Intra-Articular | Nonunion Risk | ORIF Often Required
- INTRA-ARTICULAR fracture (elbow and wrist joint)
- Greater than 2mm displacement = surgical indication
- High risk of nonunion due to synovial fluid bathing fracture
- Late complications: nonunion, malunion, cubitus valgus, tardy ulnar nerve palsy
- Lateral approach - do NOT dissect posterior (blood supply)
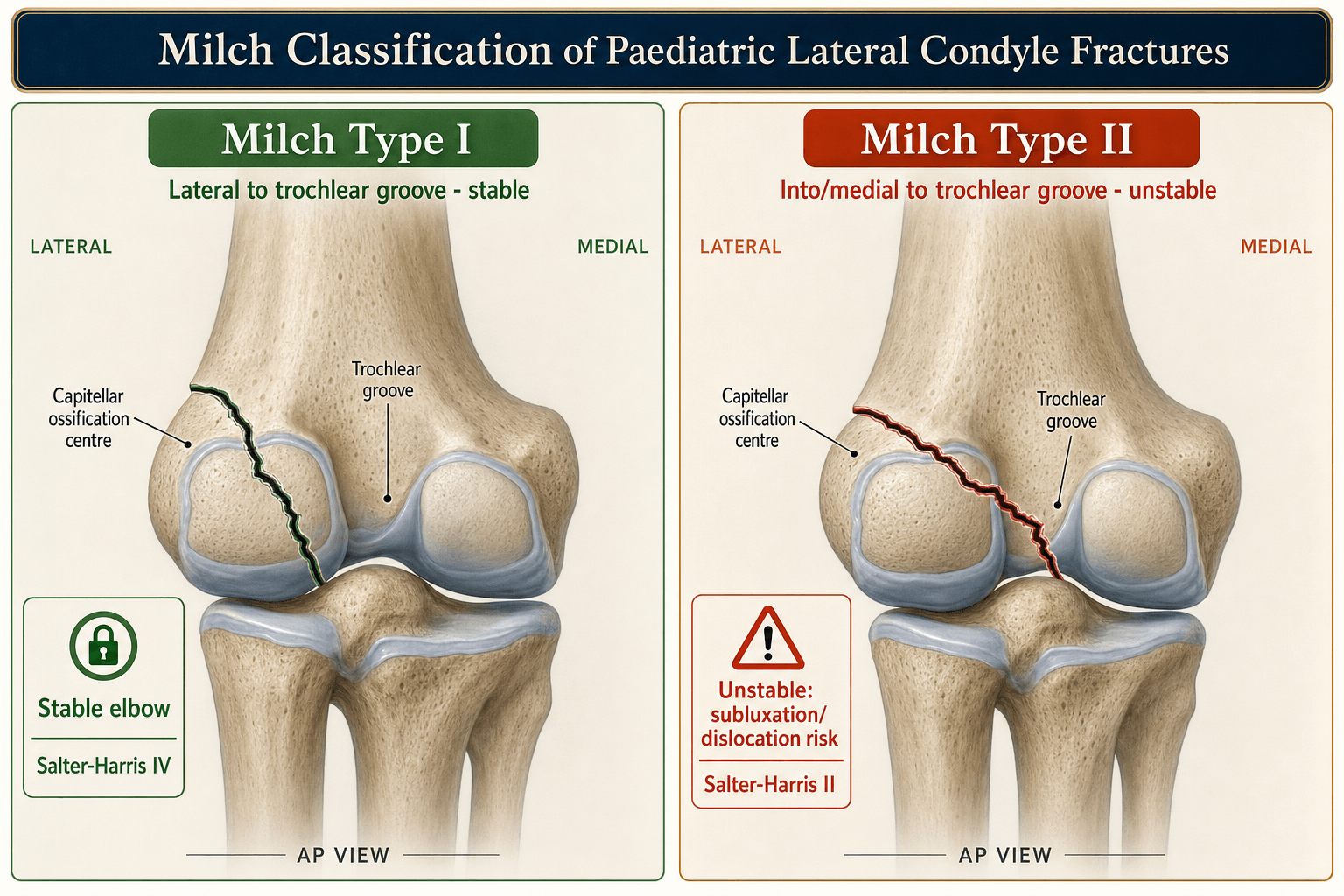
- “Milch Type I = Salter-Harris IV (lateral to trochlear ridge)
- “Milch Type II = Salter-Harris II (through trochlear ridge, unstable)
- “Nonunion causes lateral spur and cubitus valgus
- “Tardy ulnar nerve palsy occurs years later due to valgus
Crosses the articular surface. Unlike supracondylar, this is an intra-articular fracture. Anatomic reduction required to prevent degenerative changes and angular deformity.
Greater than 2mm displacement = ORIF. Less than 2mm can be treated non-operatively but needs close follow-up (can displace in cast). Some advocate surgery for greater than 2mm on any view.
Synovial fluid prevents healing. Fracture bathed in synovial fluid from elbow joint. Combined with pull of extensor origin, high risk of nonunion. This is why surgery is often needed.
Delayed complication of cubitus valgus. Nonunion causes lateral spur and progressive valgus. Ulnar nerve is stretched over time. May present years later with ulnar neuropathy.
- Displacement
- Less than 2mm
- Articular Step
- Intact cartilage hinge
- Treatment
- Cast, weekly XR for 3 weeks
- Displacement
- 2-4mm
- Articular Step
- Gap but some contact
- Treatment
- ORIF with K-wires
- Displacement
- Greater than 4mm
- Articular Step
- Complete articular disruption
- Treatment
- ORIF with K-wires
Overview and Epidemiology
The lateral condyle fracture is the second most common pediatric elbow fracture (after supracondylar) but has a higher complication rate. It is intra-articular, prone to nonunion, and can lead to progressive cubitus valgus and tardy ulnar nerve palsy.
- 15% of pediatric elbow fractures
- Second only to supracondylar
- Peak age 5-7 years
- Slight male predominance
- Usually fall onto outstretched hand
- Lateral condyle (capitellum + part of lateral trochlea)
- Extends through articular surface
- Physis involved (Salter-Harris pattern)
- Lateral collateral ligament attaches to fragment
Anatomy and Biomechanics
The blood supply to the lateral condyle enters posteriorly. During ORIF, do NOT dissect or strip the soft tissues from the posterior aspect of the fragment. Use an anterior/lateral approach and visualize the articular surface from the front.
Key Anatomical Points
- Capitellum (articulates with radial head)
- Lateral portion of trochlea (variable extent)
- Lateral epicondyle (common extensor origin)
Enters posteriorly. The fragment has NO anterior blood supply once fractured. Protect posterior soft tissues during surgery.
Extensor muscles (attached to lateral epicondyle) pull the fragment distally and rotate it, causing displacement.
Classification Systems
Weiss/Jakob Classification (Most Clinically Useful)
- Displacement
- Less than 2mm
- Description
- Minimally displaced, cartilage hinge intact
- Treatment
- Long arm cast 90°, weekly XR x3
- Displacement
- 2-4mm
- Description
- Partial articular disruption, some contact
- Treatment
- ORIF with K-wires
- Displacement
- Greater than 4mm
- Description
- Complete displacement, no articular contact
- Treatment
- ORIF with K-wires
This classification is more practical for guiding treatment than Milch.
1 OUT, 2 THROUGHMilch Classification
Hook:Type 1 stays OUT (lateral), Type 2 goes THROUGH (trochlear ridge)
Clinical Assessment
- Fall mechanism (FOOSH with varus stress)
- Time since injury
- Any swelling or deformity
- Neurovascular symptoms
- Previous elbow injury
- Lateral elbow swelling and tenderness
- Ecchymosis (may be extensive)
- Full neurovascular exam
- Check elbow stability (compare to opposite)
- ROM likely limited by pain
In young children, the lateral condyle ossific nucleus may not yet be visible (capitellum ossifies around age 1-2). An effusion (positive fat pad sign) with lateral tenderness but no obvious fracture line suggests an occult lateral condyle fracture. Obtain an internal oblique view, consider ultrasound/MRI or arthrogram, or treat as a fracture and follow closely with repeat films.
Differential Diagnosis of the Painful, Swollen Paediatric Elbow
- Mechanism / Age
- FOOSH, varus stress; peak 5-7y
- Key Distinguishing Feature
- Lateral metaphyseal fragment, intra-articular, displaces in cast
- Pitfall to Avoid
- Underestimating displacement on AP/lateral only
- Mechanism / Age
- FOOSH, hyperextension; peak 5-7y
- Key Distinguishing Feature
- Transverse metaphyseal line, anterior humeral line abnormal, extra-articular
- Pitfall to Avoid
- Missing concurrent NV injury (AIN/median)
- Mechanism / Age
- Valgus/throwing; older child 9-14y
- Key Distinguishing Feature
- Medial fragment, may be incarcerated in joint
- Pitfall to Avoid
- Forgetting to count ossification centres (CRITOE)
- Mechanism / Age
- Birth/NAI in infants under 3y
- Key Distinguishing Feature
- Whole epiphysis displaced medially, radiocapitellar line maintained to capitellum
- Pitfall to Avoid
- Mistaking for elbow dislocation; consider non-accidental injury
- Mechanism / Age
- FOOSH valgus
- Key Distinguishing Feature
- Radial head angulation, point tenderness over radial neck
- Pitfall to Avoid
- Attributing all lateral pain to the condyle
- Mechanism / Age
- Axial pull; toddler 1-4y
- Key Distinguishing Feature
- No swelling, refusal to use arm, normal radiographs
- Pitfall to Avoid
- Over-imaging; reduces with supination-flexion
Use the CRITOE ossification sequence (Capitellum, Radial head, Internal/medial epicondyle, Trochlea, Olecranon, External/lateral epicondyle) to interpret the immature elbow. Comparison views of the contralateral elbow are invaluable - a displaced ossific fragment lateral to the metaphysis confirms the diagnosis when the cartilaginous fracture itself is radiolucent.
Investigations
Radiological Investigations
- What to Check
- Fragment size and displacement
- Key Finding
- Measure gap on AP
- What to Check
- Rotation of fragment
- Key Finding
- Fragment often rotates posteriorly
- What to Check
- Better visualization of fracture
- Key Finding
- 45° internal rotation
- What to Check
- Opposite elbow
- Key Finding
- Helps in young children
Internal oblique view is particularly helpful as it places the fracture line in profile.




Management

The threshold for surgery is greater than 2mm displacement. Some authors are more aggressive and operate on any fracture greater than 2mm on ANY view. Non-operative fractures need weekly X-rays for 3 weeks as they can displace in cast.
Non-Operative Management (Weiss Type I)
Displacement less than 2mm, intact cartilage hinge.
Long arm cast in 90 degrees elbow flexion.
Weekly X-rays for first 3 weeks. If any displacement occurs, convert to ORIF.
Cast for 4-6 weeks until union confirmed.
Close follow-up is mandatory. Up to 20% of initially non-displaced fractures may displace.
Traditional fixation is with smooth K-wires to avoid physeal injury. Some surgeons use a cannulated screw in older children (near skeletal maturity) for more stable fixation. Screws should NOT cross the physis in young children.
Surgical Technique Considerations
ORIF Technique for Lateral Condyle
Supine with arm on hand table.
Lateral/Kocher interval between anconeus and ECU.
Visualize the articular surface from ANTERIOR. Do NOT strip soft tissues from posterior fragment.
Reduce articular surface anatomically. The metaphyseal reduction usually follows.
Two smooth K-wires, usually 1.6mm. Divergent configuration. Cross fracture site but avoid olecranon fossa.
STAY ANTERIORSurgical Approach
Hook:STAY ANTERIOR - blood supply from posterior, don't strip it!
Complications
Complications of Pediatric Lateral Condyle Fractures
- Incidence
- Most serious
- Cause
- Synovial fluid, inadequate fixation
- Management
- ORIF if early, osteotomy if late
- Incidence
- Common with nonunion
- Cause
- Lateral physeal arrest
- Management
- Osteotomy if symptomatic
- Incidence
- Delayed (years)
- Cause
- Progressive valgus stretches nerve
- Management
- Ulnar nerve transposition
- Incidence
- Common
- Cause
- Prolonged immobilization
- Management
- Physiotherapy, rarely need release
- Incidence
- Rare
- Cause
- Posterior soft tissue stripping
- Management
- Prevention - protect blood supply
- Incidence
- With late reduction
- Cause
- Missed or delayed diagnosis
- Management
- Osteotomy if functional limitation
Tardy ulnar nerve palsy is a delayed complication occurring years after the original injury. It develops because nonunion leads to cubitus valgus, which progressively stretches the ulnar nerve around the medial epicondyle. Treatment is ulnar nerve transposition (often anterior subcutaneous) and may require corrective osteotomy.
Two More Recognised Sequelae
A lateral bony prominence (spur) and mild lateral condylar overgrowth is extremely common after healing of a lateral condyle fracture — even well-reduced ones — and is almost always benign and cosmetic. The key clinical task is to reassure the family that it is NOT a nonunion: it represents periosteal/healing new bone, the fracture is united, and it usually remodels and becomes less prominent with growth. Surgery is rarely needed for the spur alone.
A late "fishtail" (V-shaped) notch of the central distal humerus between the capitellum and trochlea, caused by osteonecrosis or growth arrest of the lateral trochlea following lateral condyle (or supracondylar/T-condylar) fractures, and aggravated by posterior soft-tissue stripping at surgery. Often an incidental radiographic finding years later, but it can cause pain, clicking, restricted motion or progressive deformity. Recognising it explains why preservation of the posterior blood supply is critical during ORIF.
NUTSLateral Condyle Complications
Hook:Don't go NUTS - treat lateral condyle fractures properly!
Postoperative Care
Post-Operative Protocol
Long arm backslab in 90 degrees elbow flexion. Neurovascular checks. Elevate and ice.
Check wound and pin sites. X-ray to confirm maintained reduction. Convert to long arm cast.
X-ray to assess healing. If good callus, may remove pins (in clinic). Continue cast.
X-ray confirms union. Remove cast. Begin active ROM exercises. Avoid passive stretching.
Full return to activities. Final check of motion, alignment, carrying angle. Follow long-term if any concern.
Outcomes and Prognosis
Prognosis Depends on Prompt Diagnosis and Treatment
- Fracture recognized early
- Displacement greater than 2mm treated surgically
- Anatomic articular reduction achieved
- Union confirmed before discharge from follow-up
- Diagnosis delayed
- Fracture displaces in cast and missed
- Nonunion develops
Guidelines, Registries & Global Practice
- 15-20% of paediatric elbow fractures; second only to supracondylar
- Peak age 5-7 years; slight male predominance
- Mechanism: fall on outstretched hand with varus (pull-off) or push-off load
- Roughly 40-60% are displaced enough to warrant surgery across published series
- National arthroplasty registries (NJR, AJRR, AOANJRR, SHAR) do not capture paediatric trauma
- Evidence base is observational cohorts and society position statements, not registry survival data
- No randomized trial defines the exact displacement threshold
Side-by-Side Society Guidance
- Operative Threshold
- Over 2mm or articular incongruity
- Fixation Emphasis
- Smooth K-wires; arthrogram to confirm reduction
- Distinct Point
- CRPP acceptable for many displaced fractures
- Operative Threshold
- Over 2mm; close cast surveillance under 2mm
- Fixation Emphasis
- K-wires standard; structured follow-up
- Distinct Point
- Emphasis on early review to detect late displacement
- Operative Threshold
- Displacement / rotation or articular step
- Fixation Emphasis
- Anatomic articular reduction, lag screw near maturity
- Distinct Point
- Protect posterior blood supply, anterolateral exposure
- Operative Threshold
- Over 2mm on maximal-displacement view
- Fixation Emphasis
- K-wires; selective screws
- Distinct Point
- Internal oblique view to grade displacement
- Routine internal oblique views, fluoroscopy and intraoperative arthrogram
- Increasing use of closed reduction and percutaneous pinning
- MRI/CT available for occult or complex fractures
- Day-case surgery with structured pin-site care and early clinic review
- Higher proportion of late presentation, nonunion and cubitus valgus
- Reliance on plain radiographs and comparison views; arthrogram less available
- Open reduction more common where image intensifiers are scarce
- Reconstruction (osteosynthesis +/- osteotomy +/- ulnar transposition) forms a larger share of workload
Across every major society the core principles are identical: this is an intra-articular, nonunion-prone fracture; over 2mm displacement or articular incongruity is operative; reduction must be anatomic; the posterior blood supply must be preserved; and close radiographic follow-up is mandatory because non-displaced fractures can displace in cast. The main variation is the closed-versus-open debate and the precise 2mm-versus-4mm threshold.
Special Considerations
Management of Nonunion
ORIF with bone grafting still possible. Better outcomes than late reconstruction.
In situ fixation with bone grafting or corrective osteotomy. The nonunion may be too sclerotic for direct healing without osteotomy.
May require supracondylar osteotomy for angular correction plus ulnar nerve transposition.
Controversies and Areas of Uncertainty
Traditional teaching mandated open reduction for displacement over 2-4mm to confirm articular congruity. Song's prospective series and later cohorts show closed reduction with percutaneous pinning can succeed even in fully displaced/rotated fractures, with intraoperative arthrogram to confirm joint reduction. The trade-off is the inability to directly inspect the articular surface.
The operative threshold is debated. Many use over 2mm on the maximally displaced view; others reserve open surgery for at least 4mm (articular disruption), treating 2-4mm fractures with closed pinning after arthrogram. Weiss data link the 4mm point to articular incongruity and higher complications.
Smooth K-wires remain standard to spare the open physis, but cannulated/headless screws are increasingly used near maturity for compression and earlier motion. Comparative data show no clear outcome superiority of one implant over another.
Leaving pins percutaneous (exposed) allows clinic removal but carries pin-site infection risk; buried pins reduce infection but need a second anaesthetic for removal. Practice varies; pin-site infection is usually superficial and resolves with oral antibiotics and pin removal.
Whether to repair an established, minimally symptomatic nonunion is contested. Historic concern about osteonecrosis and stiffness favoured observation, but contemporary series (e.g. Eamsobhana 2015) report high union rates and good Mayo scores even with mild symptoms, supporting earlier osteosynthesis - ideally before the nonunion is neglected beyond ~28 months. Aggressive dissection of a fibrosed, displaced fragment still risks avascular necrosis, so meticulous posterior soft-tissue preservation is essential.
MCQ Practice Points
Q: What is the displacement threshold for ORIF of pediatric lateral condyle fractures? A: 2mm. Greater than 2mm displacement, or any rotation of the fragment, requires ORIF. Less than 2mm can be treated non-operatively with close follow-up.
Q: In the Milch classification, what distinguishes Type I from Type II lateral condyle fractures? A: Exit point relative to trochlear ridge. Type I exits LATERAL to the trochlear ridge (elbow stable). Type II exits THROUGH the trochlear ridge (elbow potentially unstable). Type II is more common.
Q: Why should posterior soft tissue stripping be avoided during ORIF of lateral condyle fractures? A: Blood supply enters posteriorly. The blood supply to the lateral condyle fragment comes from posterior. Stripping posterior soft tissues risks avascular necrosis.
Q: Why is lateral condyle fracture at high risk of nonunion? A: Synovial fluid bathes the fracture. The intra-articular location means synovial fluid prevents hematoma formation and bone healing. This is compounded by the deforming force of the extensor muscles.
Q: What is tardy ulnar nerve palsy and how does it relate to lateral condyle fractures? A: Delayed ulnar neuropathy due to progressive cubitus valgus. Nonunion leads to lateral physeal arrest and valgus deformity, which stretches the ulnar nerve over years. Treatment is transposition.
Q: What is the standard fixation for pediatric lateral condyle fractures? A: 2 divergent smooth K-wires. This avoids physeal damage. Screws may be considered in older children near skeletal maturity.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 6-year-old child presents after a fall with lateral elbow pain and swelling. X-rays show a lateral condyle fracture with 3mm displacement. How would you manage this?”
“A 10-year-old presents 4 months after a fall. He was treated at another hospital with casting. He now has an established nonunion of the lateral condyle with 15 degrees of cubitus valgus. There is no ulnar nerve dysfunction. How would you manage this?”
“A 5-year-old child presents with a lateral condyle fracture with 1.5mm displacement on the AP view and no displacement on the lateral view. How would you manage this?”
Key Facts
- 15% of pediatric elbow fractures (2nd most common)
- INTRA-ARTICULAR fracture
- High nonunion risk (synovial fluid)
- Blood supply from posterior - do NOT strip
Management
- Less than 2mm: cast with weekly XR
- Greater than 2mm: ORIF
- Fix with 2 divergent K-wires
- Lateral approach, stay ANTERIOR
Classification
- Weiss I: less than 2mm - non-op
- Weiss II: 2-4mm - ORIF
- Weiss III: greater than 4mm - ORIF
- Milch I: lateral to trochlear ridge
Complications - NUTS
- Nonunion (most common serious)
- Ulnar nerve palsy (tardy - years later)
- Tilted (cubitus valgus)
- Stiffness
Key Surgical Points
- Lateral approach, stay ANTERIOR
- Visualize articular surface
- 2 divergent smooth K-wires
- Do NOT strip posterior soft tissues
Evidence Base and Key Studies
Weiss et al. - Displacement-Based Classification Predicts Complications
- 158 operatively treated fractures - largest operative series at the time
- Type I less than 2mm; Type II at least 2mm with intact cartilage (arthrogram); Type III at least 2mm with disrupted articular surface
- Complication rate 11% (Type II) versus 34% (Type III) - more than 3-fold higher
- Every Type II fracture had under 4mm displacement; every Type III had at least 4mm on radiographs
Song et al. - Five-Stage Classification and Treatment Algorithm
- Prospective study of 63 unstable fractures graded on four radiographic views
- Closed reduction and internal fixation succeeded in 13 of 17 stage-3 and 30 of 40 stage-4 fractures
- Open reduction reserved for residual displacement over 2mm after closed attempt
- No osteonecrosis, nonunion, malunion, or physeal arrest
Song et al. - Internal Oblique Radiograph for Assessment
- Prospective study of 54 fractures with AP, lateral, and oblique views
- 70% showed different displacement on AP versus internal oblique view
- Internal oblique view demonstrated more displacement in 30 cases and more instability in 20
- Classification should use the greatest displacement across at least three views
Song et al. - CRIF for Completely Displaced/Rotated Fractures
- Prospective, three Level I centres, 24 completely displaced and rotated (Jakob 3) fractures
- 18 of 24 (75%) reduced to within 2mm by closed technique with percutaneous fixation
- Closed reduction failed in 3 - converted to open reduction
- No osteonecrosis, nonunion, malunion, or physeal arrest