Subscapularis Attachment | Posterior Dislocation Association | Medial Displacement
- Subscapularis attachment: The only rotator cuff tendon on the lesser tuberosity
- Medial displacement: Deforming force pulls fragment medially
- Posterior dislocation: Always rule out associated posterior dislocation (seizures/electrocution)
- Axillary view essential: Shows lesser tuberosity profile anteriorly
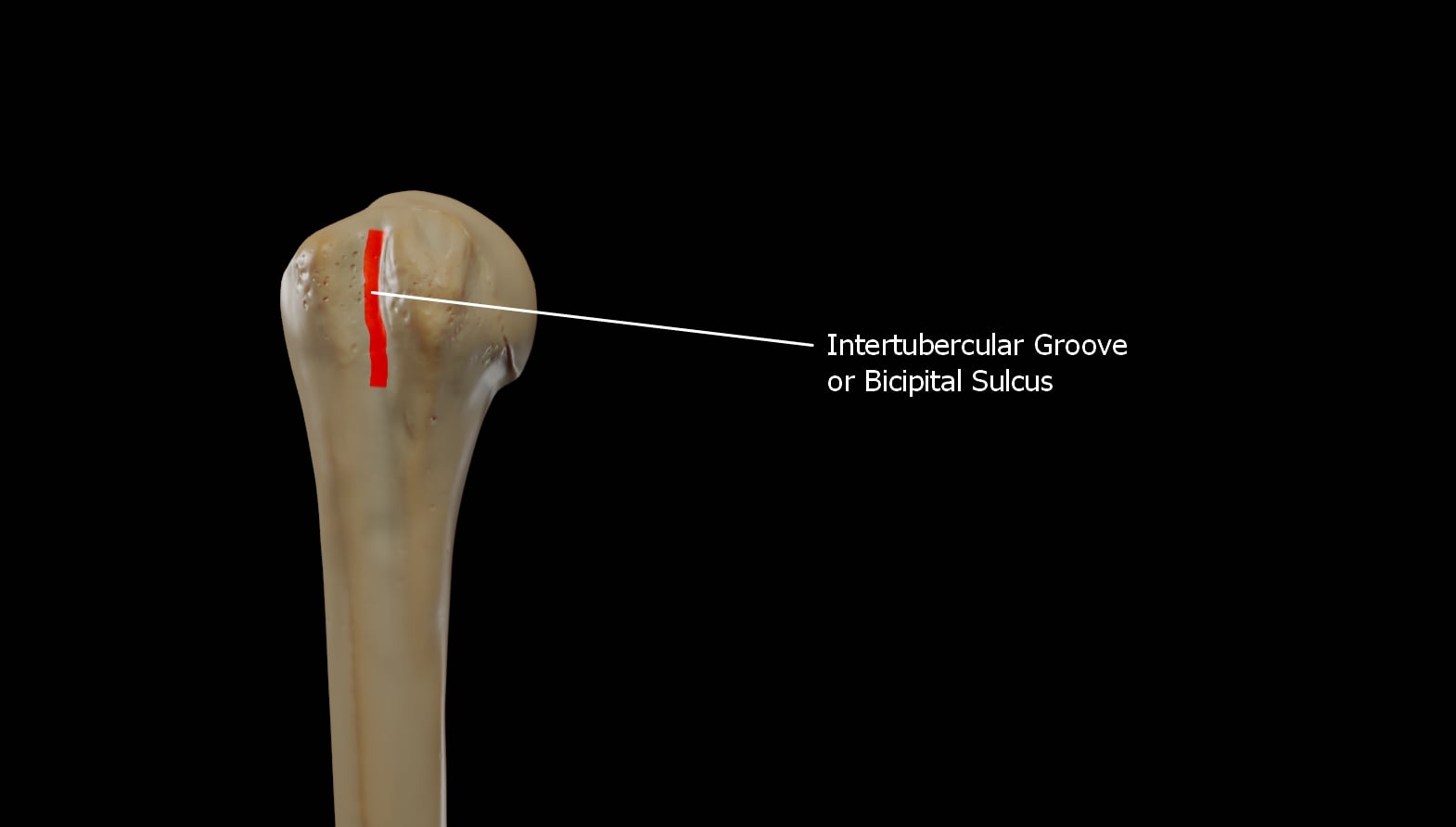
- Biceps tendon: Medial to GT, lateral to LT (in groove) - at risk during fixation
- “Modified Axillary view helps visualize lesser tuberosity profile
- “Chronic malunion can cause mechanical block to internal rotation
- “Open reduction requires deltopectoral approach
- “Hardware must avoid the bicipital groove
Mandatory Check: Any lesser tuberosity fracture should raise high suspicion for a posterior shoulder dislocation until proven otherwise. Check axillary view carefully.
Internal Rotation: The lesser tuberosity is the insertion for the subscapularis. Avulsion leads to loss of internal rotation strength (Lift-off test, Belly press).
Bicipital Groove: The long head of biceps runs in the groove lateral to the lesser tuberosity. It is at risk during injury and surgical fixation.
AP View Miss: Isolated lesser tuberosity fractures can be easily missed on standard AP views as the fragment overlaps the humeral head. Axillary view is diagnostic.
- Displacement
- Less than 5mm
- Symptoms
- Minimal weakness
- Treatment
- Non-operative (sling)
- Displacement
- Greater than 5mm
- Symptoms
- Weakness / Block
- Treatment
- Surgical fixation
- Displacement
- Variable
- Symptoms
- Locked shoulder
- Treatment
- Reduce dislocation, then reassess
- Displacement
- Healed medial
- Symptoms
- Internal rotation block
- Treatment
- Excision or Osteotomy
LESSERLesser Tuberosity Features
Hook:LESSER tuberosity fractures are tied to Subscapularis function and Posterior dislocation!
LIGHTPosterior Dislocation Signs
Hook:Look for the LIGHT to diagnose the associated posterior dislocation.
Overview
Lesser tuberosity fractures are rare isolated injuries but significant due to their association with posterior shoulder dislocations and subscapularis function. The lesser tuberosity is situated on the anterior aspect of the proximal humerus and serves as the insertion site for the subscapularis tendon.
Incidence:
- Rare as isolated injury (2-5% of proximal humerus fractures)
- Commonly associated with posterior shoulder dislocation (15-30%)
- Often missed on initial presentation
- Posterior glenohumeral dislocation (avulsion)
- Seizures or electric shock (violent muscle contraction)
- Forced external rotation of adducted arm
- Direct blow to anterior shoulder (rare)
Anatomy and Pathophysiology
Anatomical Considerations
- Anterior projection of proximal humerus.
- Medial border of bicipital groove.
- Distal to anatomical neck.
- Smaller than greater tuberosity.
- Lateral: Bicipital groove (Biceps Long Head).
- Lateral to groove: Greater Tuberosity.
- Medial: Articular surface.
Review normal anatomy to identify subtle displacements.
Classification
Classification
Based on Fragment Size & Displacement:
- Type I: Minimally displaced (less than 5mm), small avulsion.
- Type II: Displaced (greater than 5mm), large fragment involving articular surface.
- Type III: Comminuted fracture.
- Type IV: Associated with posterior dislocation.
This descriptive system aids in surgical planning.
- Description
- Small fragment
- Key Feature
- Subscapularis intact/avulsed
- Treatment
- Fix if greater than 5mm
- Description
- Posterior dislocation
- Key Feature
- Locked head possible
- Treatment
- Reduce first
- Description
- Anatomic position
- Key Feature
- Stable
- Treatment
- Non-operative
- Description
- Fragmented
- Key Feature
- Poor bone stock
- Treatment
- Suture anchors
There is no widely used specific alphanumeric classification for isolated lesser tuberosity fractures equivalent to Neer's for GT. They are generally described by fragment size and displacement (less than or greater than 5mm).
Clinical Assessment
History and Physical Examination
History
- History of seizure? (Must ask).
- Electric shock?
- Trauma with arm in adduction/internal rotation.
- Sensation of "pop" or instability.
- Anterior shoulder pain.
- Weakness in internal rotation.
- Pain with overhead activity.
Mechanism of injury is a strong predictor of this fracture pattern.
Examination
- Anterior swelling/bruising.
- Posterior prominence (if dislocated) - flattening of anterior shoulder.
- Limited external rotation (painful stretch of subscap).
- Limited internal rotation (weakness or block).
- Locked internal rotation suggests posterior dislocation.
- Lift-off test: Positive (unable to lift hand off back).
- Belly press test: Positive (wrist flexion/elbow drop).
- Bear hug test: Sensitive for upper subscapularis.
Physical exam must confirm joint reduction first.
Investigations
Imaging Studies
- True AP (Grashey).
- Scapular Y.
- Axillary View (Essential).
- AP: Fragment often superimposed on head (double density) or seen medially.
- Axillary: Shows profile of lesser tuberosity anteriorly. Confirms glenohumeral reduction.
- Scapular Y: Helps rule out dislocation.
Standard series is usually sufficient for initial screening.

Differential Diagnosis
Distinguishing the Lesser Tuberosity Fracture
- Key Distinguishing Feature
- Bony fragment medial to bicipital groove; avulsion mechanism
- Best Test
- Axillary radiograph and CT
- Key Distinguishing Feature
- Tendon retraction without a bony fragment; older or overhead athlete
- Best Test
- MRI; lift-off and belly-press
- Key Distinguishing Feature
- Locked internal rotation, empty glenoid, reverse Hill-Sachs
- Best Test
- Axillary view and CT
- Key Distinguishing Feature
- Fragment lateral to groove; arm in external rotation
- Best Test
- AP and axillary radiograph
- Key Distinguishing Feature
- Pain over groove, no bony fragment; positive Speed/Yergason
- Best Test
- MRI or ultrasound
- Key Distinguishing Feature
- Global passive restriction, no trauma or fragment
- Best Test
- Clinical; normal radiograph
The single most useful discriminator on imaging is the position of the fragment relative to the bicipital groove: a lesser tuberosity fragment sits medial to the groove, a greater tuberosity fragment lateral to it.
Management Algorithm
Treatment Decision Making
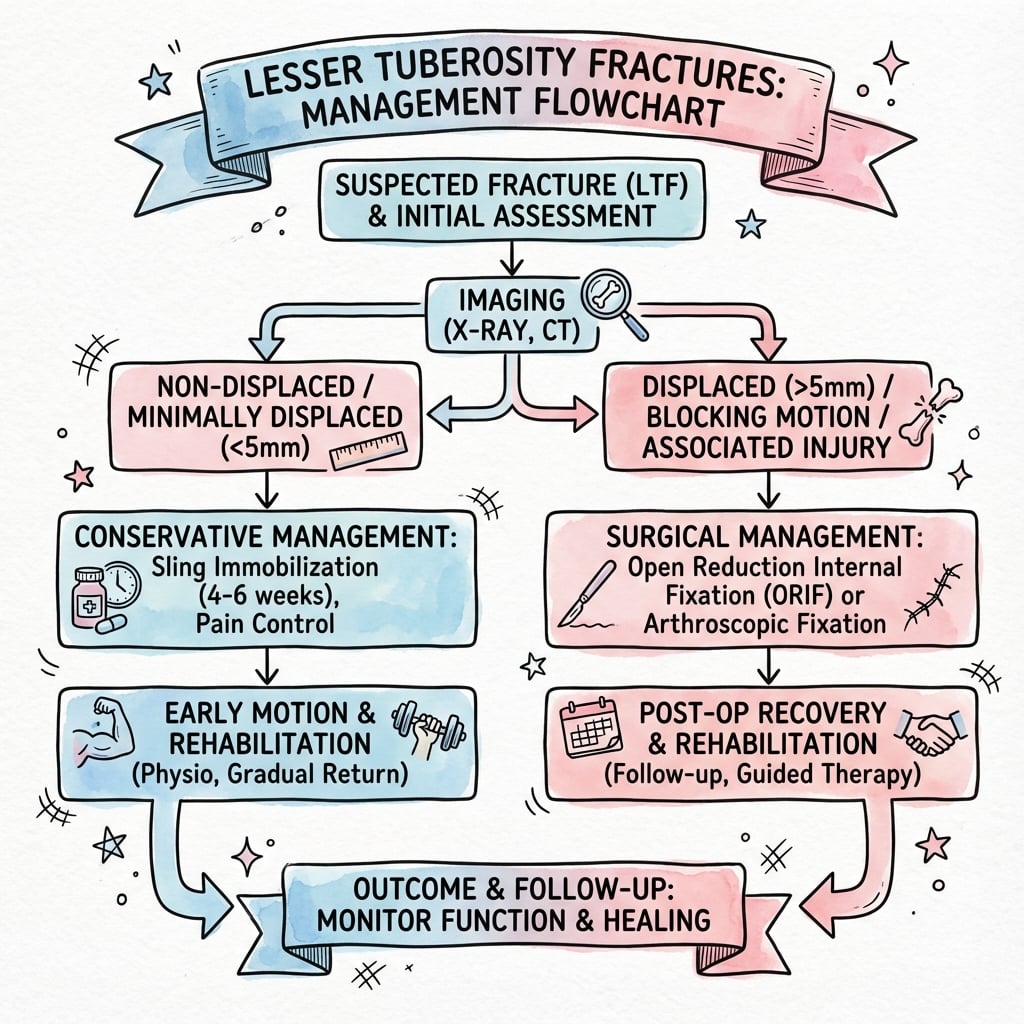
- Displacement less than 5mm.
- Minimally displaced.
- Low demand patient.
- Fragment does not block motion.
- Sling immobilization for 4-6 weeks.
- Passive external rotation restricted (protect subscap) usually to neutral.
- Active internal rotation avoided for 6 weeks.
- Elbow/wrist/hand ROM immediately.
- Progressive strengthening after 6-8 weeks.
Close radiographic follow-up is required to ensure no late displacement.
BLOCKManagement Indications
Hook:Remember BLOCK when deciding to operate on a lesser tuberosity fracture.
Surgical Technique
Fixation Techniques
Deltopectoral Approach:
- Standard approach for lesser tuberosity.
- Position: Beach chair.
- Incision: Coracoid to axillary fold.
- Plane: Pectoralis major (medial) and Deltoid (lateral).
- Cephalic vein: Retract laterally with deltoid.
- Expose clavipectoral fascia, identify conjoined tendon.
Adequate exposure is critical for anatomical reduction.
The McLaughlin Procedure (Lesser Tuberosity Transfer)
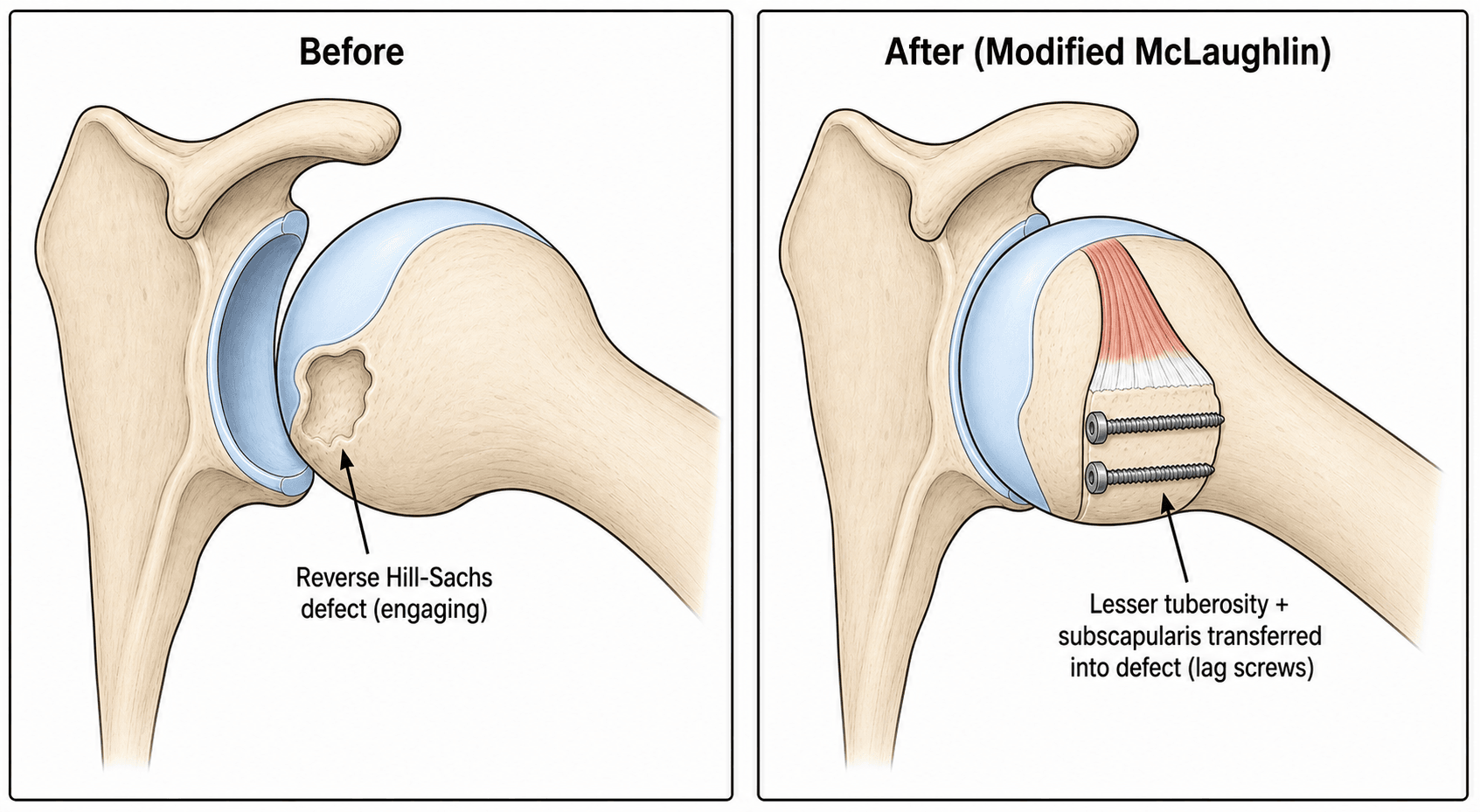
The topic invokes "McLaughlin", "modified McLaughlin" and the Xiong card four times - the lesser tuberosity is its workhorse - but the procedure itself is never described. It is the answer when a locked posterior dislocation has an engaging anteromedial impaction (reverse Hill-Sachs) defect that must be filled so the head stops catching on the glenoid.
- Original McLaughlin (1952): transfer the subscapularis tendon into the reverse Hill-Sachs defect, so soft tissue fills and blocks the engaging notch.
- Modified McLaughlin (Neer): transfer the lesser tuberosity together with its attached subscapularis into the defect - a bone-block that fills the notch more durably and heals bone-to-bone. This is why a lesser tuberosity topic owns the procedure.
deltopectoral approach → reduce the dislocation → osteotomise/elevate the lesser tuberosity with the subscapularis → transpose it into the reverse Hill-Sachs defect and fix with lag screws (and sutures), with or without bone graft (Xiong used a partial lesser tuberosity plus artificial bone secured with two lag screws and Ethibond).
Where it sits in the defect-size ladder (the broader reverse Hill-Sachs decision is developed in reverse-hill-sachs-lesions):
- Strategy
- Closed reduction +/- disimpaction; often stable
- Strategy
- McLaughlin / modified McLaughlin (lesser tuberosity transfer)
- Strategy
- Rotational osteotomy, osteoarticular allograft, or arthroplasty
Outcomes are good for the moderate defect: Xiong's modified McLaughlin improved the Constant-Murley score from 46 to 86 with no recurrent instability.
For a locked posterior dislocation with a ~25-40% engaging reverse Hill-Sachs defect, the McLaughlin procedure fills it: the original transfers the subscapularis tendon, the modified (Neer) transfers the lesser tuberosity + subscapularis as a bone block (lag-screw fixed). Smaller defects are reduced/disimpacted; larger ones (over ~40-50%) need rotational osteotomy or arthroplasty.
The Long Head of Biceps in Lesser Tuberosity Fractures
The biceps is flagged repeatedly - "incarceration blocks reduction", "at risk during fixation", "tenosynovitis/rupture" - but what to do about it is never stated, and it is a recurring viva point.
Why the biceps is involved. The long head of biceps (LHB) runs in the bicipital groove immediately lateral to the lesser tuberosity, roofed by the transverse humeral ligament that bridges the lesser to the greater tuberosity. A lesser tuberosity fracture therefore threatens the LHB in three distinct ways:
- Mechanism
- The LHB or a fragment becomes trapped in the fracture, blocking reduction
- Management
- Identify and FREE the tendon from the fracture before reducing; the block will not reduce until it is extracted
- Mechanism
- Loss of the medial groove wall / transverse ligament lets the LHB sublux medially out of the groove
- Management
- If the tendon is unstable, tenotomy or tenodesis rather than leaving it to subluxate and cause pain
- Mechanism
- Screws or anchors placed too laterally enter the groove and abrade or transfix the tendon
- Management
- Keep ALL hardware medial to / out of the bicipital groove; orient off the LHB as a landmark
The decision. When the LHB is damaged, unstable, or an obvious pain generator at the time of lesser tuberosity fixation, deal with it definitively rather than ignoring it - tenodesis in the younger/higher-demand patient (preserves contour and avoids cramping), tenotomy in the older/lower-demand patient. (General LHB pathology, SLAP and tenodesis technique are developed in proximal-biceps-ruptures.)
The LHB sits just lateral to the lesser tuberosity in the groove, so a lesser tuberosity fracture can incarcerate it (free it before you can reduce), destabilise it medially (tenotomy/tenodese if unstable), or be injured by lateral hardware (keep screws out of the groove). Always identify the biceps - it is both the orientation landmark and the structure most at risk.
Complications
Potential Complications
Weakness/Insufficiency: Failure of healing or non-union leads to weak internal rotation and anterior instability. Positive lift-off/belly press tests. This is the most common reason for revision if non-op fails.
Ten.donitis/Subluxation: The biceps tendon runs adjacent to the fracture. Callus formation or hardware can cause tenosynovitis or rupture. Incarceration blocks reduction.
Recurrent Dislocation: If the lesser tuberosity (anterior stabilizer) fails to heal, the humeral head may subluxate posteriorly.
Mechanical Block: Medial malunion is tolerated well, but prominent anterior malunion can block internal rotation or impinge on coracoid. This requires excision.
Postoperative Care
Rehabilitation Protocol
- Sling immobilization.
- No active internal rotation.
- Passive external rotation limited (usually to 0 degrees or neutral).
- Elbow/wrist/hand ROM.
- Pendulum exercises started early.
- Wean from sling.
- Progressive passive ROM.
- Gentle active-assisted Grade 1-2.
- Avoid forceful ER (puts tension on subscapularis repair).
- Forward elevation active-assisted.
- Active ROM allowed.
- Isometrics to Isotonics.
- Internal rotation strengthening initiated.
- Scapular stabilization focus.
- Hydrotherapy can be useful.
- Return to sport/heavy labor.
- Full ROM goal.
- Maintenance of cuff strength.
- Return to contact sports only when strength is 90% of contralateral side.
Outcomes
Prognosis
- Union Rates: High, generally excellent healing potential due to cancellous bed. Non-union is rare but symptomatic.
- Function: Good to excellent in 85-90% of surgically treated cases.
- Missed Diagnosis: Leads to chronic pain and weakness. Chronic posterior dislocation has poor prognosis if missed greater than 3 weeks (often requires arthroplasty).
- Subscapularis Strength: Often recovers to near normal, but some residual weakness in lift-off is common even with successful repair.
Guidelines, Registries & Global Practice
Global Epidemiology
- Isolated lesser tuberosity fracture is rare — under 0.5% of all fractures and a small minority of proximal humeral fractures (Court-Brown 2001, N=1027 prospective series).
- Two distinct populations: adolescent males with an apophyseal avulsion during sport (abduction-extension mechanism), and adults sustaining avulsion during a posterior dislocation from seizure, electric shock, or trauma.
- Posterior glenohumeral dislocation itself accounts for only 2-4% of all shoulder dislocations and is missed at first presentation in roughly half of cases.
Side-by-Side Guidance
- Region
- Global
- Emphasis
- Anatomical reduction of the subscapularis footprint; screw or suture-anchor fixation; protect the long head of biceps
- Region
- US
- Emphasis
- Most proximal humeral fractures non-operative; shared decision-making and early supervised motion
- Region
- UK
- Emphasis
- Senior review of fracture-dislocations; CT for surgical planning; urgent reduction of locked dislocations
- Region
- Europe
- Emphasis
- Recognise posterior dislocation early; reverse Hill-Sachs size drives reconstruction strategy
No society publishes a lesser-tuberosity-specific guideline; recommendations are extrapolated from proximal humerus and posterior instability guidance. The widely cited 5 mm displacement threshold is expert-consensus, not guideline-mandated.
Registry Note
- Proximal humerus registries (e.g. national arthroplasty registries) capture this injury only when it progresses to arthroplasty for a chronic locked fracture-dislocation; isolated tuberosity fixation is not separately tracked, so the evidence base remains case series rather than registry data.
High- vs Limited-Resource Practice
- Well-resourced settings: Cross-sectional CT for fragment sizing, MRI for tendon integrity, arthroscopic-assisted or open anchor repair.
- Limited-resource settings: Diagnosis rests on a good axillary radiograph and clinical subscapularis testing; transosseous suture repair through drill holes substitutes for anchors, with comparable healing in cancellous bone.
- Universal priority: Early reduction of any associated locked posterior dislocation — delay beyond 3 weeks markedly worsens the outcome regardless of setting.
Controversies and Areas of Uncertainty
Where the Evidence Is Thin
The 5 mm operative threshold is expert consensus extrapolated from small series, not a validated cut-off. Some advocate fixation at 3 mm in overhead athletes; others tolerate larger displacement in low-demand patients.
No comparative trial exists. Large bony fragments favour lag screws; small, comminuted, or apophyseal fragments favour an anchor lasso. Choice remains surgeon preference guided by fragment size and bone quality.
Arthroscopic-assisted repair is increasingly described but evidence is limited to case series; open deltopectoral fixation remains the reference standard, especially when a posterior dislocation must also be addressed.
Defect-size thresholds guiding McLaughlin transfer (roughly 25-40%) versus rotational osteotomy or arthroplasty (greater than 40-50%) are derived from small cohorts and vary between authors.
MCQ Practice
Self-Assessment Questions
Q: Which muscle attaches to the lesser tuberosity of the humerus?
- A) Supraspinatus
- B) Infraspinatus
- C) Teres Minor
- D) Subscapularis
- E) Pectoralis Major
A: D - The subscapularis is the only rotator cuff muscle that attaches to the lesser tuberosity. Supraspinatus, Infraspinatus, and Teres Minor attach to the Greater Tuberosity. Pectoralis Major attaches to the lateral lip of the bicipital groove.
Q: An isolated lesser tuberosity fracture following a seizure should raise highest suspicion for:
- A) Anterior dislocation
- B) Posterior dislocation
- C) Axillary nerve injury
- D) Biceps rupture
- E) Rotator cuff tear
A: B - Seizures cause violent muscle contractions leading to posterior dislocation. The lesser tuberosity fracture is often an avulsion injury associated with this mechanism.
Q: What is the most sensitive radiographic view for diagnosing a lesser tuberosity fracture profile?
- A) AP Internal Rotation
- B) AP External Rotation
- C) Scapular Y
- D) Axillary Lateral
- E) Outlet View
A: D - The Axillary Lateral view projects the lesser tuberosity anteriorly, allowing assessment of its profile and displacement. It is also diagnostic for posterior dislocation.
Q: What is the generally accepted displacement threshold for surgical fixation of lesser tuberosity fractures in active patients?
- A) 1mm
- B) 3mm
- C) 5mm
- D) 10mm
- E) Any displacement requires surgery
A: C - 5mm is the commonly cited threshold (Ogawa et al.) where surgical fixation is recommended to restore subscapularis function and prevent mechanical block.
Q: Which surgical approach is most appropriate for open reduction internal fixation of a lesser tuberosity fracture?
- A) Deltoid Splitting
- B) Deltopectoral
- C) Posterior
- D) Mackenzie
- E) Trans-acromial
A: B - The Deltopectoral approach utilizes the interval between the deltoid and pectoralis major to provide direct anterior access to the lesser tuberosity and subscapularis.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 40-year-old male presents with shoulder pain after a seizure. X-rays show a lesser tuberosity fracture. What is your immediate concern and how do you investigate it?”
“What are the surgical indications for a lesser tuberosity fracture?”
“Describe the Deltopectoral Approach for fixing a lesser tuberosity fracture.”
Key Facts
- Attachment: Subscapularis
- Threshold: 5mm displacement
- Assoc: Posterior Dislocation (Seizures)
- Nerve at risk: Axillary (inf), Musculocutaneous (medial retraction)
- Structure at risk: Biceps Tendon (lateral)
Surgical Steps
- Deltopectoral Approach
- Identify LHB and LT
- Reduce fragment (medial to lateral)
- Screw fixation (large) or Suture Anchor (small)
- Protect Biceps
Common Pitfalls
- Missing posterior dislocation
- Missing associated reverse Hill-Sachs
- Hardware in bicipital groove
- Failure to recognize subscapularis weakness
Examiner Favorites
- What muscle attaches here?
- Mechanism of injury?
- How do you test clinical function? (Lift-off)
- Surgical approach anatomy?
Evidence Base
Key Studies
Ogawa & Takahashi - Long-Term Outcome of Isolated Lesser Tuberosity Fractures
- Series of 10 isolated lesser tuberosity fractures (6 acute, 4 chronic), mean age 30 years
- ORIF most often recommended for displaced acute injuries; all 3 operated acute cases excellent/satisfactory
- In chronic cases conservative (muscle strengthening) is first line, with ORIF reserved for failures
Garrigues et al. - Subscapularis Avulsion of the Lesser Tuberosity in Adolescents
- 6 skeletally immature patients plus pooled literature review; mean follow-up over 4 years
- Prototype: 13-year-old male, abduction-extension sporting injury, positive belly-press and lift-off
- Suture-anchor lasso technique gave predictably good results (mean ASES 97, WOSI 94)
Levine et al. - Avulsion Fractures of the Lesser Tuberosity in Adolescents
- Case report plus literature review of lesser tuberosity apophyseal avulsion in adolescents
- Often present late as chronic shoulder pain after a missed acute diagnosis
- ORIF of the displaced apophyseal fragment restored full motion and strength at 4 months
Gerber & Krushell - Isolated Rupture of the Subscapularis Tendon
- 16 men with isolated subscapularis rupture from forced hyperextension or external rotation of the adducted arm
- Loss of internal-rotation strength and increased passive external rotation without instability
- Introduced and validated the lift-off test for clinically relevant subscapularis lesions
Xiong et al. - Modified McLaughlin for Locked Chronic Posterior Dislocation
- 5 locked chronic posterior dislocations with reverse Hill-Sachs defects of 30-40% of the head
- Lesser tuberosity plus artificial bone transferred into the defect, fixed with two lag screws and sutures
- Constant-Murley score improved from 46.0 to 85.8 with no recurrent instability at mean 19.8 months
Court-Brown et al. - Epidemiology of Proximal Humeral Fractures
- Prospective 5-year study of 1,027 proximal humeral fractures
- Unimodal age distribution peaking in women aged 80-89 years
- AO classification more comprehensive than Neer; isolated tuberosity patterns are uncommon