a degenerative cascade: increased facet stress accelerates facet arthropathy, which further alters load distribution. Understanding this cascade informs treatment decisions, including motion preservation versus fusion.
- Fracture classification: Apply Denis three-column theory
- Instability assessment: Use White-Panjabi criteria
- Surgical planning: Two-column disruption guides fixation
- Neurological risk: Middle column compromise threatens canal
- Disc pathology: Intradiscal pressure guides activity modification
- Spondylolisthesis: Understand shear forces at L5-S1
- Stenosis: Facet hypertrophy from altered load distribution
- Adjacent segment disease: IAR changes after fusion
Distinguishing Injury Patterns by Failed Column
A frequent exam task is to differentiate fracture patterns by which columns fail and under what loading mode. This is the biomechanical "differential" of thoracolumbar trauma.
- Loading mode
- Axial + flexion
- Columns involved
- Anterior only (middle intact)
- Stability / key feature
- Usually stable; loss of anterior height, intact posterior wall
- Loading mode
- Axial compression
- Columns involved
- Anterior + middle
- Stability / key feature
- Retropulsion and canal compromise; stability depends on PLC
- Loading mode
- Flexion-distraction (tension)
- Columns involved
- Posterior + middle (anterior hinge)
- Stability / key feature
- Unstable; high association with hollow-viscus injury
- Loading mode
- Combined shear/rotation/flexion
- Columns involved
- All three columns
- Stability / key feature
- Highly unstable; frequent neurological deficit
Controversies and Areas of Uncertainty
Denis's three-column model is conceptually elegant but does not grade ligamentous injury or sagittal alignment. AO Spine and TLICS now lead surgical decision-making, yet column logic remains the teaching foundation. The two are complementary rather than competing.
Whether post-fusion adjacent-level degeneration reflects altered mechanics or the natural progression of spondylosis is unresolved. Hilibrand's finding of higher risk after single-level than multilevel fusion argues against a purely mechanical explanation.
Classic intradiscal pressure rankings rest on very small subject numbers (Wilke: a single volunteer). Sitting-versus-standing pressure ordering is debated, so absolute figures should be quoted with caution.
Disc arthroplasty aims to preserve the IAR and protect adjacent segments, but long-term registry evidence that it reduces clinically meaningful adjacent-segment disease compared with fusion remains contested.
Surgical Decision-Making
Biomechanical understanding informs surgical approach selection. For example, posterior fixation addresses the tension band but may not adequately restore anterior column height in burst fractures. Combined anterior-posterior approaches restore both columns. In cervical spine, understanding that C1-C2 provides 50% of rotation helps explain why C1-C2 fusion significantly limits neck rotation.
Patient Education and Rehabilitation
Nachemson's intradiscal pressure measurements provide evidence-based guidance for activity modification. Patients with disc pathology benefit from understanding that sitting flexion creates the highest disc pressure (275% of standing), while supine positioning is lowest (25%). This informs posture recommendations and lifting technique education.
Guidelines, Registries & Global Practice
Global Epidemiology and Burden
- Low back pain is the single leading cause of years lived with disability worldwide (Global Burden of Disease), driven largely by disc and motion-segment degeneration—the clinical endpoint of the biomechanical cascade described above.
- Thoracolumbar fractures cluster at the T10-L2 junction, the mechanical transition from the rib-stabilised thoracic spine to the mobile lumbar spine; burst fractures predominate in younger high-energy trauma and osteoporotic compression fractures in older low-energy injury.
- Adjacent-segment disease affects roughly one quarter of patients within 10 years of cervical fusion, a consistent finding across registry and cohort data internationally.
Side-by-Side Guidance on Instability and Classification
- Core principle
- Three columns; 2 or more disrupted = unstable; middle column pivotal
- Practical use
- Conceptual baseline for thoracolumbar fracture stability
- Core principle
- Checklist with translation/angulation thresholds plus neurology
- Practical use
- Reference radiographic instability criteria, cervical and thoracolumbar
- Core principle
- Morphology + PLC integrity + neurology, scored
- Practical use
- Operative threshold (score 5 or more); widely taught globally
- Core principle
- Morphology (A/B/C) + neurology + case modifiers
- Practical use
- International consensus language; favoured by AO-trained surgeons
- AAOS (US) and BOA / BASS (UK) endorse a biomechanically grounded, MRI-supported assessment of the posterior ligamentous complex when deciding operative versus non-operative care for thoracolumbar injury—conceptually aligned with the middle/posterior column emphasis above.
- AO Foundation / AO Spine has progressively shifted international teaching from pure column theory toward morphology-based classifications (AO Spine TLICS and subaxial cervical systems) while retaining Denis's stability logic.
- EFORT / European consensus stresses sagittal balance and segmental motion preservation as extensions of the same load-sharing principles.
High- vs Limited-Resource Practice Variation
- High-resource settings: routine MRI for PLC assessment, dynamic radiographs and occasionally upright/weight-bearing imaging to infer abnormal motion; access to motion-preserving devices (cervical and lumbar disc arthroplasty) where adjacent-segment mechanics are a concern.
- Limited-resource settings: stability decisions rely more heavily on plain radiographs, CT, and clinical examination; column theory and the White-Panjabi checklist remain robust, equipment-independent tools, and posterior instrumented fusion is the mainstay where arthroplasty implants are unavailable.
- Universal principle: regardless of setting, the same biomechanical reasoning—identify the failed column(s), assess the neutral zone/PLC, and match construct to the deforming force—governs sound surgical decision-making.
MCQ Practice Points
Q: Which structure is considered part of the middle column in the Denis three-column theory? A: Posterior longitudinal ligament (PLL) and posterior 50% of the vertebral body and disc. The middle column is critical for stability determination.
Q: In which position is intradiscal pressure highest according to Nachemson? A: Sitting with forward flexion (275% of standing). This informs patient education on posture and lifting technique.
Q: What is the White-Panjabi threshold for cervical instability in terms of translation? A: Greater than 3.5mm horizontal displacement. This criterion guides surgical decision-making in trauma and degenerative disease.
Q: What defines a functional spinal unit? A: Two adjacent vertebrae plus the intervening disc, facet joints, and all associated ligaments. It is the smallest biomechanical unit of the spine.
At a Glance
Spinal biomechanics centers on the functional spinal unit—two adjacent vertebrae plus intervening disc, facet joints, and ligaments—representing the smallest functional motion unit with 6 degrees of freedom. The Denis three-column theory defines spinal stability: Anterior column (ALL + anterior 50% of vertebral body), Middle column (PLL + posterior 50% of body), Posterior column (neural arch structures)—disruption of 2 or more columns indicates instability. The anterior column bears approximately 70% of axial load, with the nucleus pulposus behaving as an incompressible fluid distributing forces, while facet joints bear 10-30% depending on posture and guide motion patterns (sagittal in lumbar, coronal in thoracic). The instantaneous axis of rotation (IAR) normally lies within the disc space; abnormal IAR migration indicates degeneration or instability. White and Panjabi criteria quantify clinical instability: greater than 3.5mm translation or greater than 11° angulation in the cervical spine, greater than 4.5mm or greater than 20° in the thoracolumbar spine.
AMPDenis Three-Column Spine Stability
Hook:AMP up stability: 2 or more columns disrupted = unstable spine!
TRANSLATIONWhite and Panjabi Clinical Instability Criteria
Hook:TRANSLATION measurements define clinical instability in spinal imaging!
SAFERSpinal Load Distribution by Position
Hook:SAFER positions = lower intradiscal pressure (supine best, flexion worst)!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“The examiner shows a thoracolumbar burst fracture on CT. Describe the Denis three-column theory and how it guides your assessment of stability.”
“Explain the concept of instantaneous axis of rotation and how it changes in degenerative disc disease. What are the implications for adjacent segment degeneration after fusion?”
“A 45-year-old presents with chronic discogenic low back pain. Walk me through the normal mechanics of the intervertebral disc and how these change with degeneration. What is the biomechanical rationale for activity and posture advice?”
Key Concepts
- Functional spinal unit = 2 vertebrae + disc + ligaments + facets
- 6 degrees of freedom: 3 translations + 3 rotations
- IAR = instantaneous axis of rotation (normally in disc space)
- Load distribution: 70% anterior column, 10-30% facets
Denis Three-Column Theory
- Anterior = ALL + anterior 50% body + disc
- Middle = PLL + posterior 50% body + disc (KEY for stability)
- Posterior = pedicles, facets, laminae, spinous processes
- 2 or more columns disrupted = unstable
Clinical Instability Criteria
- Cervical: greater than 3.5mm translation or greater than 11 degrees angulation
- Thoracolumbar: greater than 4.5mm translation or greater than 20 degrees
- White-Panjabi criteria = gold standard
- Two-column disruption on Denis = surgical consideration
Regional Biomechanics
- Cervical: Highest mobility, C5-C6 most mobile, IAR posteroinferior body
- Thoracic: Limited motion, coronal facets, rib cage stability
- Lumbar: Highest load, sagittal facets, L4-L5 most mobile
- C1-C2: 50% cervical rotation at atlanto-axial joint
Disc Mechanics
- Nucleus pulposus: 80% water (young), incompressible fluid
- Intradiscal pressure: 275% sitting flexion, 100% standing, 25% supine
- Annulus fibrosus: Concentric lamellae, type I collagen
- Degeneration: Water loss, IAR shift, reduced shock absorption
Evidence Base and Key Studies
Denis Three-Column Concept of Thoracolumbar Injury
- Retrospective review of 412 thoracolumbar injuries introduced the middle osteoligamentous column (posterior vertebral wall, PLL, posterior annulus)
- Anterior column = ALL + anterior body and annulus; posterior column = neural arch and posterior ligamentous complex
- Mode of middle column failure correlated with both fracture type and neurological injury
- Four major patterns described: compression, burst, seat-belt (Chance), and fracture-dislocation
Stabilizing System of the Spine: Neutral Zone and Instability Hypothesis
- Defined the neutral zone as the low-resistance region of intervertebral motion around the neutral posture
- Neutral zone increases with injury and degeneration and is a more sensitive marker of instability than total range of motion
- Neutral zone decreases with muscle force across the segment and with instrumented fixation/fusion
- Proposed the three-subsystem model of stability: passive (osteoligamentous), active (muscle), and neural control
In Vivo Intradiscal Pressure in Daily Life
- Telemetric pressure transducer implanted in a non-degenerate L4-L5 disc of one volunteer recorded pressure across daily activities
- Relaxed standing 0.5 MPa, standing flexed forward 1.1 MPa, sitting unsupported 0.46 MPa, lying prone 0.1 MPa
- Lifting 20 kg with a round flexed back reached 2.3 MPa versus 1.7 MPa with flexed knees and 1.1 MPa held close to the body
- Confirmed Nachemson's classic data overall but found sitting pressure may be lower than erect standing
Stress Distribution Inside Intervertebral Discs With Age and Degeneration
- Stress profilometry of 87 cadaver lumbar discs (ages 16-87) mapped compressive stress across the mid-sagittal diameter
- Degeneration reduced the central hydrostatic nucleus diameter by about 50% and nuclear pressure by about 30%
- Functional annulus width rose by about 80% and posterior annular stress peaks by about 160%
- Load transfers from the nucleus to the posterior annulus, concentrating stress where annular pain and disruption arise