Posterior Surgical Approach to Acetabulum
- Internervous plane: Superior gluteal nerve (gluteus medius/minimus) and inferior gluteal nerve (gluteus maximus)
- Safe zone: Release short external rotators (piriformis to quadratus femoris) to mobilize sciatic nerve
- Sciatic nerve at highest risk: stays posterior to acetabulum, traction injury during retraction
- Heterotopic ossification prophylaxis MANDATORY: indomethacin 75mg daily × 6 weeks OR single-dose radiation
- Prone positioning standard but can be done lateral decubitus (facilitates surgical hip dislocation if needed)
- “Examiners expect detailed sciatic nerve anatomy: division level (60% at greater sciatic notch, 40% proximal), peroneal component lateral and more vulnerable
- “Must explain WHY prone positioning preferred (gravity assists exposure, easier sciatic nerve identification)
- “Key danger: Superior gluteal neurovascular bundle emerges above piriformis - stay inferior when releasing muscle origins
- “Post-op protocol: mobilize sciatic nerve by releasing all short external rotators from piriformis to quadratus femoris
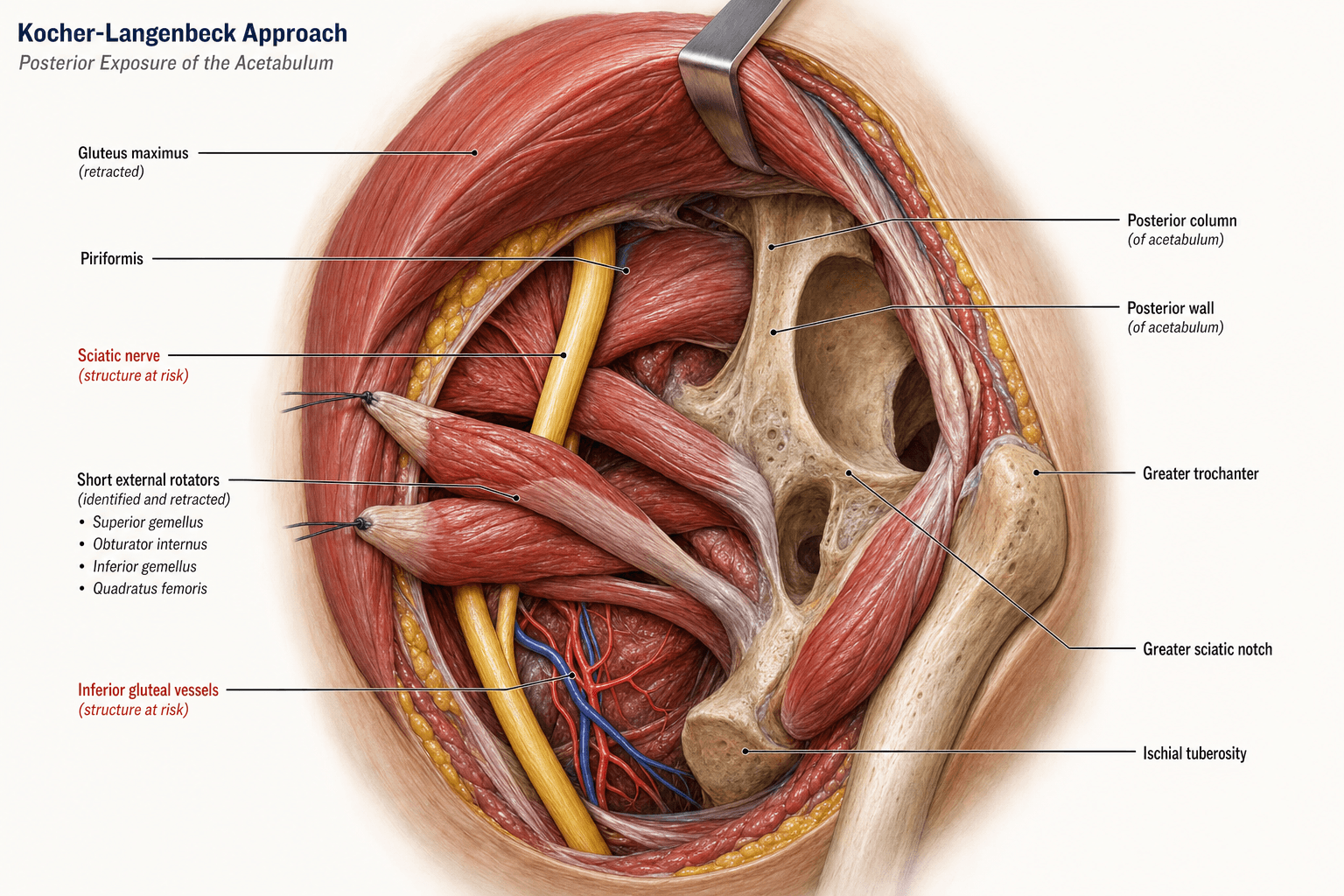
Kocher-Langenbeck Approach to the Posterior Acetabulum
Division: 60% at sciatic notch, 40% proximal. Lateral component (common peroneal) more vulnerable to stretch. Protection: Release short external rotators, avoid sharp retraction.
Location: Emerge ABOVE piriformis muscle. Safe zone: Release piriformis INFERIORLY from greater trochanter. Risk: Catastrophic bleeding if injured during muscle release.
Incidence: 10-15% without prophylaxis, 50% in head injuries. Prophylaxis: Indomethacin 75mg daily × 6 weeks (start within 24h) OR single-dose radiation (700-800 cGy). Risk factors: TBI, prolonged surgery (greater than 3h), extensive dissection.
Surgical dislocation: Trochanteric flip osteotomy (Ganz modification). Indications: Posterior wall fragments extending superiorly, femoral head impaction. Advantage: 360° acetabular visualization, protects blood supply.
Indications
Acetabular Fracture Patterns (Letournel Classification)
-
Posterior Wall Fractures
- Greater than 40% of wall involvement (CT assessment)
- Associated hip subluxation or dislocation
- Marginal impaction requiring elevation
- Failure of closed reduction
-
Posterior Column Fractures
- Displaced fractures (greater than 2-3mm)
- Posterior column with posterior wall component
- Extension into quadrilateral plate
-
Transverse Fractures
- Transtectal pattern (through superior acetabulum)
- Juxtatectal pattern (may require ilioinguinal extension)
- Infratectal pattern (low transverse fracture)
-
T-Type Fractures
- Superior stem component accessible via Kocher-Langenbeck
- May require combined approach for anterior column
-
Posterior Column + Posterior Wall
- Standard indication for Kocher-Langenbeck
- Most common pattern requiring surgery (approximately 25% of all acetabular fractures)
Contraindications
- Active deep infection overlying proposed surgical site
- Medical unfitness for prolonged surgery (ASA 4-5 with prohibitive risk)
- Severe osteoporosis (fixation challenges, consider arthroplasty)
- Delay greater than 3 weeks (increased HO risk, difficult reduction)
- Sciatic nerve palsy present for greater than 24 hours (nerve exploration urgency)
- Anterior column fractures (requires ilioinguinal or anterior approach)
- Both-column fractures (may require combined approach or ilioinguinal alone)
Alternative Approaches
- Ilioinguinal approach: Anterior column, anterior wall, both-column fractures
- Extended iliofemoral approach: Complex fractures requiring simultaneous anterior and posterior access
- Stoppa approach: Quadrilateral plate and medial wall
- Combined approaches: Both-column fractures, complex T-type patterns
The single commonest decision that brings a patient to a Kocher-Langenbeck is whether a posterior wall fracture is stable, and the topic states wall-size thresholds without the modern decision tool:
- CT wall-size estimation is imperfect. The old teaching - "fix if more than 40-50% of the wall" - is unreliable in the indeterminate zone (roughly 20-50%): small-looking walls can still be unstable, and CT-measured fragment size correlates poorly with true stability.
- Examination under anaesthesia (EUA) with dynamic stress fluoroscopy is the discriminator. With the patient relaxed under anaesthesia, the hip is taken through flexion/adduction/internal rotation under live fluoroscopy (and AP/Judet views); any subluxation or incongruity = unstable wall = ORIF via Kocher-Langenbeck, while a hip that stays congruent and concentric through the arc may be managed non-operatively with protected weight-bearing and close surveillance.
- Caveats: marginal impaction, an associated dislocation that was unstable on reduction, or a clearly large wall fragment make the hip unstable and obviate the need for a borderline stress test; EUA is for the genuinely indeterminate fragment.
Exam point: for a borderline posterior wall fracture, do not decide on CT wall-percentage alone - perform an EUA with dynamic stress fluoroscopy; subluxation/incongruity mandates Kocher-Langenbeck fixation, a congruent stable hip can be treated non-operatively.

Anatomy
Neurovascular Anatomy
- Origin: Sacral plexus (L4-S3)
- Exit: Greater sciatic notch, inferior to piriformis muscle
- Division: Common peroneal (lateral) and tibial (medial) components
- 60% divide at level of greater sciatic notch
- 40% divide proximal to notch
- Course: Runs posterior to short external rotators and posterior acetabulum
- Relation to acetabulum: 1-2 cm posterior at level of ischial tuberosity
- Vulnerability: Common peroneal component more lateral and superficial, higher traction injury risk
- Exit: ABOVE piriformis muscle through greater sciatic notch
- Course: Runs between gluteus medius and minimus
- Clinical importance: Injured if piriformis released too far superiorly or proximally
- Result of injury: Trendelenburg gait (gluteus medius/minimus weakness)
- Exit: Below piriformis muscle
- Course: Enters gluteus maximus from deep surface
- Protection: Safe during muscle splitting as vessels run longitudinally
- Course: Passes posterior to quadratus femoris
- Importance: Main blood supply to femoral head (lateral epiphyseal artery)
- Risk: Injured during anterior dissection along quadrilateral plate or with excessive retraction of quadratus femoris
Muscular Anatomy
- Origin: Ilium posterior to posterior gluteal line, sacrum, coccyx
- Insertion: Gluteal tuberosity of femur (upper fibers), iliotibial tract (lower fibers)
- Innervation: Inferior gluteal nerve
- Action: Hip extension and external rotation
- Surgical consideration: Split in line with fibers to minimize denervation
-
Piriformis
- Origin: Anterior sacrum
- Insertion: Superior medial greater trochanter
- Landmark: Superior gluteal vessels emerge ABOVE this muscle
-
Superior Gemellus
- Origin: Ischial spine
- Insertion: Greater trochanter (blends with obturator internus)
-
Obturator Internus
- Origin: Obturator membrane and pelvis
- Insertion: Greater trochanter (medial surface)
- Note: Exits pelvis through lesser sciatic foramen
-
Inferior Gemellus
- Origin: Ischial tuberosity
- Insertion: Greater trochanter (blends with obturator internus)
-
Quadratus Femoris
- Origin: Lateral ischial tuberosity
- Insertion: Quadrate tubercle (intertrochanteric crest)
- Relation: Medial circumflex femoral artery runs posterior
All five muscles are tagged with sutures at their trochanteric insertions, then released from lateral to medial (piriformis → superior gemellus → obturator internus → inferior gemellus → quadratus femoris). This mobilizes the sciatic nerve posteriorly and allows safe retraction for acetabular exposure.
Internervous Plane
Between:
- Superior gluteal nerve (L4-L5-S1): Innervates gluteus medius, gluteus minimus, tensor fascia lata
- Inferior gluteal nerve (L5-S1-S2): Innervates gluteus maximus
Clinical Significance:
The internervous plane preserves motor function to all gluteal muscles. The gluteus maximus is split in line with its fibers (minimizes denervation), while the gluteus medius and minimus are retracted superiorly to expose the short external rotators. No muscles are transected across their nerve supply, making this a true internervous approach.
Boundaries:
- Superior: Gluteus medius and minimus (retracted superiorly with superior gluteal nerve)
- Inferior: Gluteus maximus (split along fiber direction, inferior gluteal nerve intact)
- Deep: Short external rotators overlying posterior acetabulum
- Superficial: Gluteal fascia and subcutaneous tissue
Key Advantage:
By working between two different nerve territories, the approach minimizes denervation and preserves hip abductor function (critical for gait). The only muscles released are the short external rotators, which are tagged and repaired anatomically at closure to restore external rotation strength.
Approach Selection & Differential
Choosing the Surgical Approach
The Kocher-Langenbeck is one of three classic approaches; selection is driven by the fracture pattern (Letournel classification) and where the principal displacement and articular surface to be reduced lie. The single most important viva principle is: use the approach that allows direct, anatomical reduction of the dominant column/wall, and reserve extensile or combined exposures for complex patterns because they carry higher heterotopic ossification and abductor-morbidity rates.
Acetabular Approach Selection by Fracture Pattern
A common viva trap is the both-column fracture: the Kocher-Langenbeck alone is usually inadequate because the dominant pathology and articular surface lie anteriorly. Both-column fractures are typically addressed via an anterior (ilioinguinal or intrapelvic) approach, occasionally with a sequential posterior approach. Conversely, an isolated posterior wall fracture should never be approached anteriorly.
Patient Positioning
Positioning Options
- Gravity assists exposure by pulling soft tissues anteriorly
- Easier identification and protection of sciatic nerve
- Better visualization of posterior column orientation
- Allows simultaneous bilateral surgery if needed
- Surgeon stands at side of table (ergonomic)
- Cannot extend approach anteriorly if needed
- Difficult to assess hip stability intraoperatively
- Longer setup time for positioning
- Can extend to surgical hip dislocation if needed (trochanteric flip osteotomy)
- Easier to assess hip stability and range of motion
- Familiar position for hip surgeons
- Anterior ilioinguinal approach possible if required
- Soft tissues fall anteriorly, obscuring posterior exposure
- Sciatic nerve identification more difficult
- Requires pelvic positioners and careful padding
Positioning Technique (Prone)
-
General anesthesia with muscle relaxation (facilitates reduction)
-
Foley catheter placement (long procedure)
-
Position prone on radiolucent table or Jackson frame
-
Chest rolls: From clavicle to iliac crest, allowing abdominal expansion
-
Hip positioning: Slight hip extension (15-20°), neutral rotation
-
Knee: Flexed 30-45° (relaxes sciatic nerve)
-
Padding:
- Face: Prone head pillow with cutouts for eyes, nose, mouth
- Chest: Axillary rolls to protect brachial plexus
- Abdomen: Free (no pressure on abdomen)
- Anterior superior iliac spines: Padded
- Genitalia: Protected (males)
- Knees: Padded
- Ankles and feet: Padded
-
Arms: Positioned on arm boards, less than 90° abduction
Imaging Setup
- C-arm fluoroscopy: AP, obturator oblique (45°), iliac oblique (45°)
- Inlet view: Assesses anterior/posterior displacement
- Outlet view: Assesses superior/inferior displacement
- Judet views: Essential for intraoperative reduction assessment
Skin Preparation
- Prep: Chlorhexidine 2% in alcohol from mid-thoracic spine to mid-thigh
- Draping: Wide draping to allow extension of incision if needed
- Adhesive drape: Over incision site
Surgical Technique
Surface Landmarks and Incision
- Posterior superior iliac spine (PSIS): Starting point
- Greater trochanter: Palpable prominence
- Ischial tuberosity: Inferior landmark
- Sciatic nerve: Runs midpoint between greater trochanter and ischial tuberosity
- Start: 6-8 cm superior to PSIS
- Course: Curvilinear, passing over posterior aspect of greater trochanter
- Extend: Distally along posterior thigh for 8-10 cm
- Total length: 15-20 cm (extend as needed for exposure)
- Shape: Gentle curve (avoid sharp angles for wound healing)
The hip-dislocation InfoCard names the trochanteric flip but the indications, the blood-supply logic and the trade-offs are the examinable content:
- When to add it to a Kocher-Langenbeck: a superior/superomedial posterior wall or dome fragment that cannot be reduced from behind, marginal impaction high in the dome, intra-articular fragments needing removal, and associated femoral head lesions (impaction or a Pipkin femoral-head fracture) that require direct articular visualisation. It converts the posterior exposure into 360-degree access to the femoral head and acetabulum.
- Why it is safe - the digastric flip protects the MFCA: the trochanteric osteotomy fragment keeps gluteus medius/minimus proximally and vastus lateralis distally (a "digastric" flip), and crucially the obturator externus is left intact, which shields the deep branch of the medial femoral circumflex artery (the dominant femoral-head blood supply) - this is why dislocation can be performed without causing avascular necrosis (the Ganz principle).
- Trade-offs: adds trochanteric osteotomy fixation (screws/cables) with a risk of trochanteric non-union/hardware irritation, and increases heterotopic ossification risk - so reserve it for fragments/lesions you genuinely cannot address through the standard window.
Exam point: extend a Kocher-Langenbeck with a trochanteric flip osteotomy (digastric, obturator-externus-sparing to protect the deep branch of the MFCA) for superior-dome wall fragments, high marginal impaction, intra-articular debris or femoral-head lesions - accepting added trochanteric-nonunion and HO risk.

Structures at Risk
Sciatic Nerve Protection
- Location: 1-2 cm posterior to acetabulum at level of ischial tuberosity
- Division: 60% divide at greater sciatic notch, 40% proximal
- Vulnerable component: Common peroneal (lateral) more susceptible to traction injury
- Relationship: Runs between short external rotators and posterior acetabulum
- Traction: Most common - excessive or prolonged retraction
- Direct trauma: Sharp dissection or instrumentation
- Thermal: Monopolar cautery near nerve
- Compression: Post-operative hematoma
- Early identification: Locate nerve immediately after releasing short external rotators
- Mobilization: Release ALL rotators from piriformis to quadratus femoris
- Retractor placement: Blunt retractor between nerve and bone (never sharp Hohmann under nerve)
- Periodic release: Release retraction every 15-20 minutes
- Cautery discipline: Bipolar only if absolutely necessary near nerve
- Screw awareness: Check trajectory - no screws directed posteriorly toward nerve
10-20% transient palsy, 2-4% permanent deficit
Closure
Wound Closure Technique
-
Short External Rotator Repair:
- Re-approximate muscles to greater trochanter using tagged sutures
- Start with quadratus femoris (most inferior), work proximally
- Transosseous tunnels or suture anchors if bone quality poor
- Goal: Restore external rotation strength and protect sciatic nerve
-
Gluteus Maximus:
- Allow muscle to fall back together (fibers re-align)
- Minimal sutures needed
-
Fascia:
- Close fascia lata and gluteus maximus fascia with absorbable suture (0 Vicryl)
-
Subcutaneous and Skin:
- Deep dermal sutures (2-0 Vicryl)
- Skin: Staples or running subcuticular absorbable suture
- Drain: Rarely needed (if significant oozing, place 1-2 drains)
Heterotopic Ossification Prophylaxis (MANDATORY)
- Dose: 75 mg daily (or 25 mg three times daily)
- Duration: 6 weeks
- Start: Within 24 hours of surgery
- Contraindications: Peptic ulcer, renal impairment, NSAID allergy
- Dose: 700-800 cGy single fraction
- Timing: Within 72 hours of surgery (ideally within 24h)
- Technique: External beam to surgical site
- Contraindications: Pregnancy, children
Choose ONE method (not both - no additional benefit, increased side effects).
DVT Prophylaxis
- Mechanical: TED stockings, pneumatic compression devices
- Chemical: Low molecular weight heparin (e.g., enoxaparin 40 mg daily)
- Start 12-24 hours post-op if hemostasis secure
- Continue until fully mobilized (minimum 10-14 days)
- Mobilization: Early mobilization reduces VTE risk
Weight-Bearing Protocol
- First 6 weeks: Toe-touch weight-bearing only (10-20 kg)
- 6-12 weeks: Progressive weight-bearing (if radiographic healing)
- 12 weeks: Full weight-bearing (if fracture healed)
- Exceptions:
- Severe comminution: delay weight-bearing to 12 weeks
- Both-column fractures: earlier mobilization (secondary congruence)
Rehabilitation
- ROM exercises: Start early (within 48 hours)
- Hip flexion/extension, rotation
- Avoid forced abduction initially (respect short external rotator repair)
- Strengthening: Begin at 6 weeks (isometric), progress to isotonic
- Gait training: Parallel bars → crutches → stick → independent
- Return to work: 3-6 months (sedentary work earlier)

Complications
Sciatic Nerve Injury
Incidence: 10-20% (transient palsy), 2-4% (permanent deficit)
Mechanism:
- Traction injury during retraction (most common)
- Direct trauma during dissection or screw placement
- Thermal injury from cautery
- Hematoma compression post-operatively
Prevention:
- Mobilize nerve by releasing all short external rotators
- Use blunt retractors (not sharp Hohmann under nerve)
- Minimize retraction time (periodic release)
- Avoid cautery near nerve (bipolar only if necessary)
- Correct screw placement (stay intra-osseous)
Management:
- Post-operative palsy: EMG/NCS at 3-4 weeks (distinguish neurapraxia from axonotmesis)
- Neurapraxia: Observe (80-90% recover in 3-6 months)
- Axonotmesis/neurotmesis: Consider exploration if complete palsy or no recovery at 3 months
- Foot drop: AFO (ankle-foot orthosis) for ambulation
- Expected recovery: Peroneal worse than tibial (peroneal rarely recovers if complete palsy)
Heterotopic Ossification
Incidence: 10-15% (without prophylaxis), 50% (with TBI), 3-5% (with prophylaxis)
Classification (Brooker):
- Grade I: Islands of bone in soft tissues
- Grade II: Bone spurs from pelvis or femur with gap greater than 1 cm
- Grade III: Bone spurs with gap less than 1 cm
- Grade IV: Ankylosis
Risk Factors:
- Traumatic brain injury (strongest predictor)
- Delay to surgery (greater than 2 weeks)
- Prolonged surgery (greater than 3 hours)
- Extensive soft tissue dissection
- Previous HO
Prevention:
- Indomethacin 75 mg daily × 6 weeks OR radiation 700 cGy (single dose)
- Start within 24 hours
Treatment:
- Observation if asymptomatic
- Excision if: Pain, restricted ROM (less than 90° flexion), difficulty with ADLs
- Timing of excision: Wait 12-18 months (mature bone on bone scan)
- Prophylaxis for excision: Radiation preferred (indomethacin has failed once)
Superior Gluteal Nerve Injury
Incidence: Less than 5%
Mechanism:
- Injury during piriformis release (vessels emerge ABOVE muscle)
- Excessive superior retraction
Clinical Presentation:
- Trendelenburg gait (gluteus medius/minimus paralysis)
- Positive Trendelenburg test
Management:
- No treatment available (nerve not repairable)
- Compensate with cane in contralateral hand
- Gluteus maximus transfer (Mustard procedure) for severe cases
Infection
Incidence: 2-5%
Prevention:
- Prophylactic antibiotics (cefazolin 2g pre-op, continue 24h)
- Meticulous hemostasis
- Layered closure
- Drain if significant oozing
Management:
- Superficial: Antibiotics, wound care
- Deep: Surgical debridement, retain hardware if stable, 6 weeks IV antibiotics
Post-traumatic Arthritis
Incidence: 20-30% (varies with fracture pattern and reduction quality)
Risk Factors:
- Inadequate reduction (greater than 2 mm displacement)
- Femoral head injury (impaction, AVN)
- Delay to surgery
- Age greater than 40 years
Management:
- Conservative initially: NSAIDs, weight loss, activity modification
- Arthroplasty when symptomatic (THA)
- Timing: Wait minimum 1 year after fracture (allow soft tissue healing)
- Challenges: Scar tissue, bone loss, heterotopic ossification
Guidelines, Registries & Global Practice
Global Epidemiology
- Acetabular fractures have a classic bimodal distribution: high-energy injuries (road traffic and falls from height) in young adults, and low-energy fragility fractures in the elderly, the latter rising rapidly in high-income ageing populations. [24]
- Posterior wall and posterior column patterns are among the most common operatively treated patterns and are the core indication for the Kocher-Langenbeck. Associated (rather than elementary) fracture types predominate in large operative series, with both-column fractures the single commonest associated type. [2]
- Frailty and comorbidity, not just fracture pattern, increasingly drive outcome in the elderly cohort. [26]
Guidance & Consensus, Side by Side
- Position relevant to posterior acetabular fixation
- Displaced posterior wall/column and many transverse patterns: ORIF via Kocher-Langenbeck, aiming for anatomical articular reduction; HO prophylaxis after posterior/extensile approaches
- Evidence level
- Expert consensus, large case series
- Position relevant to posterior acetabular fixation
- Operative reduction for displaced/incongruent fractures; reduction accuracy and hip congruity are the principal modifiable outcome drivers; tertiary referral for complex patterns
- Evidence level
- Level III-IV cohort, consensus
- Position relevant to posterior acetabular fixation
- Pelvic and acetabular fractures should be managed in, or promptly transferred to, a specialist pelvic/acetabular unit; CT mandatory for classification and planning
- Evidence level
- Standards / expert consensus
- Position relevant to posterior acetabular fixation
- Endorses Letournel classification-led approach selection and centralisation of complex acetabular trauma to high-volume centres
- Evidence level
- Consensus, registry-supported
A consistent global theme is centralisation: complex acetabular fractures are best managed in high-volume units, reflected in the high inter-hospital transfer rates seen for these injuries. [24]
Registry & Outcome Benchmarks
There is no single dedicated acetabular-fracture registry equivalent to the arthroplasty joint registries (NJR, AJRR, AOANJRR, SHAR), so benchmarking relies on large single-surgeon and multicentre series:
- Native-hip survivorship: ~79% at 20 years after anatomical fixation (Matta/Tannast benchmark). [20]
- Functional outcome: 75-80% good/excellent at ~5 years across pooled operative series. [3]
- Reoperation: ~8% require further surgery, usually conversion to THA. [3]
For the increasing subset converted to or primarily treated with total hip arthroplasty, the arthroplasty registries (NJR, AOANJRR, AJRR, SHAR, NZJR) provide the relevant implant-survival and revision benchmarks for post-traumatic and acute "fix-and-replace" reconstructions.
Practice Variation
- Approach for both-column / quadrilateral plate: many centres have shifted from the ilioinguinal to the anterior intrapelvic (modified Stoppa) approach for medial-wall and quadrilateral-plate control, with the Kocher-Langenbeck reserved for posterior-dominant patterns.
- Elderly fractures: practice ranges from non-operative care, through ORIF, to acute total hip arthroplasty (with or without ORIF) - the choice varies by region, surgeon expertise and resource setting rather than by a single agreed algorithm.
- HO prophylaxis: routine indomethacin or single-dose radiation after posterior/extensile approaches is common but not universal; in polytrauma with long-bone fractures, radiation is preferred to avoid the indomethacin-associated nonunion risk. [22][23]
Special Populations
Elderly / Fragility Acetabular Fractures
Geriatric acetabular fractures are a rapidly growing problem. In a US Nationwide Inpatient Sample analysis, geriatric acetabular fractures rose by 67% over 18 years while traditional hip fractures fell by ~26%, reflecting an ageing population and low-energy mechanisms. [24] These injuries are characterised by anterior column and quadrilateral-plate involvement, dome impaction and the "gull sign", and are frequently transferred to tertiary centres for definitive care. [24]
- Frailty matters: sarcopenia (low psoas:lumbar vertebral index) is an independent predictor of 1-year mortality after acetabular fracture in patients over 60; combining age over 75, ISS over 14 and sarcopenia carried a 90% 1-year mortality in one cohort. [26]
- Reduced fixation durability: osteoporotic bone, dome impaction and medial comminution limit the holding power of a posterior Kocher-Langenbeck construct. Options include ORIF with buttress/quadrilateral support, the combined "fix-and-replace" (ORIF plus acute total hip arthroplasty), or primary arthroplasty with a cage/cup-cage construct.
Posterior Wall + Hip Dislocation
Posterior wall fractures usually result from a dashboard injury with posterior hip dislocation, demanding urgent reduction of the dislocation to protect femoral head vascularity. In a prospective series of 109 such combined injuries, quality of fracture reduction was the only significant predictor of radiological grade, function and post-traumatic arthritis; every hip lacking anatomical reduction developed arthritis versus 25.5% of anatomically reduced hips. [7] The traditional dogma that the dislocation must be reduced within 6 hours was less influential than reduction quality in this dataset, although emergent relocation of the dislocated hip remains standard.
Articular Cartilage Damage
Even with an anatomical bony reduction, CT "modifiers" - subchondral impaction, intra-articular fragments and comminution - predict significantly worse mid-term Harris Hip and Merle d'Aubigné scores. [25] This is the surgical rationale for elevating and grafting marginal impaction and for counselling patients that an anatomical reduction does not guarantee a normal hip.
At a Glance
The Kocher-Langenbeck approach is the workhorse posterior exposure for acetabular fracture surgery, providing direct access to the posterior column and posterior wall. Originally described by Kocher (1887) for hip arthrodesis and later modified by Langenbeck, the approach develops an internervous plane between the superior gluteal nerve (gluteus medius and minimus) and inferior gluteal nerve (gluteus maximus). The sciatic nerve runs posterior to the acetabulum and is the structure most at risk—its location must be identified early, and traction minimized by releasing all short external rotators from piriformis to quadratus femoris. Prone positioning is standard (gravity assists exposure, easier nerve identification), though lateral decubitus is acceptable. Heterotopic ossification occurs in 10-15% of cases without prophylaxis—indomethacin 75mg daily for 6 weeks (starting within 24 hours) or single-dose radiation (700-800 cGy within 72 hours) is mandatory unless contraindicated. The approach provides excellent visualization of posterior column, posterior wall, and quadrilateral plate, but anterior column and anterior wall remain poorly visualized (requires combined ilioinguinal approach for both-column fractures).
SGMSEKocher-Langenbeck - Tissue Layers
Hook:Safely Getting to My Sciatic Exposure - five layers to posterior acetabulum
SIPSStructures at Risk - Kocher-Langenbeck
Hook:SIPS water carefully - four structures that can ruin your day
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old motorcyclist has a displaced posterior wall acetabular fracture involving 50% of the wall with hip subluxation after closed reduction. You are planning a Kocher-Langenbeck approach. Walk me through your patient positioning and early steps of the approach.”
“You are 2 hours into a Kocher-Langenbeck approach for a transverse acetabular fracture. You achieve reduction and place your posterior column plate. Fluoroscopy shows a screw appears to be intra-articular on the obturator oblique view. What is your immediate management?”
Quick Facts
- Internervous plane: Superior gluteal nerve (glut med/min) and inferior gluteal nerve (glut max)
- Sciatic nerve most at risk: release all short external rotators to mobilize
- Superior gluteal vessels ABOVE piriformis - release muscle inferiorly
- HO prophylaxis mandatory: indomethacin 75mg daily × 6 weeks OR radiation 700-800 cGy
- Prone position standard - gravity assists exposure, easier nerve identification
Key Structures
- Short external rotators (superior to inferior): Piriformis, superior gemellus, obturator internus, inferior gemellus, quadratus femoris
- Sciatic nerve: 1-2 cm posterior to acetabulum, emerges inferior to piriformis, peroneal lateral and more vulnerable
- Medial circumflex femoral: posterior to quadratus femoris, main blood supply to femoral head
- Superior gluteal neurovascular bundle: exits ABOVE piriformis, injury causes Trendelenburg gait
Indications
- Posterior wall fractures (greater than 40% involvement, subluxation, marginal impaction)
- Posterior column fractures (displaced greater than 2-3mm)
- Transverse fractures (transtectal pattern)
- Posterior column + posterior wall (most common surgical pattern, approximately 25%)
Complications
- Sciatic nerve palsy: 10-20% transient, 2-4% permanent (peroneal worse prognosis than tibial)
- Heterotopic ossification: 10-15% without prophylaxis, 50% with TBI, 3-5% with prophylaxis
- Superior gluteal nerve injury: less than 5%, causes Trendelenburg gait, not repairable
- Post-traumatic arthritis: 20-30%, higher with inadequate reduction (greater than 2mm) or age greater than 40
- Infection: 2-5%, deep infection requires debridement and 6 weeks IV antibiotics
Evidence Base
Matta (1996) - Landmark Acetabular Fracture Outcomes Study
- 262 displaced acetabular fractures operated within 21 days, 255 hips followed mean 6 years (range 2-14)
- Anatomical reduction achieved in 185 hips (71%); rate fell with greater fracture complexity, older age and longer injury-to-surgery interval
- Overall clinical result excellent 40%, good 36% (76% good/excellent), fair 8%, poor 16%
- Clinical result closely tracked the radiographic result; outcome worsened by femoral head injury, older age and operative complications, and improved by anatomical reduction and femoral head-roof congruity
- Femoral head osteonecrosis 3%, progressive head wear 5%, conversion to THA 6% at follow-up
Giannoudis et al (2005) - Meta-Analysis of Operative Acetabular Fracture Treatment
- Meta-analysis of 3670 operatively treated displaced acetabular fractures
- Between 75% and 80% achieved an excellent or good result at a mean of 5 years
- Post-traumatic osteoarthritis was the commonest long-term complication (~20%)
- Heterotopic ossification and femoral head avascular necrosis each occurred in less than 10%
- Only 8% required a further operation, usually conversion to hip arthroplasty
Burd, Lowry & Anglen (2001) - HO Prophylaxis: Indomethacin vs Radiation RCT
- Prospective RCT, 166 acetabular fractures via posterior/extensile approach: indomethacin (25 mg three times daily × 6 weeks) vs single-fraction 800 cGy radiation within 72h
- Brooker Grade III-IV heterotopic ossification: indomethacin 11% (8/72) vs radiation 4% (3/78) - not significant (p=0.22)
- All 16 untreated patients developed HO, with 38% Grade III-IV - confirming prophylaxis is effective
- No prophylaxis-related complications in either arm; grade I-III HO did not reduce hip range of motion except in flexion
- Overall Grade III-IV prevalence 7% in treated vs 38% in untreated
Burd, Hughes & Anglen (2003) - Indomethacin Increases Long-Bone Nonunion
- 112 patients with an acetabular fracture plus a concomitant long-bone fracture, randomised to radiation, indomethacin or no prophylaxis
- Long-bone nonunion: 26% with indomethacin vs 7% without indomethacin (radiation or none) - p=0.004
- NSAID-mediated impairment of fracture callus is the proposed mechanism
Moed et al (2003) - Postoperative CT Predicts Posterior Wall Outcome
- 67 operatively treated posterior wall fractures assessed by postoperative 2D CT and plain Judet radiographs
- Plain films graded 65/67 as 'anatomic', but CT revealed offset greater than 2 mm in 11 hips and gaps of 2 mm or more in 52 hips
- Residual fracture gap of 10 mm or more, or total gap area of 35 mm-squared or more, was associated with a poor result
- Strong association between final CT/radiographic grade and clinical outcome; osteonecrosis was the other main risk factor
Tannast, Najibi & Matta (2012) - 20-Year Hip Survivorship
- 816 operatively fixed displaced acetabular fractures from a single surgeon over 26 years
- Cumulative 20-year survivorship of the native hip (endpoint THA or arthrodesis) was 79%
- Independent negative predictors: non-anatomical reduction, age over 40, anterior dislocation, postoperative roof incongruence, posterior wall involvement, acetabular impaction, femoral head cartilage lesion, initial displacement 20 mm or more, and use of the extended iliofemoral approach
- Provides benchmark survivorship data and a nomogram for predicting early THA