ATFL and CFL Insufficiency
- ATFL: Weakest lateral ligament. Resists inversion in plantarflexion. Most commonly injured.
- CFL: Injured in severe sprains. Resists inversion in dorsiflexion. Crosses both ankle and subtalar joints.
- Anterior Drawer: Tests ATFL integrity. Compare to contralateral side.
- Talar Tilt: Tests CFL integrity. Performed in neutral dorsiflexion.
- Brostrom-Gould: Direct ATFL repair + inferior extensor retinaculum augmentation. Gold standard surgical treatment.
- “ATFL is weakest - always injured first (ACP order)
- “Anterior drawer tests ATFL, talar tilt tests CFL
- “Rehabilitation first - majority stabilize without surgery
- “Brostrom repair is gold standard (85-90% success)
- “Reconstruction for revision, heavy athletes, or generalized laxity
Lateral ligament injury order: ATFL → CFL → PTFL (weakest to strongest).
- ATFL is weakest - injured with inversion in plantarflexion (most common mechanism).
- CFL is next - injured with greater force (inversion in dorsiflexion). Crosses ankle AND subtalar joints.
- PTFL is strongest - only injured in severe ankle dislocations.
- Remember: ACP = Anterior, Calcaneofibular, Posterior (weakest to strongest).
Overview/Epidemiology
Lateral ankle instability is the most common sports injury worldwide, affecting athletes across all sports and age groups.
Epidemiology
- 23,000 ankle sprains per day in the United States
- 1 per 10,000 person-days in general population
- Up to 30% of all sporting injuries
- Most common in basketball, soccer, and volleyball
- 20-40% of acute sprains develop chronic instability
- Risk factors: incomplete rehabilitation, ligamentous laxity
- 55% have residual symptoms at 6 months
- Recurrence rate without treatment: 70-80%
- Peak incidence: 15-35 years (active population)
- Equal male:female ratio in general population
- Higher female incidence in specific sports
- Prior ankle sprain strongest risk factor
Types of Instability
- Mechanical Instability: Objective ligament laxity on stress testing
- Functional Instability: Subjective feeling of giving way despite normal stress tests
- Combined: Most patients have elements of both
Risk Factors for Chronic Instability
- Previous ankle sprain (strongest predictor)
- Incomplete or inadequate rehabilitation
- Generalized ligamentous laxity (Beighton score greater than 4)
- High-demand sports (basketball, soccer, netball)
- Hindfoot varus malalignment
- Cavovarus foot deformity
- Peroneal weakness or dysfunction
Pathophysiology and Mechanisms
Lateral Ankle Ligament Complex
The lateral ankle ligaments originate from the lateral malleolus and provide stability against inversion and anterior translation of the talus.
- Origin
- Anterior border of lateral malleolus
- Insertion
- Talar neck (anterolateral)
- Function
- Resists anterior translation + inversion in plantarflexion
- Injury Order
- 1st (weakest)
- Origin
- Tip of lateral malleolus
- Insertion
- Lateral calcaneus
- Function
- Resists inversion in dorsiflexion; crosses ankle + subtalar
- Injury Order
- 2nd
- Origin
- Medial surface of lateral malleolus
- Insertion
- Posterior talus
- Function
- Resists posterior translation; strongest ligament
- Injury Order
- 3rd (rarely injured)
ATFL Anatomy (Most Important)
- Length: 20-25mm
- Width: 10-12mm
- Orientation: Horizontal in plantarflexion → becomes vertical in dorsiflexion
- Variants: 1-3 bands (2 bands most common)
- Strength: Weakest of the three (58-90N failure load)
CFL Anatomy
- Length: 20-25mm
- Crosses two joints: Ankle AND subtalar (unique feature)
- Orientation: 10-45° posterior to long axis of fibula
- Key relationship: Lies deep to peroneal tendons
- Clinical significance: CFL injury affects subtalar stability
Biomechanics of Injury
The typical mechanism is inversion injury in plantarflexion:
- In plantarflexion, the narrower posterior talus sits in the mortise → less bony stability
- ATFL becomes the primary restraint → first to fail
- With continued force, CFL then fails
- PTFL only fails with severe trauma/dislocation
Dynamic Stabilizers
- Peroneus longus and brevis: Primary dynamic stabilizers
- Extensor digitorum longus: Secondary support
- Proprioceptive afferents: Critical for neuromuscular control
- Peroneal reaction time: Delayed in chronic instability
Classification Systems
Ankle Sprain Grading
- Pathology
- Microscopic tear, stretch injury
- Clinical Findings
- Mild swelling, tenderness
- Stability
- Stable
- Treatment
- RICE, early mobilization
- Pathology
- Partial macroscopic tear
- Clinical Findings
- Moderate swelling, ecchymosis
- Stability
- Mild laxity
- Treatment
- Brace 4-6 weeks, physio
- Pathology
- Complete rupture ATFL ± CFL
- Clinical Findings
- Severe swelling, ecchymosis
- Stability
- Frank instability
- Treatment
- Brace, physio ± surgery
Grade I and II injuries typically heal with conservative treatment. Grade III injuries may require surgical intervention if chronic instability develops.
Clinical Assessment
History
Key Questions:
- Initial injury: mechanism, treatment, rehabilitation
- Symptoms: giving way episodes, pain, swelling
- Functional limitation: sports, uneven ground, stairs
- Prior treatment: physiotherapy duration, bracing
- Red flags: locking (loose body), medial pain (deltoid), persistent swelling (OCD)
Physical Examination
Observation
- Swelling: lateral ankle, anterolateral gutter
- Ecchymosis: may indicate recent episode
- Hindfoot alignment: varus predisposes to lateral sprains
- Cavus foot: associated with instability
- Muscle wasting: peroneal atrophy suggests chronic injury
Inspection findings help assess the chronicity and severity of instability.
Investigations
Imaging Protocol
Standard Views
- Weight-bearing AP: Mortise alignment, OCD
- Mortise view: Lateral clear space
- Lateral: Talar dome, anterior impingement
Stress Radiographs (If Indicated)
- Anterior drawer stress: Greater than 10mm translation significant
- Talar tilt stress: Greater than 10° or greater than 5° vs. contralateral
- Useful for objective documentation
- Compare to contralateral side
Standard weight-bearing views are essential first-line imaging.
Associated Pathology to Exclude
- Frequency
- 20-25%
- Investigation
- MRI, CT
- Clinical Significance
- Address at surgery
- Frequency
- 15-20%
- Investigation
- MRI, ultrasound
- Clinical Significance
- May need concurrent repair
- Frequency
- 10-15%
- Investigation
- Lateral X-ray, MRI
- Clinical Significance
- Debride at arthroscopy
- Frequency
- 5-10%
- Investigation
- X-ray, MRI
- Clinical Significance
- Different treatment
- Frequency
- Variable
- Investigation
- Stress views
- Clinical Significance
- Consider reconstruction
Differential Diagnosis of the "Unstable" or Painful Lateral Ankle
- Key Distinguishing Feature
- Recurrent giving-way; positive anterior drawer/talar tilt
- Best Test
- Clinical stress tests; stress radiographs
- Why It Matters
- Index diagnosis - guides rehab vs surgery
- Key Distinguishing Feature
- Retromalleolar pain/clicking; pain on resisted eversion, not true giving-way
- Best Test
- Dynamic ultrasound; MRI
- Why It Matters
- Needs tendon repair/groove deepening, not ligament repair alone
- Key Distinguishing Feature
- Deep ankle pain, catching/locking, effusion rather than instability
- Best Test
- MRI / CT
- Why It Matters
- Often coexists; must address arthroscopically at surgery
- Key Distinguishing Feature
- Pain proximal to joint line; positive external rotation/squeeze test
- Best Test
- ER stress test; weight-bearing CT
- Why It Matters
- Different treatment - stabilisation, not lateral repair
- Key Distinguishing Feature
- Anterolateral pain on dorsiflexion, no objective laxity
- Best Test
- MRI; diagnostic arthroscopy
- Why It Matters
- Treated by debridement, not ligament repair
- Key Distinguishing Feature
- Hindfoot 'rolling' on uneven ground; CFL involvement
- Best Test
- Broden/stress views; clinical exam
- Why It Matters
- May need reconstruction crossing the subtalar joint
Management Algorithm
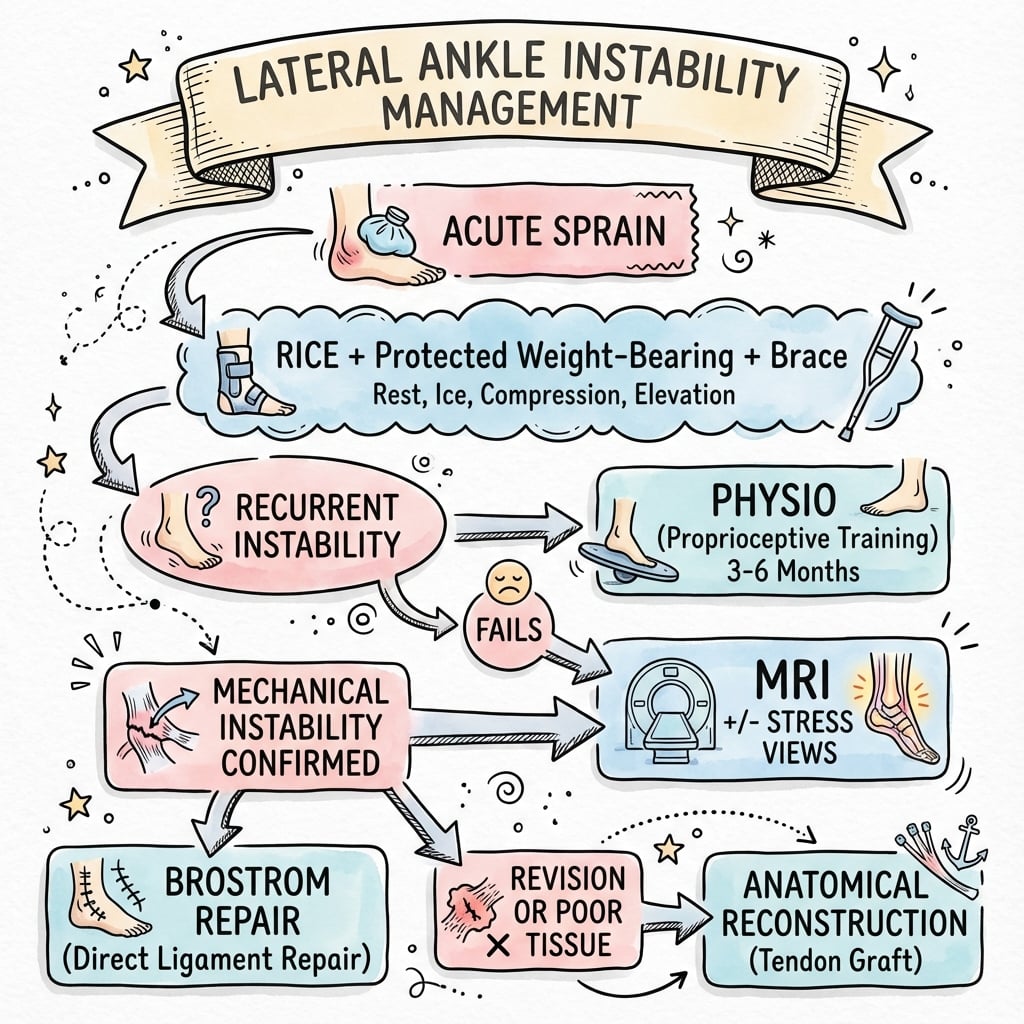
Treatment Decision Framework
First-Line for ALL Patients
Duration: 3-6 months minimum before considering surgery
Components:
-
Proprioceptive Training
- Wobble board exercises
- Single-leg stance progressions
- Sport-specific balance training
-
Peroneal Strengthening
- Resisted eversion exercises
- Theraband programs
- Functional strengthening
-
Ankle Bracing
- Semi-rigid brace for sport
- Lace-up brace for daily activities
- Taping for specific activities
-
Activity Modification
- Avoid uneven terrain initially
- Gradual return to sport
Success Rate: 70-80% of patients stabilize with rehabilitation alone.
Conservative treatment remains the cornerstone of management.
- All patients: Rehabilitation first (3-6 months)
- Persistent symptoms: Brostrom-Gould repair
- Failed Brostrom/Generalized laxity/Heavy athlete: Anatomic reconstruction
- Revision surgery: Consider reconstruction with allograft
Surgical Technique
Brostrom-Gould Repair (Gold Standard)
Patient Positioning
- Position: Supine with bump under ipsilateral hip
- Tourniquet: High thigh (250-300mmHg)
- Leg position: Slight internal rotation for lateral access
Equipment
- Standard foot and ankle set
- Suture anchors (2.4-3.0mm)
- Non-absorbable braided suture
- Fluoroscopy (optional)
Approach
- Curvilinear incision over lateral malleolus
- Length: 4-6cm
- Identify and protect superficial peroneal nerve branches
Proper positioning and nerve protection are essential for successful repair.
The superficial peroneal nerve is at risk with lateral ankle approaches. It typically crosses the surgical field 5-10cm proximal to the tip of the lateral malleolus. Always identify and protect this nerve to avoid sensory deficit.
Complications
Complications by Type
Intraoperative Complications
- Incidence
- 2-5%
- Prevention
- Careful dissection, identify before incision
- Management
- Neurolysis, reassurance
- Incidence
- 1-2%
- Prevention
- Posterior incision extension awareness
- Management
- Reassurance (usually neuropraxia)
- Incidence
- 5-10%
- Prevention
- Pre-op MRI assessment
- Management
- Convert to reconstruction
- Incidence
- Rare
- Prevention
- Proper technique, bone quality assessment
- Management
- Re-anchor or transosseous sutures
Nerve identification is the key to preventing intraoperative complications.
Postoperative Care
Rehabilitation Protocol
Immobilization Phase
- Wound healing
- Pain and swelling control
- Prevent DVT
- Below-knee backslab or CAM boot
- Non-weight bearing or touch weight bearing
- Elevation, ice
- Ankle pumps (within splint if able)
- Wound check at 10-14 days
- Remove sutures
- Transition to CAM boot
Early immobilization protects the healing repair.
Expected Outcomes
- Brostrom-Gould
- 85-90%
- Anatomic Reconstruction
- 80-90%
- Brostrom-Gould
- 85-95%
- Anatomic Reconstruction
- 80-90%
- Brostrom-Gould
- 5-10%
- Anatomic Reconstruction
- 5-15%
- Brostrom-Gould
- 4-6 months
- Anatomic Reconstruction
- 6-9 months
Outcomes
Results by Treatment Type
- 70-80% stabilize without surgery
- Best results with supervised physiotherapy
- Proprioceptive training key to success
- Peroneal strengthening essential
- Bracing for sport may be permanent
- 85-90% good/excellent results
- Gold standard surgical treatment
- Preserves subtalar motion
- Lower revision rate than non-anatomic
- Return to sport: 4-6 months
- 80-90% good results
- Reserved for failures, laxity, heavy athletes
- Longer rehabilitation (6-9 months)
- Allograft reduces donor site morbidity
- Higher revision rate than primary Brostrom
Prognostic Factors
- Single ligament injury (ATFL only)
- Good tissue quality
- Normal hindfoot alignment
- Compliant patient
- Supervised rehabilitation
- Combined ATFL + CFL injury
- Generalized ligamentous laxity
- Hindfoot varus or cavovarus
- Associated OCD
- Poor compliance
Guidelines, Registries & Global Practice
Global Epidemiology
- Ankle sprain is among the most common musculoskeletal injuries worldwide; the lateral ankle sprain is the dominant subtype (Doherty meta-analysis of 181 prospective studies).
- Incidence is higher in females than males (13.6 vs 6.94 per 1000 exposures) and in indoor/court sports (basketball, volleyball, netball, handball).
- Approximately 20-40% of acute sprains progress to chronic instability; the Cochrane review cites ~10-20% developing chronic lateral instability.
- A prior sprain remains the single strongest predictor of recurrence regardless of region or healthcare setting.
Side-by-Side Guidelines & Consensus
- Diagnostic Position
- History of ≥1 significant sprain plus recurrent giving-way, recurrent sprains, or feelings of instability
- Management Emphasis
- Distinguish mechanical vs functional instability; structured outcome measures
- Diagnostic Position
- Clinical diagnosis; stress imaging for objective laxity
- Management Emphasis
- Functional treatment + neuromuscular/proprioceptive rehabilitation first-line for acute and chronic injury
- Diagnostic Position
- Ottawa rules for acute imaging; clinical exam primary
- Management Emphasis
- Early functional rehabilitation; surgery for refractory instability
- Diagnostic Position
- Stress views and MRI for surgical planning
- Management Emphasis
- Anatomic repair (Broström-Gould) as gold standard; reconstruction for failures/laxity
- Diagnostic Position
- Exclude associated osteochondral and syndesmotic injury
- Management Emphasis
- Anatomic restoration of ATFL/CFL footprints; address concomitant pathology
Registry & Outcome Notes
- Unlike arthroplasty, lateral ankle stabilisation is not tracked in national joint registries (NJR, AOANJRR, SHAR); evidence derives from cohort series, meta-analyses, and consensus statements rather than registry survivorship.
- Reported recurrence after anatomic repair is broadly 5-15%, higher with generalised laxity - the rationale for suture-tape augmentation or reconstruction in selected patients.
High- vs Limited-Resource Practice Variation
- High-resource settings: Ready access to MRI, stress imaging, arthroscopy, and suture-tape/InternalBrace augmentation; arthroscopic Broström increasingly favoured for lower wound morbidity.
- Limited-resource settings: Diagnosis is largely clinical (Ottawa rules, stress testing); supervised neuromuscular rehabilitation and bracing carry the management burden, with open anatomic repair the mainstay where surgery is indicated.
- The conservative-first, rehabilitation-led pathway is universal and equally valid across all settings - the major global driver of good outcomes.
The Varus Hindfoot: Why the Ligament Repair Alone Fails, and When to Add a Calcaneal Osteotomy
The topic repeatedly names hindfoot varus and cavovarus as a risk factor for lateral sprains and as an unfavourable prognostic sign, yet the crucial surgical corollary is easy to miss: a soft-tissue repair performed on a malaligned foot is set up to fail.
The Biomechanical Problem
In a varus/cavovarus hindfoot the ground-reaction force passes medial to the subtalar joint axis, generating a constant inversion (supination) moment across the ankle and hindfoot. This does two things:
- It predisposes to the original recurrent sprains (the lateral ligaments are chronically loaded).
- After surgery it places a persistent stretching force on a Broström-Gould repair, so an isolated soft-tissue repair on an uncorrected varus hindfoot is prone to gradual stretch-out and recurrent instability. Failing to recognise and correct hindfoot varus is one of the leading causes of an otherwise technically sound repair failing.
Sorting Out the Deformity (routed workup)
The deformity assessment itself belongs to the cavovarus work-up (see the dedicated cavovarus-foot topic): standing hindfoot alignment, a standing hindfoot-alignment/long-axial radiograph, and the Coleman block test to decide whether the hindfoot varus is forefoot-driven (a plantarflexed first ray that corrects on the block = flexible) or a fixed hindfoot varus (does not correct). What is this topic's job is deciding what bony procedure, if any, must accompany the ligament surgery.
The Surgical Corollary
- Fixed hindfoot varus: add a lateralising/valgus-producing calcaneal osteotomy (Dwyer lateral closing-wedge, or a lateral-translation/Z-type osteotomy) to move the weight-bearing axis lateral to the subtalar joint and unload the lateral repair.
- Forefoot-driven varus (positive Coleman block — corrects on the block): a dorsiflexion (dorsal closing-wedge) osteotomy of the first metatarsal addresses the plantarflexed first ray.
- Peroneal balance: consider a peroneus longus-to-brevis transfer where longus overdrive (plantarflexing the first ray) is driving the varus, strengthening eversion.
- The ligament repair/reconstruction is then done on a balanced, plantigrade foot.
If the examiner shows a patient with recurrent lateral instability and a varus/cavovarus hindfoot, the trap is to offer a Broström in isolation. State that you would realign first: a lateralising Dwyer calcaneal osteotomy for a fixed hindfoot varus (and/or a dorsiflexion first-metatarsal osteotomy for a forefoot-driven, Coleman-positive varus), because an uncorrected inversion moment stretches out any lateral ligament repair. Correct the alignment, then stabilise the ligaments.
Concurrent Subtalar Instability: Recognise It and Recreate the CFL
The topic flags subtalar instability in its differential ("hindfoot rolling on uneven ground; CFL involvement; may need reconstruction crossing the subtalar joint"), notes the CFL crosses both the ankle and subtalar joints, and that the talar tilt test "also tests subtalar stability" — but never develops how to recognise or treat it. Because it shares the CFL as a restraint, subtalar instability frequently coexists with lateral ankle instability and is commonly under-recognised.
Recognising It
- Symptoms: a sense of the hindfoot "rolling" or giving way on uneven ground, sometimes with medial-hindfoot ache, that persists despite an apparently competent ATFL. Patients may describe instability that feels deeper or more posterior than a pure ankle giving-way.
- Examination: hard to isolate clinically because ankle and subtalar motion couple; look for a medial subtalar glide/tilt and reproduction of the "rolling" sensation. CFL insufficiency (positive talar tilt) should raise suspicion.
- Imaging: Broden views and subtalar stress radiographs are described to demonstrate talocalcaneal tilt, but normative values are poorly standardised and the tilt is difficult to separate from ankle (talar) tilt — so the diagnosis remains substantially clinical. CT/MRI mainly exclude other hindfoot pathology and coalition.
Treating It
- Rehabilitation first, exactly as for the lateral ankle — proprioceptive and peroneal work.
- Surgery: because the CFL is the shared restraint, an isolated ATFL-only Broström is inadequate; the reconstruction must extend distally to the calcaneus and recreate the CFL. An anatomic reconstruction reproducing both the ATFL and CFL footprints is preferred.
- Historical caution: the older non-anatomic tenodeses (Chrisman-Snook, Evans) did restrain subtalar motion, but at the cost of subtalar stiffness and later arthritis — a key reason anatomic techniques that preserve subtalar motion are now favoured.
If a patient still gives way on uneven ground despite a competent ATFL repair, think concurrent subtalar instability. The unifying anatomical fact is that the CFL spans both joints — so the answer is to recreate the CFL (an anatomic reconstruction extending to the calcaneus), not simply to re-tension the ATFL. Avoid non-anatomic tenodeses, which stiffen the subtalar joint and predispose to arthritis.
Controversies and Areas of Uncertainty
- Meta-analyses show comparable stability with lower wound morbidity arthroscopically
- Longer-term durability and learning-curve data still maturing
- No high-level RCT establishes clear superiority of either approach
- Biomechanically stronger and allows earlier loading
- Clinical benefit over standard repair is small and short-term
- Concern about over-constraint and cost-effectiveness remains unresolved
- Higher failure with direct repair in generalised laxity (Beighton ≥4)
- Optimal threshold to choose graft reconstruction is not standardised
- Augmented repair may bridge the gap but lacks long-term comparative data
Unresolved Questions
- Early surgery in elite athletes: Whether acute repair of complete Grade III ruptures in high-level athletes shortens return-to-sport versus functional treatment remains debated; most evidence still favours rehabilitation first.
- Optimal rehabilitation dose: The ideal duration, supervision intensity, and balance/neuromuscular protocol are not standardised across guidelines.
- Defining "failed" conservative treatment: The 3-6 month threshold is pragmatic rather than evidence-defined.
- Role of weight-bearing CT and dynamic imaging in routine assessment is evolving and not yet consensus practice.
MCQ Practice Points
Q: Which lateral ankle ligament is injured first during an inversion injury?
A: The ATFL (anterior talofibular ligament) is the weakest and most commonly injured. It is injured with inversion in plantarflexion - the most common ankle sprain mechanism. Remember ACP order: Anterior → Calcaneofibular → Posterior (weakest to strongest).
Q: A patient has a positive talar tilt test but negative anterior drawer. Which ligament is injured?
A: The CFL (calcaneofibular ligament) is injured. The talar tilt test assesses CFL integrity (inversion stress in dorsiflexion), while the anterior drawer tests ATFL. This pattern is unusual as ATFL is typically injured first, so consider other pathology.
Q: What does the Gould modification add to the original Brostrom repair?
A: The Gould modification adds augmentation with the inferior extensor retinaculum (IER). The IER is advanced over the ATFL repair and anchored to the fibula, providing additional restraint and improved proprioceptive input. This is now standard with all Brostrom repairs.
Q: When is anatomic reconstruction preferred over Brostrom repair for lateral ankle instability?
A: Reconstruction is indicated for: (1) Failed Brostrom repair, (2) Generalized ligamentous laxity (Beighton score greater than 4), (3) Heavy/high-demand athletes, and (4) Poor quality native tissue. These patients have higher failure rates with direct repair.
Q: What is unique about the calcaneofibular ligament compared to other lateral ankle ligaments?
A: The CFL crosses two joints - both the ankle joint AND the subtalar joint. This means CFL injury affects subtalar stability as well as ankle stability. The ATFL and PTFL only cross the ankle joint.
Self-Assessment Quiz
At a Glance Table
- Details
- Chronic mechanical and/or functional instability of the lateral ankle complex
- Details
- 23,000 ankle sprains/day (US); 20-40% develop chronic instability
- Details
- ATFL (most common), CFL, PTFL (rare)
- Details
- Inversion injury, typically in plantarflexion
- Details
- Anterior drawer (ATFL), Talar tilt (CFL)
- Details
- Rehabilitation: proprioceptive training + peroneal strengthening
- Details
- Brostrom-Gould repair (85-90% success)
- Details
- Failed Brostrom, generalized ligamentous laxity, revision, heavy athletes
ACPLateral Ligaments - ACP
Hook:ACP = Anterior to Posterior = Weakest to Strongest. Like the alphabet, A comes first (injured first).
ATEStress Test Interpretation - ATE
Hook:ATE my ankle! Know which ligament each stress test assesses.
SCARSCAR - Lateral Ankle Surgery Complications
Hook:SCAR reminds you of the main complications that can leave a mark on outcomes.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 25-year-old basketball player presents with recurrent left ankle 'giving way' episodes despite 6 months of physiotherapy. He reports 3-4 episodes per month during games. Examination shows positive anterior drawer test compared to the contralateral side. What is your assessment and management plan?”
“A 30-year-old female netball player presents 18 months after a Brostrom repair with recurrent instability. She has hypermobile joints (Beighton score 6/9). Stress testing shows persistent ATFL laxity. How do you approach this case?”
“A 22-year-old soccer player sustains an inversion injury during a match. He has significant lateral swelling, ecchymosis, and tenderness over the ATFL. He cannot weight bear. Anterior drawer appears positive but is difficult to assess due to guarding. How do you manage this acute injury?”
ANATOMY - ACP
- ATFL: Weakest, injured first, resists inversion in plantarflexion
- CFL: Crosses ankle AND subtalar, injured second
- PTFL: Strongest, only injured in dislocations
- ACP order = Anterior to Posterior = Weakest to Strongest
EXAMINATION
- Anterior drawer = ATFL (anterior translation)
- Talar tilt = CFL (inversion in dorsiflexion)
- External rotation = Syndesmosis (NOT lateral ligaments)
- Always compare to contralateral side
TREATMENT ALGORITHM
- FIRST: Rehabilitation 3-6 months (majority stabilize)
- SECOND: Brostrom-Gould repair (85-90% success)
- THIRD: Reconstruction if failed Brostrom/laxity/heavy athlete
- Gould modification = IER augmentation (always do this)
KEY NUMBERS
- 20-40%: Acute sprains → chronic instability
- 70-80%: Stabilize with rehabilitation alone
- 85-90%: Good results with Brostrom-Gould
- 4-6 months: Return to sport after Brostrom
Evidence Base
- Original description of direct delayed anatomic repair of ruptured lateral ligaments
- Established that scarred ligament ends could be re-apposed years after injury with good results
- Foundation for all modern anatomic lateral ankle stabilization
- Added advancement of the inferior extensor retinaculum (IER) over the repaired ATFL
- Reinforces the repair and limits inversion, adding a proprioceptive contribution
- Converted the Broström into the 'Broström-Gould' construct
- Meta-analysis of 181 prospective studies; ankle sprain incidence higher in females than males (13.6 vs 6.94 per 1000 exposures)
- Highest incidence in indoor/court sports; children at higher risk than adolescents or adults
- Lateral ankle sprain was the most common subtype overall
- Consensus selection criteria defining chronic ankle instability (CAI) for research and practice
- Requires a history of at least one significant sprain plus recurrent 'giving way', recurrent sprains, or feelings of instability
- Standardised CAI definition to harmonise the literature
- Seven randomised trials; insufficient high-quality evidence to favour any single surgical or conservative technique
- After surgical reconstruction, early functional rehabilitation gave earlier return to work and sport than 6 weeks of immobilisation
- Chronic lateral instability follows roughly 10-20% of acute sprains
- Six comparative studies; arthroscopic repair gave slightly higher AOFAS and Karlsson scores and lower VAS pain
- No difference in postoperative anterior drawer, talar tilt, or overall complications
- Wound-related complications were significantly lower with arthroscopic repair (OR 0.25)
- 28 patients with generalised ligamentous laxity (Beighton ≥4); 2-year follow-up
- FAOS improved 63.2 to 90.6 and talar tilt 16.2° to 3.6°; anterior translation 12.1 mm to 4.2 mm
- Only 1 patient (3.6%) had recurrent subjective and mechanical instability
- 64 CLAI patients with generalised joint laxity (Beighton ≥4); 24-month follow-up
- No difference in functional scores or stress radiographs between arthroscopic and open repair
- Arthroscopic group returned to work earlier; failure rates 23.3% vs 16.1% (not significant)