Level Selection | Energy Expenditure | Prosthetic Outcomes | Surgical Technique by Level
- Energy expenditure increases proximally: Toe 0%, TMA 10-20%, BKA 40-60%, AKA 90-120%, hip disarticulation 200%+
- Transtibial minimum length: 12-15cm from tibial tuberosity for prosthetic lever arm
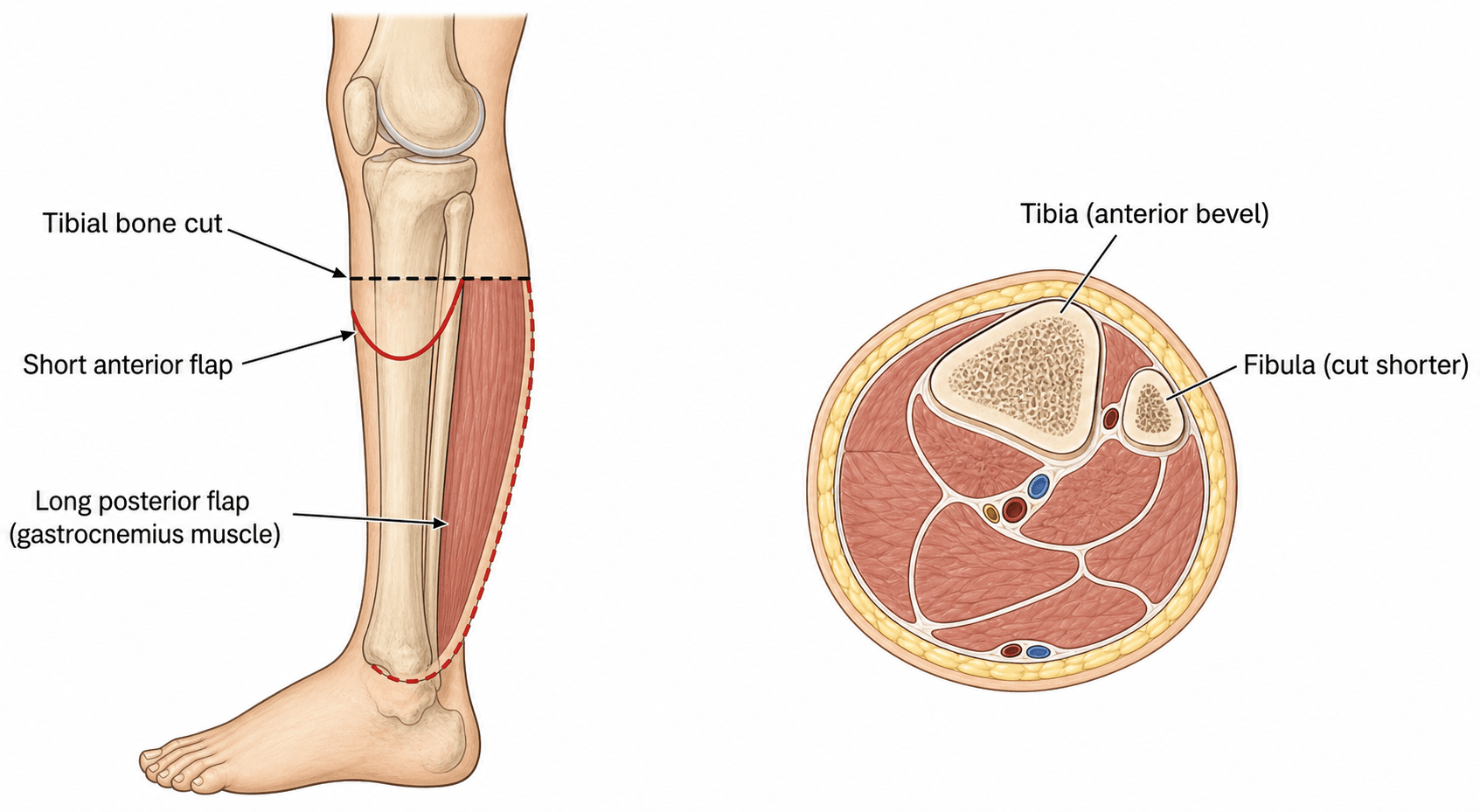
- Long posterior flap (Burgess technique) is gold standard for transtibial amputation
- Adductor myodesis to lateral femur prevents abduction contracture in transfemoral
- Syme amputation provides end-bearing but requires experienced surgeon and viable heel pad
- “Preserve the knee - energy expenditure 40-60% less with BKA vs AKA
- “TcPO2 greater than 30-40 mmHg predicts healing at proposed level
- “Bevel anterior tibia 45 degrees in BKA to prevent skin pressure
- “Fibula cut 1-2cm shorter than tibia to prevent pressure symptoms
This is an EXAM FAVOURITE. Energy cost increases with proximal amputation. Toe/ray: baseline. TMA: 10-20% increase. Transtibial: 40-60% increase. Transfemoral: 90-120% increase. Hip disarticulation: greater than 200% increase. Knee preservation is paramount - reduces energy by 40-60%.
Choose the most distal level that will heal. Consider: (1) Tissue viability - TcPO2, Doppler, clinical assessment (2) Functional requirements - prosthetic fitting, mobility goals (3) Patient factors - age, comorbidities, rehabilitation potential. Vascular surgery input essential in PVD.
Transtibial: Long posterior flap (Burgess), 45-degree anterior tibial bevel, fibula 1-2cm shorter, myodesis. Transfemoral: Equal anterior-posterior flaps, adductor myodesis to lateral femur (prevents abduction contracture), minimum 10-12cm from greater trochanter.
Adequate bone length for lever arm and soft tissue padding for socket. End-bearing levels (Syme, knee disarticulation) allow direct weight transfer. Transtibial requires PTB (patellar tendon bearing) socket. Transfemoral uses ischial containment socket. Early prosthetist involvement essential.
- Energy Increase
- 0-5%
- Healing Rate
- Variable (60-80%)
- Prosthetic Outcome
- No prosthesis needed
- Key Consideration
- High revision rate in PVD, watch for transfer ulcers
- Energy Increase
- 10-20%
- Healing Rate
- 70-80%
- Prosthetic Outcome
- Toe filler in shoe
- Key Consideration
- Achilles lengthening prevents equinovarus
- Energy Increase
- 20-40%
- Healing Rate
- 60-75%
- Prosthetic Outcome
- Difficult prosthetic fitting
- Key Consideration
- Equinus deformity common, rarely performed
- Energy Increase
- 20-40%
- Healing Rate
- 75-85%
- Prosthetic Outcome
- End-bearing, long lever arm
- Key Consideration
- Requires viable heel pad, experienced surgeon
- Energy Increase
- 40-60%
- Healing Rate
- 70-85%
- Prosthetic Outcome
- PTB socket, excellent function
- Key Consideration
- MOST IMPORTANT: Preserve the knee
- Energy Increase
- 60-80%
- Healing Rate
- 85-90%
- Prosthetic Outcome
- End-bearing, bulky knee
- Key Consideration
- No bone cut, good for non-ambulatory
- Energy Increase
- 90-120%
- Healing Rate
- 90-95%
- Prosthetic Outcome
- Ischial containment socket
- Key Consideration
- Adductor myodesis prevents abduction contracture
- Energy Increase
- Greater than 200%
- Healing Rate
- 95%+
- Prosthetic Outcome
- Canadian hip prosthesis, limited use
- Key Consideration
- Reserved for tumor, trauma - high mortality in vascular
TOES To THIGHAmputation Level Hierarchy
Hook:From TOES To THIGH - more proximal = more energy, less function
Overview and Level Selection Principles
Lower limb amputation levels range from toe amputation to hemipelvectomy. The choice of level is critical and determines functional outcome, prosthetic options, energy expenditure, and quality of life.
Key Principles of Level Selection:
- Most distal level that will heal - balance function against healing potential
- Preserve joints - especially the knee (reduces energy by 40-60%)
- Adequate bone length for prosthetic lever arm
- Sufficient soft tissue for durable, well-padded closure
- Consider prosthetic requirements - early prosthetist involvement
PRESERVE THE KNEE AT ALL COSTS. A short transtibial amputation that heals is vastly superior to a transfemoral amputation. Energy expenditure for ambulation with transtibial is 40-60% less than transfemoral. Even a very short transtibial (Mazet level) preserves knee proprioception and reduces energy demands.
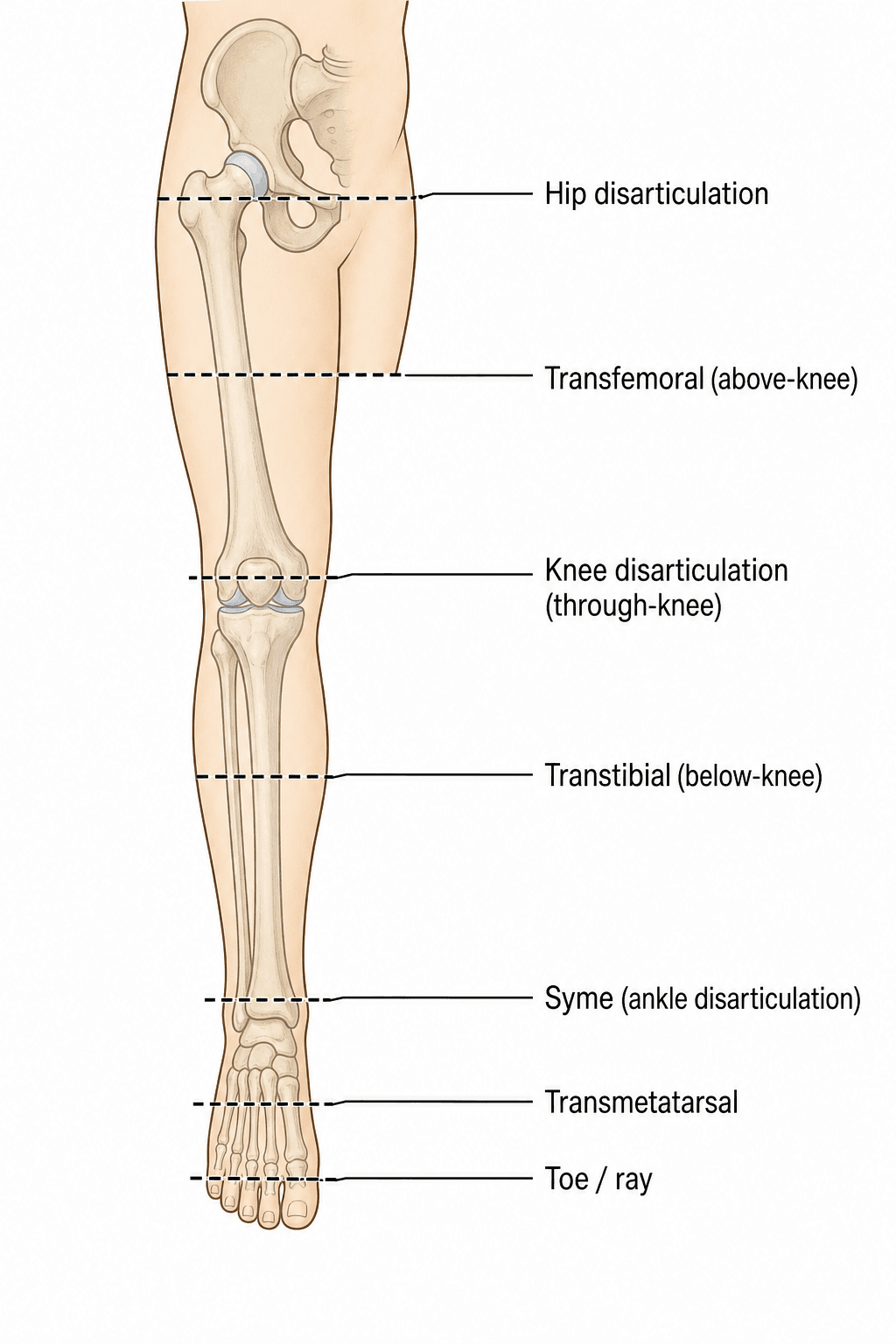
Amputation Level Categories:
- Toe amputation: Distal phalanx or toe disarticulation
- Ray amputation: Metatarsal and toe en bloc
- Transmetatarsal (TMA): Through metatarsal shafts
- Lisfranc: Tarsometatarsal disarticulation
- Chopart: Midtarsal disarticulation
- Syme: Ankle disarticulation with heel pad
- Transtibial (BKA): Most common major amputation
- Knee disarticulation: Through-knee amputation
- Transfemoral (AKA): Above-knee amputation
- Hip disarticulation: Complete limb removal
Pathophysiology and Energy Expenditure
Energy Expenditure in Amputation
Energy expenditure during ambulation increases with more proximal amputation levels. This is a critical exam topic and understanding the physiology is essential.
Mechanisms of Increased Energy:
- Loss of normal gait biomechanics - compensatory movements required
- Increased hip and trunk muscle work - to stabilize prosthesis
- Loss of ankle push-off - significant energy generator in normal gait
- Increased swing phase energy - heavier prosthetic components proximally
- Compensatory arm swing - increased upper body work
- % Increase Above Baseline
- 0-5%
- Walking Speed (% of normal)
- 95-100%
- Oxygen Consumption
- Minimal increase
- % Increase Above Baseline
- 10-20%
- Walking Speed (% of normal)
- 85-95%
- Oxygen Consumption
- Slight increase
- % Increase Above Baseline
- 20-40%
- Walking Speed (% of normal)
- 75-90%
- Oxygen Consumption
- Moderate increase
- % Increase Above Baseline
- 40-60%
- Walking Speed (% of normal)
- 65-80%
- Oxygen Consumption
- Significant increase
- % Increase Above Baseline
- 60-80%
- Walking Speed (% of normal)
- 55-70%
- Oxygen Consumption
- Substantial increase
- % Increase Above Baseline
- 90-120%
- Walking Speed (% of normal)
- 40-60%
- Oxygen Consumption
- Near doubling
- % Increase Above Baseline
- Greater than 200%
- Walking Speed (% of normal)
- Less than 40%
- Oxygen Consumption
- More than double baseline
Know these numbers: Transtibial (BKA) = 40-60% increase. Transfemoral (AKA) = 90-120% increase. This represents the energy SAVINGS of preserving the knee. Elderly vascular patients often cannot compensate for the energy demands of transfemoral amputation - many become wheelchair-bound.
Healing Considerations by Level
- Vascular supply - TcPO2, Doppler signals, clinical perfusion
- Tissue quality - infection, radiation, previous surgery
- Patient factors - diabetes, smoking, nutrition, renal disease
- Surgical technique - tension-free closure, adequate flaps
- More distal amputations have lower healing rates in vascular disease
- Transfemoral heals reliably (greater than 90%) but at functional cost
- Failed distal amputation requiring revision is worse than primary proximal
Transcutaneous oxygen tension (TcPO2) predicts healing:
- Greater than 40 mmHg: High probability of healing
- 20-40 mmHg: Indeterminate - clinical judgment required
- Less than 20 mmHg: High probability of healing failure
Always request TcPO2 at proposed amputation level in vascular patients.
ZERO TO DOUBLEEnergy Expenditure by Amputation Level
Hook:ZERO TO DOUBLE - energy goes from zero to more than double as you go proximal
Clinical Presentation and Level Assessment
Indications for Each Amputation Level
Foot Level Amputations (Toe, Ray, TMA)
- Localized gangrene of single toe
- Osteomyelitis limited to phalanges
- Frostbite with demarcated necrosis
- Trauma with non-viable toe
- Gangrene extending to metatarsal head
- Osteomyelitis involving MTPJ
- Deep space infection requiring drainage
- Central ray for web space infection
- Multiple toe gangrene
- Forefoot osteomyelitis
- Failed toe/ray amputations
- Adequate midfoot perfusion
- High revision rate in vascular disease (30-50%)
- Watch for transfer ulcers on remaining toes
- Achilles lengthening may be needed with TMA to prevent equinovarus
- Requires adequate midfoot blood supply
Level Selection Algorithm
Level Selection Decision-Making Process
Determine the underlying cause:
- Vascular: Assess perfusion, revascularization options
- Trauma: Injury pattern, soft tissue viability
- Infection: Sepsis control, staged approach
- Tumour: Margin requirements, staging
Vascular assessment:
- Clinical: Pulses, capillary refill, tissue viability
- TcPO2: Greater than 30-40 mmHg predicts healing
- Doppler: Ankle-brachial index, toe pressures
- Angiography if revascularization considered
Patient factors:
- Age and baseline mobility
- Cognitive function for prosthetic training
- Contralateral limb status
- Upper limb function (for transfers)
- Social support and living situation
Hierarchy of preservation:
- Preserve foot if possible (toe, ray, TMA)
- Preserve ankle (Syme) if heel pad viable
- PRESERVE KNEE - transtibial if possible
- Transfemoral if knee not salvageable
- Hip disarticulation only if absolutely necessary
Team involvement:
- Vascular surgery input for level in PVD
- Prosthetist early involvement
- Rehabilitation medicine
- Pain service (phantom pain prevention)
- Psychological support
Differential Diagnosis of the Amputation Indication
Before committing to amputation it is essential to confirm the underlying indication, because the cause dictates whether limb salvage is possible and what level is appropriate. The following differential distinguishes the conditions that present as a non-viable or threatened lower limb.
- Key Distinguishing Features
- Rest pain, tissue loss, absent pulses, low ABI/toe pressures, gradual onset
- Implication for Level / Salvage
- Revascularise first if feasible; level set by perfusion (TcPO2); often transtibial or transfemoral
- Key Distinguishing Features
- Sudden pain, pallor, pulselessness, paraesthesia, paralysis, poikilothermia (6 Ps)
- Implication for Level / Salvage
- Urgent revascularisation; amputation only if irreversible (fixed mottling, muscle rigor)
- Key Distinguishing Features
- Neuropathic ulcer, local infection, often palpable pulses, raised inflammatory markers
- Implication for Level / Salvage
- Source control and minor/foot-level amputation where perfused; staged if wet gangrene
- Key Distinguishing Features
- High-energy injury, soft-tissue loss, nerve/vessel disruption, contamination
- Implication for Level / Salvage
- Salvage vs amputation per LEAP principles; level dictated by viable tissue, not perfusion alone
- Key Distinguishing Features
- Mass, night pain, characteristic imaging, biopsy-proven; younger patients
- Implication for Level / Salvage
- Level set by oncological margins; salvage with endoprosthesis often preferred over amputation
- Key Distinguishing Features
- Rapidly spreading erythema, crepitus, systemic sepsis, pain out of proportion
- Implication for Level / Salvage
- Emergency debridement; guillotine amputation if life-threatening, definitive level later
Investigations for Level Selection
Investigation Protocol for Amputation Level Planning
Essential for vascular disease patients:
- Ankle-brachial index (ABI): Less than 0.4 suggests poor healing
- Toe pressures: Greater than 30 mmHg associated with healing
- TcPO2 at proposed levels: Greater than 30-40 mmHg predicts healing
- Duplex ultrasound: Arterial and venous patency
- CT angiography: If revascularization being considered
- Plain radiographs of affected limb
- Assess extent of bone disease (osteomyelitis, tumour)
- Contralateral limb assessment (vascular patients often bilateral)
- MRI for tumour margins, skip metastases
- CT for complex trauma, bone quality
- Nuclear medicine for infection localization
Preoperative optimization:
- FBC, coagulation: Anaemia, bleeding risk
- U and E, creatinine: Renal function (affects healing)
- HbA1c: Diabetes control (target less than 8%)
- Albumin, prealbumin: Nutritional status (greater than 30 g/L)
- CRP, ESR: Infection markers
- Blood cultures: If sepsis suspected
Team consultations:
- Vascular surgery: Revascularization options, level advice
- Prosthetist: Socket requirements, level optimization
- Anaesthesia: Perioperative pain plan (phantom pain prevention)
- Rehabilitation medicine: Function potential assessment
- Dietitian: Nutritional optimization
TcPO2 (Transcutaneous Oxygen Tension):
- Greater than 40 mmHg: 90%+ probability of healing
- 30-40 mmHg: 75-90% probability - usually proceed
- 20-30 mmHg: 50-75% - indeterminate, clinical judgment
- Less than 20 mmHg: Less than 50% - consider more proximal level
Request TcPO2 at BOTH the proposed level AND one level proximal.
Imaging Atlas - Prosthetic Outcomes
Shown only in this topic's images, osseointegration is examinable as a concept: a transcutaneous bone-anchored implant that replaces the socket prosthesis in selected amputees.
- Principle: a titanium implant is anchored into the residual bone (the same osseointegration principle as a dental implant) and a transcutaneous abutment passes through the skin (a permanent stoma) to connect directly to the prosthesis - bypassing the socket entirely.
- Indications: amputees with chronic socket problems - recurrent skin breakdown, socket pain, pistoning, residual-limb volume fluctuation, or a short transfemoral stump that cannot be socket-fitted.
- Advantages over a socket: osseoperception (direct mechanical/proprioceptive feedback through bone), no socket skin complications, improved sitting comfort and hip range of motion, easier donning, and better prosthetic control.
- The dominant risk/limitation: a permanent skin-implant interface prone to chronic peri-stomal superficial and deep infection (the main complication), plus peri-prosthetic fracture and implant loosening. It requires staged surgery and a structured graded-loading rehabilitation programme, and is contraindicated in active infection or poor bone stock.
Exam point: osseointegration replaces the socket with a direct bone-anchored implant for socket-intolerant amputees - better osseoperception and no socket skin problems, at the cost of a permanent transcutaneous stoma and its infection risk.
Management Principles by Level
Universal Principles for All Levels
- Optimize medical comorbidities (diabetes, cardiac, renal)
- Smoking cessation (counsel and pharmacotherapy; smoking significantly impairs healing)
- Nutritional optimization (albumin greater than 30 g/L)
- Early prosthetist involvement
- Psychological preparation and support
- Appropriate level based on healing potential
- Adequate bone length for lever arm
- Sufficient soft tissue for tension-free closure
- Myodesis (muscle to bone) for optimal function
- Proper nerve handling - traction neurectomy
- Rigid dressing or IPOP (immediate post-op prosthesis)
- Edema control - compression
- Phantom pain management
- Early rehabilitation and prosthetic fitting
- Psychological support
Myodesis = muscle sutured directly to bone through drill holes or anchors Myoplasty = muscle sutured to opposing muscle or fascia
Myodesis is the gold standard - provides:
- Physiological muscle tension
- Better proprioception
- Stable residual limb shape
- Improved prosthetic control
Surgical Technique by Level
Toe Amputation Technique
Localized gangrene, osteomyelitis of phalanx, frostbite
- Racquet incision around base of toe
- Disarticulate at MTPJ or PIPJ
- Identify and ligate digital vessels
- Transect digital nerves under traction
- Close with interrupted sutures
- Leave open if infected (delayed primary closure)
Ray Amputation Technique
Gangrene to metatarsal head, MTPJ osteomyelitis
- Racquet incision extending onto dorsum of foot
- Incise along metatarsal shaft
- Disarticulate at tarsometatarsal joint (or cut metatarsal)
- Remove metatarsal and toe en bloc
- Preserve intermetatarsal ligaments if possible
- Close with slight narrowing of foot
- Consider first or fifth ray specifically
First ray amputation: Preserves lateral foot but loses medial weight bearing - shifts weight laterally. Fifth ray amputation: Preserves medial column but narrows foot. Central rays (2nd, 3rd): Can be removed with minimal functional loss. Multiple rays: Consider TMA instead if greater than 2 rays involved.
FLAPSTranstibial Amputation Technique
Hook:Good FLAPS make a good stump - remember the Burgess long posterior flap
Complications
Wound-Related Complications
- Incidence
- 10-20%
- Risk Factors
- Diabetes, PVD, malnutrition
- Management
- Antibiotics, drainage, debridement
- Incidence
- 5-15%
- Risk Factors
- Tension closure, poor perfusion
- Management
- VAC therapy, revision if extensive
- Incidence
- 5-30% (level dependent)
- Risk Factors
- Wrong level selection, PVD
- Management
- Debridement, proximal revision
- Incidence
- 5-10%
- Risk Factors
- Poor hemostasis, anticoagulation
- Management
- Aspiration or surgical evacuation
- Toe/Ray: 30-50% in vascular disease
- TMA: 20-40%
- Transtibial: 10-20%
- Transfemoral: 5-10%
More distal amputations have higher revision rates but better function if successful.
Prosthetic prescription is built on the patient's functional potential, and the K-level (Medicare Functional Classification Level) is the standard framework examiners expect.
- K0: no ability or potential to ambulate or transfer safely - a prosthesis does not aid mobility (not a candidate).
- K1: transfers or ambulates on level ground at a fixed cadence (household ambulator) - basic feet (SACH/single-axis), a locked or constant-friction knee.
- K2: limited community ambulator able to negotiate low barriers (kerbs, stairs, uneven ground) - flexible/multi-axial feet.
- K3: community ambulator with variable cadence - energy-storing (dynamic-response) feet and a fluid/pneumatic or microprocessor knee.
- K4: high-impact/athletic demands (child, active adult, athlete) - high-performance dynamic feet and specialised knees.
SACH (solid-ankle cushion-heel, no moving parts, K1-2) -> single-axis -> multi-axial (accommodates uneven ground) -> energy-storing/dynamic-response carbon feet (K3-4).
locked (most stable, K1) -> single-axis constant-friction -> polycentric (four-bar) -> fluid/pneumatic (variable cadence, K3) -> microprocessor knees (e.g. C-leg) that sense the gait cycle and provide stumble resistance to reduce falls (K3-4).
Exam point: match the prosthesis to the K-level - the K-level determines (and governs eligibility for) the foot and knee componentry the patient should receive.
Guidelines, Registries & Global Practice
Global Epidemiology
Worldwide, the dominant causes of major lower limb amputation are peripheral arterial occlusive disease (PAOD) and diabetic foot disease; trauma, malignancy and congenital deformity account for the remainder and predominate in younger patients. A GBD-2017 analysis of EU15+ countries (Hughes et al., 2020) found that despite a falling incidence of PAOD, trends in lower extremity amputation incidence were highly variable between countries and did not consistently decline. Australia recorded the highest age-standardised incidence rates for all amputation categories at every time point and the greatest overall increase, whereas the USA achieved the largest reductions over 1990 to 2017.
- Predominant Indication
- Diabetic foot sepsis and PAOD in an ageing population
- Typical Pattern
- Most amputations in those over 60; persistent or rising incidence despite revascularisation
- Predominant Indication
- Trauma (road traffic, occupational) and late-presenting infection
- Typical Pattern
- Younger patients, higher proportion of traumatic and major-level amputations
- Predominant Indication
- Blast and high-energy trauma
- Typical Pattern
- Young, often bilateral; transfemoral and through-knee over-represented
Guideline Comparison
- Core Guidance Relevant to Level
- Revascularise where feasible before deciding level; choose the most distal level likely to heal; perfusion testing (ankle/toe pressures, TcPO2) to guide healing
- Evidence Basis
- Systematic-review-based recommendations (GRADE)
- Core Guidance Relevant to Level
- Multidisciplinary limb-preservation pathway; assess perfusion before amputation; preserve the knee whenever healing allows
- Evidence Basis
- Consensus on RCT and registry evidence
- Core Guidance Relevant to Level
- Early specialist multidisciplinary input; rehabilitation-focused level selection; standards for time to surgery and prosthetic referral
- Evidence Basis
- Standards / consensus (BOAST)
- Core Guidance Relevant to Level
- Most distal viable level; long posterior flap a benchmark transtibial technique; structured perioperative pain and rehabilitation
- Evidence Basis
- Expert consensus on cohort and trial data
Across IWGDF, European, UK and US guidance the principles are consistent: assess and optimise perfusion (revascularise if possible) before committing to a level, choose the most distal level that will heal, and preserve the knee wherever healing allows. Differences are largely in service organisation (limb-preservation pathways, time-to-surgery standards) rather than in the core surgical decision.
Registry Evidence and Practice Variation
National vascular and amputation registries (for example UK National Vascular Registry/NVR audits, Vascunet collaborations and the SerbVasc registry) consistently report that major amputation carries high perioperative mortality - in-hospital mortality after above-knee amputation is frequently around 10% - and that only a minority of patients undergo revascularisation before amputation. Registry data also reveal wide practice variation in the ratio of major to minor amputations and in transtibial-versus-transfemoral selection between centres, much of which reflects case mix, access to revascularisation and multidisciplinary footcare rather than surgical preference alone.
- Health-equity gradients are marked: across high-income settings, disadvantaged and minority populations — including Indigenous peoples (for example Aboriginal and Torres Strait Islander Australians, who experience substantially higher diabetes-related amputation rates than non-Indigenous Australians) and comparable groups internationally — carry a disproportionate amputation burden. This reflects disparities in diabetes prevalence, access to multidisciplinary foot care and timely revascularisation rather than biological differences, and targeted, culturally safe prevention and foot-protection services narrow the gap.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 72-year-old diabetic male with peripheral vascular disease presents with gangrene of his left forefoot extending to the base of all toes. His previous femoral-popliteal bypass is occluded. TcPO2 at the ankle is 25 mmHg and at 15cm below the knee is 42 mmHg. What amputation level would you recommend and why?”
“Describe the surgical technique for transtibial amputation, highlighting the key technical points that optimize function and prosthetic fitting.”
“A 45-year-old man requires transfemoral amputation for a high-grade osteosarcoma of the distal femur. What are the key technical considerations for this amputation that differ from a vascular amputation?”
Energy Expenditure - KNOW THESE NUMBERS
- Toe/Ray: 0-5% increase
- TMA: 10-20% increase
- Syme: 20-40% increase
- Transtibial (BKA): 40-60% increase
- Knee disarticulation: 60-80% increase
- Transfemoral (AKA): 90-120% increase
- Hip disarticulation: Greater than 200% increase
- PRESERVE THE KNEE - saves 40-60% energy vs AKA
Transtibial Key Points (FLAPS)
- Flap: Long posterior (Burgess technique)
- Length: Minimum 12-15cm from tibial tuberosity
- Anterior bevel: 45 degrees on tibia
- Position fibula: 1-2cm shorter than tibia
- Suture myodesis: Posterior muscles to anterior tibia
Transfemoral Key Points
- Equal anterior-posterior flaps
- Minimum 10-12cm from greater trochanter
- ADDUCTOR MYODESIS to lateral femur - prevents abduction contracture
- Sciatic nerve - ligate vessel before transection
- Myodesis of quadriceps and hamstrings over bone
Level Selection Algorithm
- TcPO2 greater than 40 mmHg: 90%+ healing
- TcPO2 20-40 mmHg: Indeterminate
- TcPO2 less than 20 mmHg: High failure risk
- Vascular surgery input for level in PVD
- Most distal level that will heal
- Failed distal worse than primary proximal
Complications to Know
- Phantom limb pain: 70-80% incidence
- Knee flexion contracture (BKA): Prone lying, stretching
- Hip abduction contracture (AKA): Adductor myodesis prevents
- Equinovarus (TMA): TAL prevents
- Neuroma: Traction neurectomy technique
Emergency Amputation
- Guillotine amputation for life-threatening sepsis
- All tissues at same level, no closure
- VAC dressing
- Revise in 48-72 hours when stable
- Life before limb principle
Evidence Base
Energy Cost of Walking of Amputees: The Influence of Level of Amputation
- Seminal study (70 unilateral amputees, 40 normal controls) establishing energy cost of prosthetic walking by level
- In both traumatic and vascular amputees, gait performance was significantly better the lower the level of amputation
- Self-selected walking speed and oxygen cost worsened progressively from Syme to transtibial to transfemoral
- Vascular amputees walked slower and at higher energy cost than traumatic amputees at the same level
- Conclusion: when preservation of function is the chief concern, amputate at the lowest possible level
LEAP Study - An Analysis of Outcomes of Reconstruction or Amputation After Leg-Threatening Injuries
- Prospective multicentre observational study of 569 patients with severe leg injuries (Lower Extremity Assessment Project)
- No significant difference in Sickness Impact Profile at 2 years between amputation and reconstruction (12.6 vs 11.8, p=0.53)
- Reconstruction patients were more likely to be rehospitalised for a major complication (47.6% vs 33.9%, p=0.002)
- Similar return-to-work rates by 2 years (amputation 53.0%, reconstruction 49.4%)
- Poorer outcome predicted by major-complication rehospitalisation, low education, poverty, weak social support, low self-efficacy, smoking and litigation
Type of Incision for Below-Knee Amputation (Cochrane Systematic Review)
- Three RCTs (309 participants) of incision type for below-knee amputation in ischaemia or diabetic foot sepsis
- Skew flaps and sagittal flaps conferred no advantage over the established long posterior (Burgess) flap (primary stump healing 60% for both skew and long posterior; RR 1.00, 95% CI 0.71 to 1.42)
- For wet gangrene, a two-stage procedure (guillotine ankle amputation then definitive long posterior flap) gave better primary stump healing than one-stage (Peto OR 0.08, 95% CI 0.01 to 0.89)
- Reamputation, post-operative infection and prosthetic mobility were similar across techniques
- Overall quality of evidence judged moderate
Segmental Transcutaneous Measurements of PO2 in Patients Requiring Below-Knee Amputation
- Evaluated transcutaneous PO2 in 37 patients needing below-knee amputation for peripheral vascular insufficiency
- All 15 patients with below-knee TcPO2 of 40 mmHg or more healed without delay
- 17 of 19 patients with TcPO2 above zero but less than 40 mmHg healed at the below-knee level (2 after local revision)
- All 3 patients with a below-knee TcPO2 of zero required re-amputation above the knee
- Transcutaneous oximetry quantifies healing potential at candidate amputation levels
Mirror Therapy for Phantom Limb Pain
- Randomised, controlled crossover trial in lower-limb amputees with phantom limb pain (military cohort)
- Three arms compared: mirror therapy, a covered (opaque) mirror, and mental visualisation
- Phantom limb pain decreased in the mirror-therapy group, while the covered-mirror and mental-imagery groups did not improve or worsened
- Patients who crossed over to mirror therapy after failing other treatments also improved
- Proposed mechanism: visual feedback of the intact limb resolves a sensorimotor (cortical) conflict
Skew Flap Versus Long Posterior Flap in Below-Knee Amputations: Multicentre Trial
- Multicentre RCT (11 centres, 191 patients) of skew flap (n=98) versus long posterior flap (n=93) for below-knee amputation in end-stage occlusive vascular disease
- Primary wound healing at 1 week was 60% in both groups
- 30-day mortality (11% skew vs 17% long posterior), same-level revision and revision to a higher level did not differ significantly
- At 6 months a prosthesis was fitted to 84% (skew) and 77% (long posterior); walking achieved in 78% and 71% respectively, with no significant difference
- Concluded the skew flap is as effective as the long posterior flap for below-knee amputation