Distraction Osteogenesis | Ilizarov Technique | Regenerate Formation
- Distraction rate: 1mm/day in 4 divided doses (0.25mm QID)
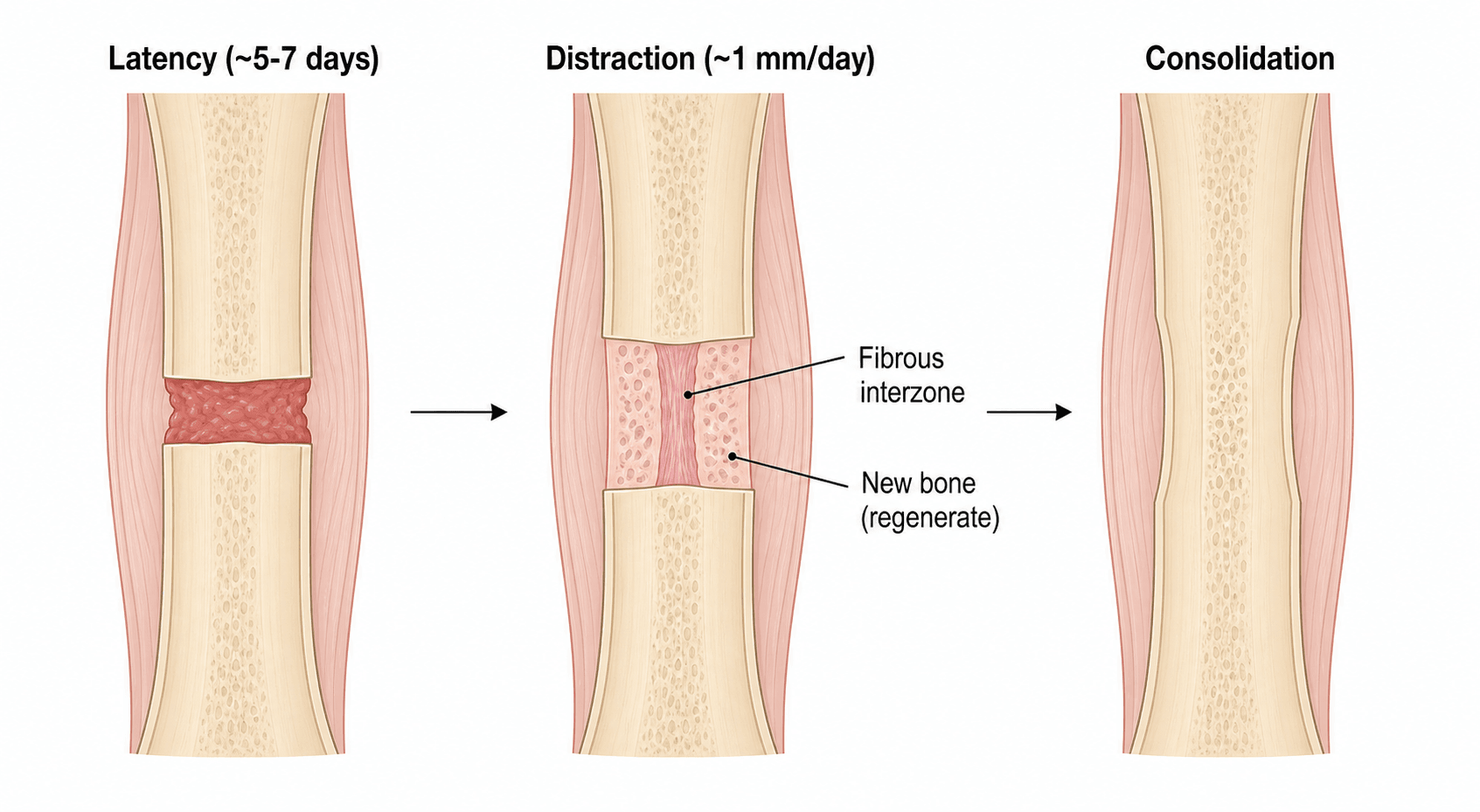
- Latency period: 5-7 days (longer in adults, smokers)
- Consolidation: Approximately 1 month per cm of lengthening
- Maximum safe lengthening: Generally 20% of original bone length
- Corticotomy vs osteotomy: Corticotomy preserves periosteum and medullary blood supply
- “Ilizarov discovered distraction osteogenesis principles in Kurgan, Russia
- “Faster distraction causes fibrous tissue; slower causes premature consolidation
- “Healing index = days in frame / cm lengthened (normal 30-45 days/cm)
- “Regenerate problems: Too fast = cyst/fibrous; Too slow = premature consolidation
1mm per day is the standard rate, divided into 4 increments of 0.25mm (QID rhythm). Faster distraction causes fibrous regenerate or cyst formation. Slower distraction causes premature consolidation. Adjust based on regenerate quality on X-ray.
5-7 days in children, 7-14 days in adults. This allows initial callus formation before distraction begins. Shorter latency risks poor regenerate; longer risks premature consolidation. Smokers and diabetics need longer latency.
Corticotomy (not osteotomy) preserves periosteum, medullary blood supply, and marrow contents. Low-energy technique with multiple drill holes and osteotome completion. Minimally invasive approach preferred to preserve biology.
Soft tissues limit lengthening - muscles, nerves, vessels all resist distraction. Physiotherapy essential throughout. Monitor for joint contractures, nerve symptoms. Maximum safe lengthening is 20% of original length per session.
Overview and Epidemiology
Limb lengthening utilizes the biological principle of distraction osteogenesis to generate new bone within a gradually widening gap created by controlled separation of bone ends. First described by Codivilla in 1905 and refined by Ilizarov in the 1950s, it has revolutionized treatment of limb length discrepancy and short stature conditions.
- Congenital: Fibular hemimelia, congenital femoral deficiency, hemihypertrophy
- Developmental: Achondroplasia, hypochondroplasia, other skeletal dysplasias
- Acquired: Post-traumatic, post-infection, post-tumour resection
- Limb length discrepancy: Greater than 2.5cm predicted at maturity
- Active infection
- Poor soft tissue envelope
- Inadequate bone stock
- Poor patient compliance
- Uncontrolled vascular disease
- Severe psychological issues
Gavriil Ilizarov developed the principles of distraction osteogenesis while treating World War II veterans in Kurgan, Siberia. His work remained unknown in the West until the 1980s when Italian surgeons visited his institute. The "tension-stress effect" describes how gradual traction stimulates tissue regeneration.
Pathophysiology
Understanding the biology of distraction osteogenesis is fundamental to successful limb lengthening.
The Tension-Stress Effect
Ilizarov's principle:
- Gradual traction on living tissues creates stress that stimulates regeneration
- Applies to bone, soft tissues, blood vessels, nerves, skin
- Optimal tension maintains cellular viability while stimulating proliferation
- Too much tension = ischemia and tissue death
- Too little tension = insufficient stimulation
Biology of Bone Regeneration
- Fibrous interzone: Central region of collagen fibers aligned parallel to distraction
- Primary mineralization front: Active osteoid formation at bone ends
- Microcolumn formation: Longitudinal columns of bone forming
- Remodeling zone: Mature lamellar bone formation
- Periosteal and endosteal osteoprogenitor cells activated
- Angiogenesis critical for regenerate formation
- Mechanical strain drives mesenchymal stem cell differentiation
- Growth factors (BMP, VEGF, TGF-beta) upregulated
Optimal Conditions for Regenerate
- Low-energy technique preserving periosteum
- Multiple drill holes followed by osteotome completion
- Minimally invasive approach preferred
- Avoid saw (thermal necrosis) or Gigli wire (periosteal stripping)
- 1mm/day is optimal for most situations
- Divided into 4 increments (0.25mm QID) better than single daily adjustment
- Continuous distraction (motorized devices) may be superior
- Adjust based on regenerate appearance
Regenerate quality guides rate adjustment. Cystic/poor regenerate = slow down to 0.5-0.75mm/day. Premature consolidation = speed up to 1.5mm/day or perform regenerate "accordioning" (compress then re-distract). Always assess regenerate on orthogonal X-rays.
Classification Systems
Several classifications are high-yield in the lengthening viva. None is a single "staging" system - they describe the biology phases, the complication severity, and the outcome benchmark.
- Latency - corticotomy to start of distraction (5-7 days children, 7-14 days adults); initial callus forms.
- Distraction - active lengthening at 1 mm/day (0.25 mm QID) until target length.
- Consolidation - regenerate mineralises (~1 month/cm) while the frame neutralises load.
- Remodelling - cortical maturation continues after frame/nail removal.
Clinical Presentation
Patient Assessment
- Aetiology of limb length discrepancy
- Functional limitations and goals
- Previous surgery
- Medical comorbidities (diabetes, smoking - affect healing)
- Psychological readiness for prolonged treatment
- Accurate limb length measurement (blocks, CT scanogram)
- Joint range of motion
- Muscle strength and soft tissue quality
- Neurovascular status
- Skin condition and previous scars
Limb Length Discrepancy Measurement
- Block method with standing
- Tape measure (ASIS to medial malleolus)
- Galeazzi test for femoral vs tibial discrepancy
- CT scanogram: Gold standard, accurate to 1mm
- Standing long-leg radiograph: Also shows alignment
- EOS imaging: Low radiation, full-length imaging
Prediction of Discrepancy at Maturity
- Moseley straight-line graph
- Multiplier method (Paley)
- Anderson-Green growth remaining charts
- Less than 2cm: Shoe lift, observe
- 2-5cm: Epiphysiodesis or lengthening
- Greater than 5cm: Lengthening (possibly staged)
Investigations
Preoperative Imaging
- Accurate measurement of bone lengths
- Assessment of bone quality
- Deformity analysis
- Mechanical axis assessment
- Joint orientation angles
- Planning for concurrent deformity correction
- Soft tissue assessment
- Physeal mapping if epiphysiodesis considered
- Intramedullary canal assessment for nail
Vascular Assessment
Indications for angiography:
- Previous vascular injury
- Absent pulses
- Congenital limb deficiency (vessel anomalies common)
- Large lengthening planned (greater than 5cm)
Psychological Assessment
Important in:
- Cosmetic lengthening (achondroplasia)
- Adolescent patients
- Multiple previous surgeries
- Complex family dynamics
Assessing the Regenerate (image interpretation)
Reading the distraction-gap regenerate on serial orthogonal radiographs is a core ISAWE/viva skill - you must be able to look at a film and say whether the regenerate is healthy and what you would do.
- Homogeneous, increasing radiodensity filling the gap, continuous with both bone ends.
- The classic "three-column" pattern - two denser peripheral columns and a central lucent growth zone that mineralises last.
- Width of the regenerate roughly matches the parent bone (good cross-sectional area).
- Lucent / thin / "candle-flame" attenuation in mid-gap = distraction too fast for biology - slow the rate (0.5-0.75 mm/day).
- Cystic lucency = poor osteogenesis - slow down, check patient factors (smoking, vitamin D, nutrition), consider the accordion manoeuvre or bone grafting.
- Premature mineralisation bridging the gap early = rate too slow / latency too long - speed up (or re-corticotomy if consolidated).
- Asymmetric / angulated regenerate = axial deviation - adjust the frame/struts.
Regenerate shape (described on the AP film) ranges from the favourable fusiform/cylindrical column to the unfavourable concave ("waisted"), lateral, or central (hourglass) patterns, which flag inadequate cross-sectional bone and a higher risk of regenerate fracture after frame removal.
Don't just describe it - state the action. Thin/cystic = slow distraction and optimise biology; persistent poor regenerate = accordion or graft; symmetric premature consolidation = increase rate. Always confirm on orthogonal views before acting, and never remove the frame until 3 of 4 cortices are bridged.



Deformity Analysis: CORA, Joint Angles and the Osteotomy Rules
Lengthening frames also correct deformity, and the examiner expects the analytic framework behind that - the mechanical axis, the joint orientation angles, the CORA and Paley's osteotomy rules.
Mechanical axis and the malalignment test
- The mechanical axis of the leg runs from the centre of the femoral head to the centre of the ankle; normally it passes just medial to the knee centre.
- Mechanical axis deviation (MAD) is the perpendicular distance from that line to the knee centre - normal is about 8 to 10 mm medial (roughly 8 plus or minus 7 mm). An abnormal MAD is the malalignment test that tells you a deformity exists; the joint orientation angles then localise it.
Joint orientation angles (where is the deformity?)
- Joint
- Mechanical lateral distal femoral angle
- Approximate normal
- About 85 to 90 degrees
- Joint
- Medial proximal tibial angle
- Approximate normal
- About 85 to 90 degrees
- Joint
- Lateral distal tibial angle
- Approximate normal
- About 86 to 92 degrees
- Joint
- Joint-line convergence angle
- Approximate normal
- About 0 to 2 degrees
An abnormal angle pinpoints whether the deformity is femoral or tibial and on which side, which determines where to cut.
CORA and Paley's osteotomy rules
- The CORA (centre of rotation of angulation) is the point where the proximal and distal axis lines intersect - the true apex of the deformity.
- Osteotomy rule 1: if the osteotomy and the angulation-correction axis both pass through the CORA, you get pure angular correction with no translation.
- Osteotomy rules 2 and 3: if the osteotomy is made away from the CORA, correcting the angle introduces a secondary translation (a "Z" deformity) - acceptable only when deliberately planned. The practical message is to find the CORA and base the correction there.
Before correcting any deformity, run the malalignment test (MAD), use the joint orientation angles (mLDFA / MPTA roughly 85 to 90 degrees) to localise it, and find the CORA. Osteotomise and angulate at the CORA for pure angular correction; cutting away from it introduces translation. A hexapod frame (TSF) executes this in six axes simultaneously.
Differential of LLD Management Strategies
A common viva trap is to jump straight to lengthening. The first decision is whether to lengthen the short side, shorten the long side, or accept and accommodate the discrepancy. The projected discrepancy at maturity, skeletal age, and patient goals drive the choice.
- Best suited to
- Under 2 cm projected
- Key advantage
- Non-operative, immediate
- Main limitation
- Cosmesis, ceiling near 2 cm
- Best suited to
- 2-5 cm, growth remaining
- Key advantage
- Single small operation, low morbidity
- Main limitation
- Sacrifices height; timing-dependent
- Best suited to
- Skeletally mature, small discrepancy
- Key advantage
- One stage, no frame
- Main limitation
- Loses height; limited to ~2-3 cm safely
- Best suited to
- Greater than 5 cm or deformity
- Key advantage
- Multiplanar correction, bone transport
- Main limitation
- Pin-site care, frame time, contractures
- Best suited to
- Isolated LLD, good bone/canal
- Key advantage
- No external device, no pin sites
- Main limitation
- Cost, minimal deformity correction
Management
Corticotomy Technique
- Low-energy technique to preserve biology
- Metaphyseal location preferred (better blood supply)
- Minimally invasive approach
- Small incision at planned osteotomy site
- Apply external fixator or prepare for nail
- Multiple drill holes circumferentially through cortex
- Complete osteotomy with osteotome
- Confirm mobility of bone ends
- Wound closure
- Ilizarov: Rings with tensioned wires and half-pins
- TSF: Hexapod system with struts for multiplanar correction
- Monolateral: Rail fixator, simpler but less versatile
- Corticotomy as above
- Ream canal
- Insert lengthening nail (PRECICE or similar)
- Lock proximally and distally
- Confirm device activation
This section covers surgical technique.
Surgical Management
Device Selection
External Fixation Devices
- Classic ring fixator with tensioned wires
- Excellent stability
- Allows weight-bearing
- Complex application, steep learning curve
- Hexapod based on Stewart platform
- Computer-assisted deformity correction
- Six-axis control simultaneously
- Web-based planning software
- Rail-based systems
- Simpler application
- Less versatile for deformity correction
- May have higher complication rates
- Can correct deformity simultaneously
- Lower implant cost
- Can adjust postoperatively
- Suitable for complex cases
- Pin site care burden
- Pin site infections common
- Patient discomfort
- Cosmetically unacceptable to some
This section covers external fixation options.
Complications
Bone Complications
- Premature consolidation: Rate too slow, requires re-osteotomy
- Delayed consolidation: Rate too fast, bone grafting may be needed
- Regenerate fracture: After frame removal, protect with cast/brace
- Axial deviation: Angulation during lengthening, adjust fixator
Soft Tissue Complications
- Joint contracture: Most common, aggressive physiotherapy essential
- Joint subluxation/dislocation: Over-lengthening, reduce length
- Nerve injury: Stretch neuropathy, slow or stop distraction
- Vascular compromise: Rare, urgent assessment needed
Pin Site Complications
- Pin site infection: Most common overall (30-100% incidence)
- Pin tract osteomyelitis: Rare but serious
- Pin loosening: May require replacement
Device Complications
- Frame instability: Construct failure, revision
- Nail mechanical failure: Device malfunction, exchange
Joint contractures are the most significant functional complication. Aggressive physiotherapy from day one is essential. Consider prophylactic soft tissue releases (Achilles lengthening, knee capsulotomy) for large lengthenings. Monitor joint ROM at every visit.
Pin-Site Infection: Checketts-Otterburn Grading
Pin-site infection is the commonest complication of external fixation, and the examiner wants a graded, structured answer rather than just "give antibiotics." The Checketts-Otterburn classification separates minor (soft-tissue) from major (bone-involving) infection and drives management.
- Features
- Slight redness, slight discharge
- Management
- Improve pin-site care
- Features
- Redness, discharge, soft-tissue pain and tenderness
- Management
- Pin care plus oral antibiotics
- Features
- Grade 2 not responding to antibiotics
- Management
- Remove or exchange the affected pin/wire
- Features
- Severe soft-tissue infection of several pins, sometimes with pin loosening
- Management
- Remove affected pins, reassess the construct, antibiotics
- Features
- Grade 4 plus radiographic bone involvement
- Management
- Pin removal, debridement, treat as osteomyelitis
- Features
- Occurs after frame removal - the pin track discharges and forms a ring sequestrum
- Management
- Curettage of the pin track / sequestrum
The split is the key point: grades 1 to 3 are minor and soft-tissue (pin care and antibiotics, escalating to pin removal); grades 4 to 6 are major and involve bone (pin removal, debridement, treat as deep infection). Most pin-site infections are Paley "problems" that settle without theatre - but a ring sequestrum after removal is a recognised, treatable cause of persistent discharge.
Don't just say "antibiotics" - grade it. Checketts-Otterburn 1 to 3 (minor, soft-tissue) = pin care and oral antibiotics, removing the pin if it fails; 4 to 6 (major, bone) = pin removal, debridement and treat as osteomyelitis, with grade 6 (a ring sequestrum after frame removal) needing curettage.
Structures at Risk & Safe Technique
The distraction-osteogenesis biology applies to nerves and vessels too - but they tolerate stretch less well than bone, so the soft tissues, not the bone, set the safe limit. Know the structure most at risk for each segment and how to protect it.
- Structure most at risk
- Common peroneal nerve (foot-drop), then tibial nerve; anterior tibial vessels
- Protective strategy
- Consider prophylactic peroneal nerve decompression at the fibular neck for large gains; ankle splint against equinus; slow rate if dorsiflexion weakens
- Structure most at risk
- Sciatic nerve stretch; quadriceps (knee flexion contracture, patellar subluxation)
- Protective strategy
- Knee ROM/extensor physio from day one; watch for patellar tracking; consider quadricepsplasty for refractory contracture
- Structure most at risk
- Radial nerve
- Protective strategy
- Identify/protect at corticotomy; monitor wrist/finger extension during distraction
- Structure most at risk
- Vascular compromise (rare) / compartment syndrome
- Protective strategy
- Urgent assessment; never ignore disproportionate pain or a tense compartment
Safe corticotomy / technique points:
- Metaphyseal corticotomy (richer vascularity, broader cross-section) regenerates better than diaphyseal.
- Low-energy technique - drill holes + osteotome, protect periosteum; avoid the power saw (thermal necrosis) and Gigli-wire circumferential stripping.
- Pre-tension wires and place half-pins in safe corridors away from neurovascular bundles (use the standard Ilizarov tibial safe zones).
- Nerve symptoms during distraction (paraesthesia, weakness) → slow or pause distraction first; if they persist, decompress. A new foot-drop is an emergency, not a "problem."
Bone Transport & Segmental Defects
Distraction osteogenesis is not only for lengthening - the same biology reconstructs segmental bone loss (infected non-union, tumour resection, open-fracture bone loss) by bone transport: a corticotomy creates a mobile transport segment that is gradually moved across the defect on the frame, laying down regenerate behind it while it advances, until it meets (docks) the far fragment.
- Monofocal - simple lengthening/compression at one corticotomy (no defect).
- Bifocal - one corticotomy + transport across a single defect (the standard bone-transport construct); regenerate forms at the corticotomy, the docking site is where the transport segment meets the far fragment.
- Trifocal - two corticotomies / two transport segments for very large defects (faster, halves transport distance, but two regenerate sites).
- Transport rate mirrors lengthening - ~1 mm/day in divided steps; the transported segment is moved, not the limb lengthened, so overall length is preserved.
- Acute shortening-then-relengthening is an alternative for some defects (closes the gap acutely, lengthens elsewhere).
Postoperative Care
Limb lengthening is unusual in that the postoperative phase is the treatment - the operation only sets it up. Structured aftercare determines the result.
- Pin/wire-site care: daily cleaning to an agreed protocol; teach the patient/family to recognise infection (erythema, discharge, pain) and to treat early with oral antibiotics. Most pin-site infections are "problems" that settle without surgery.
- Distraction management: begin after the latency period; 0.25 mm QID; provide a written turning schedule and a turning diary. Review the regenerate on orthogonal radiographs (initially fortnightly).
- Physiotherapy from day one: daily active and passive range of motion to counter the dominant functional complication - joint contracture. Splinting/orthoses to hold the ankle/knee in a functional position; foot-drop and equinus prophylaxis during tibial lengthening.
- Weight-bearing: partial-to-full weight-bearing is encouraged with circular frames (they are axially dynamic), which stimulates regenerate; protected weight-bearing with internal nails per device limits.
- Monitoring during consolidation: radiographs every 2-4 weeks; watch for axial deviation, regenerate quality and neurovascular symptoms.
- Frame/device removal: when 3 of 4 cortices are consolidated on orthogonal films; protect the limb (cast/brace, activity restriction) afterwards to prevent regenerate fracture. Dynamise frames before removal to confirm the regenerate can bear load.
Outcomes/Prognosis
- Healing index is the universal outcome measure: 30-45 days/cm is a normal external-fixator course; magnetic intramedullary nail series report indices around 30 days/cm without pin-site morbidity.
- Achieving target length is reliable in experienced units - large internal-nail and frame cohorts reach within ~2.5 cm of goal in the high-80s-to-90s percent of cases.
- The complication burden is high and expected: most segments have at least one Paley problem/obstacle/complication, and this rises steeply beyond ~20% (and especially beyond ~55%) of segment length - the rationale for staging large lengthenings.
- Functional outcome is generally good when joint motion is preserved; the strongest determinant of a poor result is an uncorrected joint contracture or subluxation rather than the bone itself.
- Prognostic factors: younger age, good bone quality, smaller percentage lengthening, non-smoking status, metaphyseal corticotomy and reliable physiotherapy all favour a lower healing index and fewer complications.
Guidelines, Registries & Global Practice
Limb lengthening is a low-volume, high-complexity procedure concentrated in specialist limb-reconstruction units worldwide. There is no single randomised guideline; practice is built on the Ilizarov biological principles, the Paley classification of complications, and accumulating registry and cohort data on internal versus external devices.
Global Epidemiology
- Limb length discrepancy (LLD) is common: minor discrepancies (under 1 cm) occur in a large proportion of the population and are usually asymptomatic. Discrepancies projected to exceed 2-2.5 cm at maturity are the usual threshold for active management.
- Aetiology varies by region: congenital deficiency (fibular hemimelia, congenital femoral deficiency) and post-infective/post-physeal-arrest causes dominate paediatric practice; post-traumatic shortening and bone-defect reconstruction dominate adult practice. Post-infective growth arrest is proportionally more common in limited-resource settings.
- Cosmetic (stature) lengthening is a growing but ethically scrutinised indication, performed mainly in dedicated private centres.
Side-by-Side Society Positions
- Emphasis
- Distraction-osteogenesis biology, frame technique
- Practical recommendation
- 1 mm/day in 4 steps; low-energy corticotomy; report by Paley classification
- Emphasis
- Centralisation of paediatric reconstruction
- Practical recommendation
- Manage in specialist multidisciplinary units; MDT with physiotherapy and psychology
- Emphasis
- Device selection, internal nails
- Practical recommendation
- Magnetic intramedullary nails for isolated lengthening with good bone/canal; frames for deformity
- Emphasis
- Patient selection, complication reporting
- Practical recommendation
- Standardised outcome reporting (healing index, Paley grade); caution on cosmetic indications
There is broad consensus on the core protocol (latency, 1 mm/day rate, divided rhythm, healing index as outcome) and on managing patients in MDT units. The main divergence is device preference: increasing use of magnetic intramedullary nails (PRECICE/Fitbone) for isolated lengthening in high-resource settings, versus continued reliance on Ilizarov/hexapod frames where implant cost or deformity correction dominates.
Registry and Cohort Notes
- Unlike arthroplasty, there is no large national lengthening registry; evidence comes from high-volume single-centre and multicentre cohorts (e.g. Calder et al., Royal National Orthopaedic Hospital; Rozbruch/Fragomen, Hospital for Special Surgery).
- Magnetic-nail series consistently report healing indices around 30 days/cm with elimination of pin-site infection, at the cost of higher implant price and limited deformity correction.
- A voluntary withdrawal of the titanium PRECICE nail (2020-2021) over retrieval/biocompatibility concerns is an important exam-relevant safety event illustrating implant surveillance in this field.
High- vs Limited-Resource Practice
- High-resource centres: ready access to magnetic internal nails, hexapod frames with software planning, EOS imaging and intensive physiotherapy/psychology support.
- Limited-resource centres: Ilizarov circular frames remain the workhorse - durable, reusable, low implant cost, and capable of simultaneous lengthening, deformity correction and bone transport for infected non-unions. Pin-site care education and physiotherapy access are the main limiting factors.
Controversies & Areas of Uncertainty
- Internal nail vs external fixator: Magnetic nails reduce pin-site morbidity and improve patient acceptance, but implant cost, weight-bearing limits during distraction and inability to correct significant deformity keep frames relevant. The titanium PRECICE withdrawal over retrieval concerns underlines that long-term implant data are still maturing.
- Cosmetic stature lengthening: Bilateral lengthening for short stature (including achondroplasia and constitutional short stature) remains ethically contested. The complication burden of large bilateral lengthenings must be weighed against a non-medical indication; rigorous psychological assessment is mandatory.
- The "20% limit": Historically lengthening was capped near 20% of segment length. Modern series show greater gains are achievable but with a near-universal problem/obstacle/complication burden, especially beyond 55% - favouring staged lengthening over a single large session.
- Optimal rhythm: Animal data favour higher distraction frequency; fully continuous (automated) distraction may produce better regenerate than QID, but most clinical practice remains 0.25 mm four times daily for practicality.
- Adjuncts to regenerate healing: BMP, PRP, bisphosphonates and low-intensity pulsed ultrasound have all been trialled to accelerate consolidation, but none is established as standard of care.
MCQ Practice Points
A: 1 mm/day, given as 0.25 mm four times daily (QID). Distraction that is too fast produces a fibrous or cystic regenerate; too slow leads to premature consolidation. More frequent, smaller steps give a better regenerate than a single daily turn.
A: A corticotomy is a low-energy cut that preserves the periosteum, endosteum and medullary (marrow) blood supply, all of which are essential for regenerate formation. Avoid the power saw (thermal necrosis) and circumferential periosteal stripping. Metaphyseal locations heal best because of their rich vascularity.
A: The healing index is the number of days in the frame per centimetre of length gained. 30-45 days/cm is the accepted benchmark for a normal external-fixator course; magnetic intramedullary nails achieve a similar index (~30 days/cm) without pin-site morbidity.
A: A cystic/poor regenerate means the distraction rate is too fast for that patient's biology. Slow the rate (to ~0.5-0.75 mm/day), check patient factors (smoking, nutrition, vitamin D), and if it persists consider the accordion manoeuvre (compress then re-distract) or bone grafting. Conversely, premature consolidation means the rate is too slow - speed up.
A: Problems resolve without an operation (e.g. pin-site infection settling on antibiotics); obstacles require an unplanned operation during treatment (e.g. contracture release, regenerate graft); complications are unresolved at the end of treatment or are intra-operative ("true") events. It is the universal language for reporting lengthening outcomes.
A: When 3 of 4 cortices are consolidated on orthogonal radiographs. Dynamise the frame first to confirm the regenerate bears load, and protect the limb (cast/brace, activity restriction) afterwards because regenerate fracture is a recognised early complication of premature removal.
At a Glance Table
- Answer
- 1 mm/day
- Why it matters
- Faster causes fibrous/cystic regenerate; slower causes premature consolidation
- Answer
- 0.25 mm four times daily (QID)
- Why it matters
- More frequent, smaller steps give better regenerate than a single daily turn
- Answer
- 5-7 days (children), 7-14 days (adults)
- Why it matters
- Allows initial callus; longer in smokers/poor bone
- Answer
- ~1 month per cm; healing index 30-45 days/cm
- Why it matters
- Benchmark for a normal external-fixator course
- Answer
- Classically ~20% of segment; stage if larger
- Why it matters
- Complication burden rises steeply with greater gains
- Answer
- Pin-site infection
- Why it matters
- Joint contracture is the most important functional one
- Answer
- 3 of 4 cortices consolidated on orthogonal films
- Why it matters
- Premature removal risks regenerate fracture
- External Fixator (Ilizarov/TSF)
- Required daily
- Internal Lengthening Nail (PRECICE)
- None
- External Fixator (Ilizarov/TSF)
- Lower - frame cumbersome
- Internal Lengthening Nail (PRECICE)
- Higher - no external device
- External Fixator (Ilizarov/TSF)
- Excellent (6 axes)
- Internal Lengthening Nail (PRECICE)
- Limited
- External Fixator (Ilizarov/TSF)
- Pin site infections common
- Internal Lengthening Nail (PRECICE)
- Lower
- External Fixator (Ilizarov/TSF)
- Lower
- Internal Lengthening Nail (PRECICE)
- Higher (implant cost)
- External Fixator (Ilizarov/TSF)
- Complex deformity + lengthening
- Internal Lengthening Nail (PRECICE)
- Isolated lengthening
LDCRDistraction Osteogenesis Phases
Hook:Latency-Distraction-Consolidation-Remodeling: The 4 phases of regenerate formation!
BLOODFactors Affecting Regenerate Quality
Hook:Good BLOOD supply and technique = good regenerate!
PAIN JCComplications of Lengthening
Hook:Lengthening causes PAIN JC - but manageable with good technique!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 10-year-old boy with left fibular hemimelia has a predicted limb length discrepancy of 6cm at maturity. His parents ask about treatment options.”
“You are 3 weeks into tibial lengthening on a 14-year-old with an Ilizarov frame. X-rays show a cystic regenerate with poor bone formation. The distraction rate has been 1mm/day.”
“A 16-year-old undergoing femoral lengthening for post-traumatic shortening develops a 30-degree knee flexion contracture at 4cm of lengthening. Target is 5cm.”
“A 15-year-old and his parents have agreed in principle to tibial lengthening with a circular frame. The examiner asks you to take consent. What do you tell them?”
“A 38-year-old has a 6 cm infected non-union of the tibia after an open fracture. After debridement you are left with a 6 cm segmental defect. How would you reconstruct it?”
Distraction Parameters
- Rate: 1mm/day standard
- Rhythm: 0.25mm QID (4 times daily)
- Latency: 5-7 days children, 7-14 days adults
- Maximum: 20% of bone length per session
Phases of Distraction Osteogenesis
- Latency: Initial callus formation (5-7 days)
- Distraction: Active lengthening
- Consolidation: 1 month per cm of lengthening
- Remodeling: Cortical maturation after frame removal
Regenerate Problems
- Cystic/poor regenerate: Too fast - slow down
- Premature consolidation: Too slow - speed up
- Accordion maneuver: Compress then re-distract
- Bone graft: For refractory poor regenerate
Corticotomy Technique
- Low-energy technique essential
- Preserve periosteum and endosteum
- Multiple drill holes + osteotome
- Metaphyseal location preferred
Device Selection
- External fixator: Complex deformity + lengthening
- Internal nail: Isolated lengthening, good bone
- TSF: Multiplanar correction needed
- LATN: Lengthening over nail then convert
Complications
- Pin site infection: Most common
- Joint contracture: Most significant functional
- Nerve injury: Stretch neuropathy - slow/stop
- Regenerate fracture: After frame removal
Evidence Base
Tension-Stress Effect Part II: Rate and Frequency of Distraction
- 0.5 mm/day frequently caused premature consolidation
- 2.0 mm/day produced ischaemic, undesirable changes in elongating tissues
- 1.0 mm/day was optimal; the greater the frequency of steps, the better the outcome
- Regenerate forms via a unique physis-like central growth zone
Tension-Stress Effect Part I: Stability and Soft-Tissue Preservation
- Stable fixation enhances osteogenesis
- Marrow element preservation is critical to regenerate formation
- New bone aligns parallel to the tension vector
- Damage to marrow inhibits osteogenesis
PRECICE Magnetic Femoral Lengthening: Antegrade vs Retrograde
- Mean healing index 31.6 days/cm (range 15-108)
- No deep infections; no nail failed to lengthen
- Antegrade nailing preserved hip/knee motion better than retrograde
- Five patients needed surgery for joint contracture
Lengthening Beyond 20% of Bone Length
- Goals up to 55% of bone length had significantly better outcomes
- Mean gain 33% of original length; healing index 37 days/cm
- All segments had problems; mean 1.3 obstacles and 0.9 complications each
- Supports staging large lengthenings rather than a single session
Multiplier Method for Predicting Limb Length at Maturity
- Mean bone-length prediction error 1.1 cm (chronological age)
- Requires only one data point unlike serial-charting methods
- More accurate than Anderson-Green growth-remaining charts
- Underpins timing of epiphysiodesis vs lengthening decisions
Magnetic Lengthening Nail vs Lengthening Over a Nail: Cost and Outcomes
- MLN: fewer procedures (2.1 vs 3.1, p less than 0.001)
- MLN: shorter time to union (100 vs 137 days, p = 0.001)
- Total cost similar between groups (p = 0.482)
- No difference in amount of femoral distraction achieved
Motorized Intramedullary Lengthening (Fitbone) - Early Series
- Target lengthening achieved in 88% of cases
- Mean lengthening 45 mm; complication rate 15.4%
- Healing index 73 days/cm (femur), 83.5 days/cm (tibia)
- Reliable and well tolerated at short-term follow-up
Paley Classification of Lengthening Complications
- Problems: resolve with non-operative measures
- Obstacles: require a planned operative intervention during treatment
- Complications: true (intra-op) and persist beyond treatment
- Healing index 30-45 days/cm = normal external-fixator course