Motion Preservation Alternative to Fusion | Strict Patient Selection | Anterior Approach
IMPLANT DESIGN CATEGORIES
Critical Must-Knows
- Primary indication = single or two-level DDD (L4-S1) with discogenic pain, failed conservative care
- Contraindications: Facet arthropathy, spondylolisthesis, previous surgery at level, osteoporosis, stenosis
- Motion preservation theoretically reduces adjacent segment disease (ASD) compared to fusion
- Anterior retroperitoneal approach (ALIF) required - major vascular structures at risk
- Patient selection critical - strict criteria essential for good outcomes
Clinical Pearls
- "Ideal candidate: young (under 60), single-level L4-5 or L5-S1, no facet disease, good bone quality
- "Cannot perform if previous posterior surgery at same level (scar tissue)
- "Vascular injury (iliac vessels) is main intraoperative risk
- "Retrograde ejaculation risk from hypogastric plexus injury at L5-S1
- "Non-inferior to fusion in FDA IDE trials (Charite, ProDisc-L)
Clinical Imaging
Imaging Gallery


Critical Lumbar TDR Exam Points
Strict Indications
Single or two-level DDD (L4-5, L5-S1 only). Discogenic pain confirmed by provocative discography or MRI. Failed conservative treatment over 6 months. No significant facet arthropathy (excludes patient). Maintained disc height (at least 4mm). Age typically under 60 years.
Critical Contraindications
Absolute: Facet arthropathy (pain generator not addressed), spondylolisthesis greater than Grade I, spinal stenosis, previous surgery at target level, osteoporosis (T-score less than negative 1.5), active infection, pregnancy. Relative: Obesity (BMI over 35), metal allergy, more than two levels.
Vascular Approach Risks
Anterior retroperitoneal approach required. At L5-S1: access between aortic bifurcation and left common iliac vein. At L4-5: requires left common iliac vein mobilization (higher risk). Vascular injury is most feared complication - access surgeon recommended. Retrograde ejaculation from sympathetic plexus injury (1-5% at L5-S1).
Motion Preservation Rationale
Fusion transfers stress to adjacent segments, theoretically accelerating adjacent segment disease (ASD). TDR preserves 5-15° range of motion per level, maintaining more physiologic biomechanics. However, long-term ASD reduction benefit remains theoretical - data still evolving beyond 10 years.
At a Glance
Lumbar total disc replacement (TDR) is a motion-preserving alternative to fusion for single or two-level degenerative disc disease at L4-S1 in carefully selected patients, theoretically reducing adjacent segment disease by preserving 5-15° range of motion per level. The ideal candidate is under 60 years, has isolated discogenic pain confirmed by MRI or discography, no significant facet arthropathy, and good bone quality—the mnemonic "FOSSILS" captures contraindications: Facet arthropathy, Osteoporosis, Spondylolisthesis, Stenosis, Infection, Levels (greater than 2), Surgery at level. The anterior retroperitoneal approach places major vascular structures at risk, with iliac vessel injury being the most feared complication; retrograde ejaculation from hypogastric plexus injury occurs in 1-5% at L5-S1. FDA IDE trials (Charité, ProDisc-L) demonstrate non-inferiority to fusion, though long-term adjacent segment disease reduction remains theoretical.
FOSSILSTDR Contraindications
| F | Facet arthropathy Major pain generator not addressed by TDR |
| O | Osteoporosis Endplate subsidence risk (T-score less than negative 1.5) |
| S | Spondylolisthesis Instability contraindicated (greater than Grade I) |
| S | Stenosis (spinal) Needs decompression, not motion preservation |
| I | Infection Active or previous discitis at target level |
| L | Levels (more than 2) Multi-level disease not FDA approved |
| S | Surgery (previous at level) Scarred disc space, altered anatomy |
| F | Facet arthropathy Major pain generator not addressed by TDR | S | Stenosis (spinal) Needs decompression, not motion preservation | S | Surgery (previous at level) Scarred disc space, altered anatomy |
| O | Osteoporosis Endplate subsidence risk (T-score less than negative 1.5) | I | Infection Active or previous discitis at target level | ||
| S | Spondylolisthesis Instability contraindicated (greater than Grade I) | L | Levels (more than 2) Multi-level disease not FDA approved |
Hook:FOSSILS = Ancient, outdated patients for disc arthroplasty - these patients need fusion instead!
YOUNG-DISCIdeal TDR Candidate
| Y | Young (under 60 years) Longer expected benefit from motion preservation |
| O | One or two levels only Typically L4-5 or L5-S1, FDA-approved levels |
| U | Unchanged facets No facet arthropathy or posterior element disease |
| N | No previous surgery at level Virgin disc space, no scar tissue |
| G | Good bone quality Normal BMD, no osteoporosis (T-score greater than negative 1.5) |
| D | Discogenic pain confirmed Provocative discography or high-intensity zone on MRI |
| I | Isolated disc disease No stenosis, no multilevel degeneration |
| S | Sufficient disc height At least 4mm remaining height for implant placement |
| C | Conservative treatment failed Minimum 6 months of non-operative management |
| Y | Young (under 60 years) Longer expected benefit from motion preservation | N | No previous surgery at level Virgin disc space, no scar tissue | I | Isolated disc disease No stenosis, no multilevel degeneration |
| O | One or two levels only Typically L4-5 or L5-S1, FDA-approved levels | G | Good bone quality Normal BMD, no osteoporosis (T-score greater than negative 1.5) | S | Sufficient disc height At least 4mm remaining height for implant placement |
| U | Unchanged facets No facet arthropathy or posterior element disease | D | Discogenic pain confirmed Provocative discography or high-intensity zone on MRI | C | Conservative treatment failed Minimum 6 months of non-operative management |
Hook:YOUNG-DISC candidates are young patients with isolated disc disease perfect for motion preservation!
ACCESSTDR Surgical Approach Steps
| A | Anterior midline incision Infraumbilical for L5-S1, extended for L4-5 |
| C | Clear peritoneum laterally Retroperitoneal dissection to spine |
| C | Control vessels (mobilize) Retract aorta/IVC, protect iliac vessels |
| E | Expose disc space Between vessels at L5-S1, mobilize veins at L4-5 |
| S | Sympathetic plexus preserve Protect hypogastric plexus (retrograde ejaculation risk) |
| S | Secure implant placement Trial sizing, final implant insertion with imaging |
| A | Anterior midline incision Infraumbilical for L5-S1, extended for L4-5 | C | Control vessels (mobilize) Retract aorta/IVC, protect iliac vessels | S | Sympathetic plexus preserve Protect hypogastric plexus (retrograde ejaculation risk) |
| C | Clear peritoneum laterally Retroperitoneal dissection to spine | E | Expose disc space Between vessels at L5-S1, mobilize veins at L4-5 | S | Secure implant placement Trial sizing, final implant insertion with imaging |
Hook:ACCESS the spine anteriorly with careful vascular control and sympathetic preservation
Overview and Rationale
Lumbar total disc replacement (TDR) is a motion-preserving alternative to spinal fusion for the treatment of degenerative disc disease (DDD). The fundamental goal is to relieve discogenic axial low back pain while maintaining segmental motion at the affected level, theoretically reducing the development of adjacent segment disease (ASD) that commonly follows fusion procedures.
Historical Development
The concept of disc arthroplasty dates to the 1960s with early attempts using stainless steel ball-and-socket designs (Fernström). Modern TDR evolved in the 1980s-1990s with improved biomechanical understanding and materials science. The Charité artificial disc (SB Charité III, DePuy Spine) was the first FDA-approved device in 2004, followed by ProDisc-L (Synthes) in 2006. Multiple other designs have gained European CE marking but not FDA approval in the United States.
Biomechanical Rationale
Adjacent Segment Disease (ASD) is a well-documented phenomenon following spinal fusion, with radiographic changes developing in 8-30% of patients at 10 years and clinical ASD requiring reoperation in 2-4% per year. The pathophysiology involves:
- Increased intradiscal pressure at adjacent levels (up to 45% increase)
- Altered kinematics with hypermobility compensation
- Facet joint overload from loss of normal load sharing
- Accelerated disc degeneration from abnormal stress concentration
TDR aims to maintain physiologic motion (5-15° flexion-extension per level), preserve normal intradiscal pressure distribution, and reduce stress transfer to adjacent segments. However, whether TDR truly prevents ASD versus fusion remains controversial, with long-term data (greater than 10 years) still accumulating.
Clinical Evidence Summary
Multiple Level I randomized controlled trials comparing TDR to fusion have demonstrated:
- Non-inferior clinical outcomes at 2, 5, and 10 years
- Equivalent pain relief and functional improvement
- Preserved motion at the index level (average 7-10°)
- Lower reoperation rates at adjacent levels in some studies
- Similar overall complication rates but different complication profiles
The FDA Investigational Device Exemption (IDE) trials for Charité and ProDisc-L established TDR as a viable alternative for highly selected patients.
Implant Designs and Biomechanics
SB Charité III (DePuy Spine)
Design: Three-component mobile-bearing device with unconstrained ultra-high molecular weight polyethylene (UHMWPE) core between two cobalt-chromium-molybdenum (CoCrMo) endplates.
Biomechanics:
- Unconstrained motion allows translation and rotation
- Low constraint may reduce stress on bone-implant interface
- Self-centering core design intended to maintain center of rotation
- Potential for core dislocation with improper positioning
Clinical Use:
- First FDA-approved device (2004)
- FDA IDE trial showed non-inferiority to circumferential fusion
- Strict midline placement required to prevent core subluxation
- Sagittal alignment restoration more challenging than fixed-bearing designs
Outcomes:
- 73.7% success rate at 2 years in FDA trial
- Motion preservation: average 7.8° at 5 years
- Heterotopic ossification rate: 35-65% (may limit motion)
The mobile-bearing design philosophy emphasizes reduced constraint to minimize implant-bone stress, but requires precise surgical technique for optimal outcomes.
Implant Selection Considerations
TDR Design Comparison
| Feature | Mobile-Bearing (Charité) | Fixed-Bearing (ProDisc-L) | Metal-on-Metal (Maverick) |
|---|---|---|---|
| Components | 3 (endplates + core) | 2 (integrated inlay) | 2 (metal-on-metal) |
| Motion constraint | Unconstrained | Semi-constrained | Semi-constrained |
| Center of rotation | Variable (core migrates) | Fixed posterior | Fixed central |
| Lordosis restoration | Limited | Excellent (angled endplates) | Good |
| Technique sensitivity | High (positioning critical) | Moderate | Moderate |
| Wear concerns | UHMWPE wear debris | UHMWPE wear debris | Metallosis |
| FDA status (US) | Approved 2004 | Approved 2006 | Humanitarian device only |
Patient Selection and Indications
Critical Concept: Patient selection is the single most important determinant of TDR success. Expanding indications beyond strict criteria leads to poor outcomes and high complication rates. When in doubt, fusion is the safer option.
FDA-Approved Indications
Primary Indication: Single-level symptomatic degenerative disc disease at L4-5 or L5-S1 (ProDisc-L approved for single level; Charité approved for single or two-level).
Specific Criteria:
- Failed conservative treatment: Minimum 6 months of non-operative management including physical therapy, medications, injections
- Discogenic pain: Concordant pain provocation on discography OR high-intensity zone (HIZ) on T2-weighted MRI
- Maintained disc height: At least 4mm remaining height (some implants require at least 5mm)
- Age: Typically 18-60 years (upper age limit varies by study and surgeon preference)
- No facet arthropathy: Less than Grade 2 facet degeneration on imaging
- No posterior element disease: Intact pars, no spondylolisthesis
- Skeletally mature: Closed physes confirmed
Absolute Contraindications
These conditions completely exclude a patient from TDR consideration:
-
Facet joint arthropathy: Moderate to severe facet degeneration (Fujiwara Grade 2 or higher). TDR does not address facetogenic pain.
-
Spondylolisthesis: Any grade of degenerative spondylolisthesis. Isthmic spondylolisthesis at any grade. Motion preservation inappropriate with baseline instability.
-
Spinal stenosis: Central canal stenosis requiring decompression. Lateral recess stenosis. Foraminal stenosis (TDR does not decompress).
-
Previous surgery at target level: Prior discectomy, laminectomy, or fusion at the same level. Scar tissue and altered anatomy preclude safe TDR placement.
-
Osteoporosis: T-score less than negative 1.5 on DEXA scan. High risk of endplate subsidence and implant migration.
-
Active infection: Discitis, osteomyelitis, or systemic infection. Metal implant contraindicated.
-
Severe disc collapse: Less than 4mm remaining disc height. Insufficient space for implant, altered biomechanics.
-
Pregnancy: Current pregnancy (relative) or planned pregnancy within 2 years (relative).
-
Allergy to implant materials: Documented metal allergy to cobalt, chromium, molybdenum, or titanium.
-
Severe osteopenia: Insufficient bone quality for implant fixation.
Relative Contraindications
These factors increase risk and require careful individualized decision-making:
- Obesity: BMI over 35 kg per square meter (approach difficulties, increased mechanical loading)
- Smoking: Active tobacco use (impairs wound healing, may affect outcomes)
- Multilevel disease: More than two levels of symptomatic DDD (not FDA approved for more than two levels)
- Age over 60: Limited life expectancy for motion preservation benefit
- Workers' compensation: Some studies show worse outcomes in compensation cases
- Litigation: Ongoing injury litigation associated with poor outcomes
- Psychological factors: Untreated depression, chronic pain syndrome
- Morbid obesity: BMI over 40 (vascular access challenges)
Ideal Candidate Profile
The perfect TDR candidate:
- Age 30-50 years old
- Single-level L4-5 or L5-S1 DDD
- Discogenic pain confirmed by provocative discography
- At least 6 months failed conservative care
- No facet arthropathy (Grade 0-1)
- Normal sagittal alignment
- No spondylolisthesis
- Normal bone density (T-score greater than negative 1.0)
- Non-smoker
- BMI less than 30
- No previous lumbar surgery
- Psychologically healthy, realistic expectations
- Not involved in litigation or workers' compensation
In reality, few patients meet all ideal criteria, requiring clinical judgment about which deviations are acceptable.
Imaging Gallery - Patient Selection and Radiographic Outcomes
Surgical Technique
Vascular Surgery Standby: Many surgeons recommend having a vascular surgeon available or performing the approach, particularly for L4-5 where left common iliac vein mobilization is required. Have vascular instruments and blood products available.
Imaging Analysis
Standing lateral radiograph:
- Measure disc height at target level (at least 4-5mm required)
- Assess sagittal alignment (lordosis, pelvic parameters)
- Identify transitional anatomy (sacralization, lumbarization)
- Measure implant size needed (AP and lateral dimensions)
MRI review:
- Confirm disc degeneration (Pfirrmann grade)
- Rule out facet arthropathy (greater than Grade 2 excludes patient)
- Identify high-intensity zone (HIZ) if present
- Rule out stenosis (central, lateral, foraminal)
- Assess adjacent level disease
CT scan (if needed):
- Better evaluate facet joints
- Assess endplate integrity
- Identify vascular calcification
- Rule out posterior element pathology
Flexion-extension radiographs:
- Rule out instability (greater than 3mm translation or greater than 10° angulation)
- Assess motion at target level (if already fused spontaneously, TDR not indicated)
Implant Sizing
Most systems use trial implants with fluoroscopic verification:
- Anteroposterior size: Typically 38-50mm (avoid anterior cortex overhang)
- Mediolateral size: Typically 30-42mm (stay within lateral borders)
- Height: Match native disc height or restore slightly (avoid over-distraction)
- Lordotic angle: ProDisc-L offers 6° or 11° options for sagittal balance
Patient Positioning
- Supine on radiolucent table
- Slight Trendelenburg (15-20°) to move bowel contents cephalad
- Arms tucked or positioned on arm boards (not extended over head)
- Hip flexion minimal to reduce tension on femoral vessels
- C-arm positioning: Test lateral view before draping (true lateral critical)
Preoperative planning ensures appropriate patient selection, correct implant sizing, and anticipation of anatomical challenges during the anterior approach.
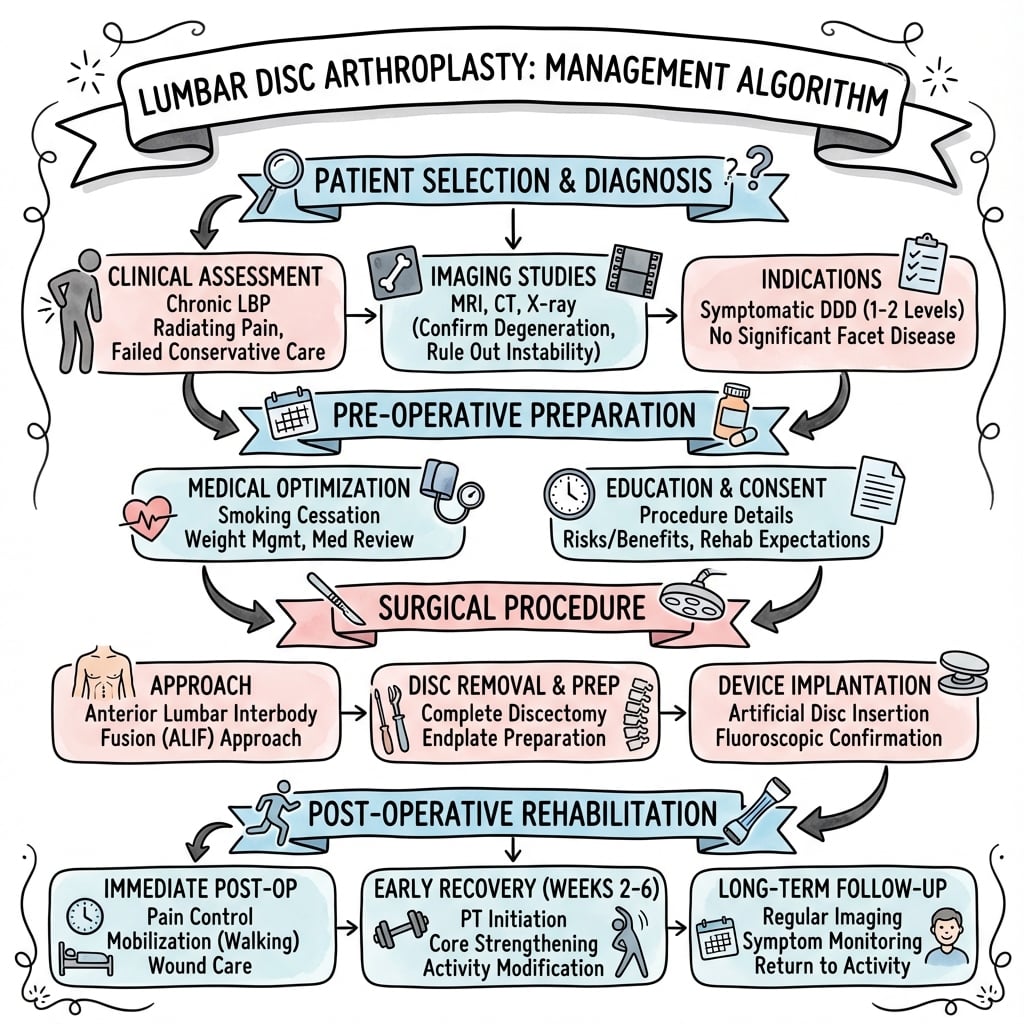
Management Algorithm
Complications
Intraoperative Complications
Vascular Injury (1-3%):
- Most feared complication during anterior approach
- Iliac vessels at highest risk (vein greater than artery)
- Left common iliac vein particularly vulnerable at L4-5
- Management: Immediate vascular surgery consultation, direct repair, possible blood transfusion
- Prevention: Gentle retraction, good lighting, vascular surgeon availability
Visceral Injury:
- Bowel perforation: Rare if peritoneum intact (recognize and repair primarily)
- Ureter injury: Retract with peritoneum, identify and protect
- Bladder injury: Rare (more common with low transverse incisions)
Neurological Injury:
- Nerve root injury: Rare (posterior approach risk, not anterior)
- Sympathetic plexus injury: 1-5% at L5-S1 (retrograde ejaculation in males)
Implant Malposition:
- Recognized intraoperatively with fluoroscopy
- Requires removal and repositioning if significant
- Easier with trial implants (check before final)
Early Postoperative Complications (Less Than 6 Weeks)
Retrograde Ejaculation:
- Incidence: 1-5% at L5-S1, less than 1% at L4-5
- Mechanism: Hypogastric plexus stretch or thermal injury
- Presentation: Inability to ejaculate (orgasm intact, dry ejaculation)
- Management: Usually permanent (counsel preoperatively), urology referral for fertility issues
- Prevention: Protect plexus during retraction, avoid cautery near plexus, gentle handling
Wound Complications:
- Infection: 1-2% (prophylactic antibiotics standard)
- Hematoma: Rare (retroperitoneal approach less dead space)
- Dehiscence: Rare with proper fascial closure
Ileus:
- Incidence: 5-10% (bowel manipulation during retraction)
- Management: Conservative (NPO, NG tube if needed)
- Usually resolves within 3-5 days
Subsidence:
- Early subsidence (first 6 weeks) suggests osteoporosis or endplate violation
- Imaging: Serial radiographs to monitor (greater than 3mm concerning)
- Management: Usually observational if asymptomatic; fusion if progressive/symptomatic
Late Complications (Greater Than 6 Weeks)
Heterotopic Ossification (HO):
- Incidence: 5-60% depending on grading system (clinically significant HO: 5-15%)
- Mechanism: Ectopic bone formation in paraspinal soft tissues (not in disc space)
- Classification: McAfee (Grade 0-4), Brooker (Grade 1-4)
- Impact: May limit motion if severe (Grade 3-4), usually asymptomatic in Grade 1-2
- Prevention: NSAIDs postoperatively (indomethacin 75mg daily for 6 weeks), low-dose radiation (controversial)
- Management: Observation if asymptomatic; excision rarely indicated
Facet Degeneration:
- Progression of facet arthropathy despite motion preservation
- Suggests poor patient selection (unrecognized facet disease preoperatively)
- May require fusion if symptomatic
Implant Wear and Loosening:
- Polyethylene wear: Long-term concern (greater than 10 years)
- Osteolysis: Rare but reported with wear debris
- Subsidence: Progressive endplate failure (osteoporosis risk factor)
- Migration: Very rare with modern designs (keel and teeth fixation)
Core Dislocation (Charité-specific):
- Mobile core subluxation or dislocation (1-3%)
- Related to malposition at surgery (non-midline placement)
- May cause recurrent pain or clicking sensation
- Diagnosis: Lateral radiographs (core position assessment)
Adjacent Segment Disease:
- Despite theoretical benefit, ASD still occurs after TDR (lower rate than fusion in some studies)
- Radiographic ASD: 10-20% at 5 years
- Symptomatic ASD requiring surgery: 2-4% per year (similar to fusion)
Persistent/Recurrent Pain:
- Incidence: 10-30% (similar to fusion)
- Causes: Facetogenic pain (missed at selection), persistent discogenic pain, psychosocial factors
- Workup: Rule out implant-related issues (subsidence, malposition, HO)
- Management: Conservative care; fusion if TDR clearly failed
Revision Surgery
Indications:
- Implant malposition causing symptoms
- Progressive subsidence with instability
- Infection
- Intractable pain despite appropriate patient selection
Revision Options:
- Anterior revision TDR: Remove and replace implant (technically demanding)
- Anterior implant removal + fusion: Convert to ALIF with cage and screws
- Circumferential fusion: Add posterior instrumentation (most common)
Revision Challenges:
- Severe scar tissue from previous anterior approach
- Vascular adhesions to vertebral bodies
- Implant fixation (keels, teeth) makes removal difficult
- Higher complication rate than primary surgery (5-10% major complications)
Success Rate:
- Revision to fusion: 60-80% pain relief
- Revision TDR: Limited data (less predictable outcomes)
Outcomes and Evidence Base
FDA Investigational Device Exemption Trials
- 304 patients at 14 US centres, randomized 2:1: Charité TDR (n=205) vs anterior lumbar interbody fusion with BAK cage + iliac crest autograft (n=99)
- Single-level DDD L4-S1 unresponsive to non-operative care
- Clinical outcomes (VAS, ODI, SF-36) at least equivalent to ALIF; TDR recovered faster with lower disability scores at most intervals
- Patient satisfaction at 24 months: 73.7% (TDR) vs 53.1% (fusion), p=0.0011
- Reoperation rate lower with TDR: 5.4% vs 9.1%; hospital stay 1 day shorter
- Complication rate similar between groups
- Five-year data: 90 Charité and 43 BAK fusion patients (133 randomized completers)
- Overall success 57.8% (Charité) vs 51.2% (BAK) — non-inferiority maintained vs the 2-year result
- No statistically significant difference in ODI, VAS, or SF-36 between groups
- Index-level ROM preserved: 6.0° (Charité) vs 1.0° (fusion)
- Additional index-level surgery: 7.7% (Charité) vs 16.3% (fusion)
- Lower long-term disability (8.0% vs 20.9%) and higher full-time employment with TDR
- 286 patients treated on protocol, randomized 2:1: ProDisc-L vs circumferential (360°) fusion for 1-level DDD (L3-S1)
- 0% major device-related complications (safety endpoint)
- ODI improvement (at least 15%) in 77.2% (TDR) vs 64.8% (fusion)
- Neurological success superior with TDR: 91.2% vs 81.4% (p=0.0341)
- VAS pain and patient satisfaction significantly favoured TDR at 24 months
- Radiographic ROM maintained within normal range in 93.7%, averaging 7.7°
- 5-year radiographs: 123 ProDisc-L TDR vs 43 circumferential fusion patients (single-level DDD)
- Adjacent-level degeneration: 9.2% (TDR) vs 28.6% (fusion), p=0.004
- In patients without baseline adjacent disease: new ALD 6.7% (TDR) vs 23.8% (fusion), p=0.008 — fusion patients 3x more likely to develop ALD
- Adjacent-level surgery: 1.9% (TDR) vs 4.0% (fusion), not statistically significant (p=0.68)
- Index-level ROM maintained: 7.3° preop to 6.0° at 5 years
- 236 patients (161 TDR : 75 fusion), 81.8% follow-up at 5 years
- Composite study success: TDR non-inferior to fusion (12.5% margin, p=0.0099)
- Both groups maintained significant ODI improvement vs baseline (p less than 0.0001); VAS pain down ~48% in both
- Index-level secondary surgery: 8% (TDR) vs 12% (fusion)
- No TDR developed spontaneous fusion; segmental ROM stayed within normal range
- Would have surgery again: 82.5% (TDR) vs 68.0% (fusion)
- 7 RCTs (24-month follow-up) included; significant risk of bias from industry sponsorship and absence of blinding
- Six trials compared TDR with fusion: ODI improved 4.3 points more with TDR (5 studies; 95% CI 1.85-6.68)
- Back-pain VAS improved 5.2 mm more with TDR (2 studies; 95% CI 0.2-10.3)
- Both differences, though statistically significant, fell BELOW the predefined threshold for clinical relevance
- Prevention of adjacent-level disease and facet degeneration was not adequately assessed
- Evidence graded LOW quality (GRADE)
Long-Term Outcomes (Beyond 10 Years)
- 53 patients (63 Charité TDRs, types I-III) followed a mean of 17 years — the longest published lumbar TDR series
- Spontaneous ankylosis (auto-fusion) of the prosthesis occurred in 60%
- Reoperation required in 11%
- No adjacent-segment degeneration was seen in the 17% of implants that remained mobile, but these patients were significantly LESS satisfied than the auto-fused group
- No significant clinical difference between the three prosthesis generations
The Putzier series highlights that the long-term behaviour of a mobile-bearing prosthesis may converge on that of a fusion (auto-ankylosis), questioning whether the theoretical adjacent-segment benefit is realised in practice. Contemporary fixed-bearing devices (ProDisc-L) maintain measurable motion at 5 years, but comparable independent 15-20 year data remain scarce.
Comparison to Fusion Outcomes
TDR vs Fusion: Comparative Outcomes
| Outcome Measure | TDR (Average) | Fusion (Average) | Clinical Significance |
|---|---|---|---|
| Pain relief (VAS) | 4-5 cm improvement | 3-4 cm improvement | Similar magnitude |
| Function (ODI) | 20-25 point improvement | 18-22 point improvement | Similar magnitude |
| Motion preservation | 6-10° maintained | 0-2° (fused) | TDR preserves motion |
| Adjacent segment surgery 5yr | 2-4% | 4-8% | Lower with TDR |
| Overall reoperation 5yr | 5-8% | 8-12% | Lower with TDR |
| Heterotopic ossification | 5-15% clinically significant | N/A | TDR-specific complication |
| Retrograde ejaculation | 1-5% (L5-S1) | Rare with posterior | TDR higher (anterior approach) |
Predictors of Success
Positive Predictors:
- Age under 50 years
- Single-level disease
- Normal BMI (less than 30)
- No facet arthropathy
- No previous surgery
- Non-smoker
- No litigation/workers' compensation
- Realistic expectations
Negative Predictors:
- Multi-level disease
- Facet arthropathy (even mild)
- BMI over 35
- Active smoking
- Previous surgery at level
- Compensation/litigation
- Psychological comorbidities
Differential Diagnosis of the Pain Generator
Before offering TDR you must be confident the pain is discogenic and isolated. The commonest reason for TDR failure is an unrecognised or mislabelled pain generator. Use this table to triage the candidate who presents with chronic low back pain.
Distinguishing Causes of Chronic Axial Low Back Pain
| Pain Generator | Typical Features | Key Imaging / Test | Implication for TDR |
|---|---|---|---|
| Discogenic (DDD) | Central axial pain, worse with sitting/flexion, midline | Pfirrmann grade III-IV, HIZ on T2 MRI, concordant provocative discography | The ONLY indication — proceed if isolated |
| Facetogenic | Pain with extension/rotation, paraspinal tenderness, worse standing | Facet hypertrophy on CT/MRI; relief with medial branch block | Absolute contraindication — TDR does not treat it |
| Spondylolisthesis / instability | Mechanical pain, may have radicular features, start-up pain | Greater than 3mm translation or over 10° angulation on flexion-extension films | Contraindication — needs fusion |
| Spinal / foraminal stenosis | Neurogenic claudication, leg over back pain, relief with flexion | Central or lateral recess narrowing on MRI | Contraindication — needs decompression |
| Sacroiliac joint | Pain below L5, over the SIJ/buttock, FABER positive | SIJ provocation tests; diagnostic SIJ injection | Not addressed by TDR — exclude first |
| Non-organic / psychosocial | Non-anatomical pain, Waddell signs, yellow flags | Distress/risk screening; widespread pain | Predicts poor outcome — relative contraindication |
Controversies and Areas of Uncertainty
Does TDR actually prevent ASD?
The central selling point. RCT data (ProDisc-L 5-year) show radiographic adjacent-level degeneration is genuinely lower with TDR (9.2% vs 28.6%), yet adjacent-level reoperation rates are statistically similar to fusion. The radiographic benefit has not yet translated into a hard clinical endpoint. Verdict: plausible, not proven.
Auto-fusion of the prosthesis
Long-term Charité data show 60% spontaneous ankylosis at 17 years. If a motion-preserving device fuses itself, the rationale collapses. Heterotopic ossification (5-60% radiographically) is the driver. Whether modern fixed-bearing designs behave better over 15-20 years is unknown.
Is the clinical advantage real?
The Cochrane review found ODI and VAS differences favouring TDR that are statistically significant but below the threshold for clinical relevance, on low-quality, industry-sponsored evidence. NICE and several payers therefore do not endorse routine TDR.
Revision burden
Revising a TDR means a re-do anterior approach through scarred retroperitoneum and vascular adhesions, with major-complication rates of 5-10%. Many surgeons argue this future morbidity outweighs an unproven ASD benefit, favouring primary fusion in borderline cases.
Discography as a selection tool
Provocative discography is used to confirm a discogenic source, but it is invasive, operator-dependent, has false positives, and may itself accelerate disc degeneration. Reliance on it for TDR selection is contested; many centres prefer MRI HIZ/Modic changes plus clinical correlation.
Where does TDR sit today?
Use has declined globally as minimally invasive and lateral fusion techniques matured and long-term TDR concerns emerged. TDR survives as a niche option for the rare, strictly-selected young single-level discogenic patient — not a mainstream alternative to fusion.
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Ideal TDR Candidate Counseling
"A 42-year-old accountant presents with 18 months of chronic low back pain. MRI shows L5-S1 disc degeneration with high-intensity zone (HIZ) and maintained disc height. No facet arthropathy. Failed 8 months of physiotherapy and epidural injections. He asks about disc replacement after researching online. How do you counsel him?"
Scenario 2: Contraindication Recognition
"A 38-year-old woman with chronic low back pain is referred by her GP requesting disc replacement at L4-5. Her MRI shows disc degeneration at L4-5 with Grade 2 facet arthropathy (moderate facet joint degeneration). She had a microdiscectomy at L4-5 three years ago. How do you manage?"
Scenario 3: Intraoperative Vascular Injury
"You are performing an L4-5 disc replacement and mobilizing the left common iliac vein when you notice pulsatile bleeding from the vein. The access surgeon is not in the room but is in the hospital. How do you manage?"
Scenario 4: Revision TDR to Fusion
"A 48-year-old woman had L5-S1 ProDisc-L performed 3 years ago at an outside institution. She initially did well for 12 months but now has recurrent severe low back pain. Imaging shows the implant is well-positioned with no subsidence, but there is progressive Grade 3 facet arthropathy at L5-S1 and Grade 2 at L4-5. She has failed injections and medications. She asks what can be done. How do you manage?"
MCQ Practice Points
Contraindication Recognition
Q: Which of the following is an absolute contraindication to lumbar total disc replacement?
A) Age 55 years B) BMI 32 C) Fujiwara Grade 2 facet arthropathy D) Two-level disease (L4-5 and L5-S1) E) Non-union of previous wrist fracture
Answer: C) Fujiwara Grade 2 facet arthropathy
Explanation: Moderate to severe facet arthropathy (Grade 2 or higher) is an absolute contraindication to TDR because the facet joints are a pain generator that TDR does not address. Patients with facet disease have consistently poor outcomes with TDR. Age 55 is acceptable (under 60 preferred). BMI 32 is a relative contraindication but not absolute. Two-level disease is FDA-approved for some devices (Charité). Previous wrist fracture is irrelevant unless it indicates systemic bone disease.
Vascular Approach Anatomy
Q: During anterior approach to L4-5 for disc replacement, which structure must typically be mobilized to access the disc space?
A) Right common iliac artery B) Left common iliac vein C) Inferior vena cava D) Abdominal aorta E) Middle sacral artery
Answer: B) Left common iliac vein
Explanation: The left common iliac vein crosses anterior to the L4-5 disc space and must be mobilized cranially (superiorly) to access L4-5. This makes L4-5 approach more challenging and higher vascular risk than L5-S1, where access is between the bifurcation of the great vessels. The middle sacral artery is ligated at L5-S1, not L4-5. The IVC and aorta are more proximal (cephalad) and typically do not require mobilization.
Sympathetic Plexus Injury
Q: A 40-year-old male underwent L5-S1 disc replacement and reports inability to ejaculate 6 weeks postoperatively. What is the most likely cause?
A) Spinal cord injury B) Cauda equina syndrome C) Hypogastric plexus injury D) Pudendal nerve injury E) Psychological reaction to surgery
Answer: C) Hypogastric plexus injury
Explanation: Retrograde ejaculation from hypogastric (sympathetic) plexus injury occurs in 1-5% of L5-S1 TDR cases. The hypogastric plexus runs over the L5-S1 disc space anteriorly and can be stretched or injured during vessel mobilization. The patient has normal orgasm but dry ejaculation (semen goes into bladder instead of urethra). This is usually permanent. Spinal cord ends at L1-2 (not injured at L5-S1). Cauda equina would cause bowel/bladder/saddle numbness. Pudendal nerve injury would affect sensation and erection, not just ejaculation.
Implant Design Differences
Q: What is the primary biomechanical difference between Charité and ProDisc-L lumbar disc replacements?
A) Charité is cemented; ProDisc-L is uncemented B) Charité has mobile polyethylene core; ProDisc-L has fixed core C) Charité is metal-on-metal; ProDisc-L is metal-on-polyethylene D) Charité requires posterior instrumentation; ProDisc-L does not E) Charité is placed posteriorly; ProDisc-L is placed anteriorly
Answer: B) Charité has mobile polyethylene core; ProDisc-L has fixed core
Explanation: The Charité is a mobile-bearing design with a free-floating polyethylene core between two metal endplates (unconstrained). The ProDisc-L is a fixed-bearing design with the polyethylene inlay fixed to the inferior endplate and articulating with the superior endplate (semi-constrained, ball-and-socket). Both are uncemented (rely on teeth/keel fixation). Both are metal-on-polyethylene (not metal-on-metal). Both are placed via anterior approach. Neither requires posterior instrumentation.
Adjacent Segment Disease Theory
Q: What is the theoretical advantage of TDR over fusion regarding adjacent segment disease?
A) TDR decompresses adjacent neural elements B) TDR maintains motion, reducing stress transfer to adjacent levels C) TDR strengthens adjacent disc collagen D) TDR prevents facet degeneration at adjacent levels E) TDR increases disc height at adjacent levels
Answer: B) TDR maintains motion, reducing stress transfer to adjacent levels
Explanation: The biomechanical rationale for TDR is that fusion eliminates motion at the index level, transferring increased stress (intradiscal pressure up to 45% higher, altered kinematics) to adjacent segments, potentially accelerating degeneration. TDR preserves motion (5-15° per level), maintaining more physiologic load distribution and theoretically reducing adjacent segment stress. However, this benefit remains theoretical - while some studies show lower radiographic ASD rates with TDR, symptomatic ASD requiring surgery is similar between TDR and fusion in most long-term studies. TDR does not directly decompress, strengthen, or increase height at adjacent levels.
Guidelines, Registries & Global Practice
Global Epidemiology and Utilisation
- Chronic low back pain is the leading cause of years lived with disability worldwide; isolated single-level discogenic pain in a young patient is the narrow niche TDR targets.
- TDR represents a small minority of lumbar surgery globally. Uptake peaked in the late 2000s after the FDA approvals and has since declined in most high-income systems as fusion techniques matured and long-term motion-preservation data disappointed.
- Highest sustained use is in parts of continental Europe (where multiple devices hold CE marking); use is comparatively low in the UK, North America, and most of Asia.
Side-by-Side Guideline Positions
Major Society / Payer Positions on Lumbar TDR
| Body | Position | Practical Effect |
|---|---|---|
| FDA (US) | Charité (2004) and ProDisc-L (2006) approved for 1-level DDD L4-S1; ProDisc-L later 2-level | Available but with strict labelled indications |
| NICE (UK) | Procedure may be used with normal arrangements for consent/audit, but evidence on long-term efficacy is limited; not routinely funded | Rarely performed in the NHS; case-by-case |
| NASS (North American Spine Society) | Coverage recommendation supports TDR for carefully selected 1-level discogenic DDD that has failed conservative care | Used to justify insurer coverage in the US |
| EFORT / European practice | Recognised as an option in selected patients; emphasis on strict selection and surgeon experience | Continued use in specialist European centres |
| Cochrane / evidence reviews | At best equivalent to fusion short-term; advantages not clinically meaningful; long-term harm uncertain | Underpins cautious / restrictive funding |
All major bodies converge on one point: patient selection and surgeon experience are decisive, and TDR is never a substitute for fusion when instability, facet disease, stenosis, or deformity is present.
Registry Evidence
- Unlike hip and knee arthroplasty, lumbar TDR has no large dedicated international implant registry; long-term survivorship data therefore rest on the IDE trial cohorts and single-centre series (e.g. the 17-year Charité data above).
- The Swedish Spine Register (Swespine) and similar national spine registries capture some TDR cases and consistently show good short- to mid-term patient-reported outcomes but high heterogeneity, reinforcing the selection-dependent nature of results.
- The absence of arthroplasty-grade registry surveillance is itself a recognised gap and a reason for ongoing caution.
High- vs Limited-Resource Practice Variation
- Well-resourced specialist centres: access to an approach (vascular/access) surgeon, intraoperative fluoroscopy, a range of implant sizes/lordotic angles, and MRI/CT selection workup — the setting in which TDR outcomes are best.
- Limited-resource settings: device cost, lack of an access surgeon, and limited revision capacity make TDR impractical; instrumented fusion (TLIF/PLIF/ALIF) is the pragmatic and far more commonly available motion-segment treatment.
- Globally, fusion remains the default for surgical discogenic pain; TDR is reserved for the rare ideal candidate where the infrastructure to do it safely exists.
Antibiotic Prophylaxis (Implant Surgery — Global Principle)
- Single-dose IV cephalosporin (e.g. cefazolin) at induction; substitute a glycopeptide where MRSA colonisation or beta-lactam allergy applies — consistent with WHO and major national surgical-site-infection prevention guidance.
- Reported surgical-site infection rates are under 2% with appropriate prophylaxis; deep implant infection is managed along arthroplasty/prosthetic-infection lines.
LUMBAR DISC ARTHROPLASTY
Clinical summary
Indications (Must Meet ALL)
- •Single or two-level DDD at L4-5 or L5-S1 (FDA approved)
- •Discogenic pain confirmed (provocative discography or HIZ on MRI)
- •Failed conservative treatment minimum 6 months
- •Age typically under 60 years (young patient, long benefit)
- •Maintained disc height (at least 4-5mm for implant placement)
- •NO facet arthropathy (Grade 0-1 only, Grade 2+ excludes)
- •NO spondylolisthesis, stenosis, or previous surgery at level
Contraindications (FOSSILS)
- •Facet arthropathy (major pain generator not addressed)
- •Osteoporosis (T-score less than negative 1.5, subsidence risk)
- •Spondylolisthesis (greater than Grade I, instability)
- •Stenosis (spinal, needs decompression not motion)
- •Infection (active or previous at target level)
- •Levels more than 2 (multi-level disease not approved)
- •Surgery previous at level (scar tissue, altered anatomy)
Implant Designs
- •Mobile-bearing (Charité): 3-piece, unconstrained, free poly core
- •Fixed-bearing (ProDisc-L): 2-piece, semi-constrained, ball-and-socket
- •Metal-on-metal (Maverick): No polyethylene, metallosis concerns
- •All use teeth/keel fixation (no cement), anterior approach only
Surgical Approach (ACCESS)
- •Anterior midline incision (infraumbilical for L5-S1, extended L4-5)
- •Clear peritoneum laterally (retroperitoneal dissection)
- •Control vessels: L5-S1 between bifurcation; L4-5 mobilize left iliac vein
- •Expose disc space (ligate middle sacral vessels at L5-S1)
- •Sympathetic plexus preserve (hypogastric, retrograde ejaculation risk)
- •Secure implant (midline positioning critical, especially Charité)
Complications
- •Vascular injury 1-3% (iliac vessels, higher at L4-5)
- •Retrograde ejaculation 1-5% at L5-S1 (hypogastric plexus injury)
- •Heterotopic ossification 5-15% clinically significant (may limit motion)
- •Subsidence (early: osteoporosis; late: endplate failure)
- •Implant malposition (check intraop fluoro, reposition if needed)
- •Revision difficult (scar, vascular adhesions, implant removal challenging)
Evidence and Outcomes
- •FDA IDE trials: Non-inferior to fusion at 2, 5, 10 years
- •Motion preservation: 5-15° per level (average 7-10° long-term)
- •Adjacent segment surgery: Lower rate than fusion (2-4% vs 4-8% at 5yr)
- •Overall success: 70-80% in selected patients (patient selection critical)
- •Reoperation rate: 5-8% at 5 years (lower than fusion 8-12%)
Exam Pearls
- •Ideal candidate: Young (under 60), single-level L4-5/L5-S1, no facet disease
- •Never offer TDR if facet arthropathy (absolute contraindication)
- •L4-5 approach harder than L5-S1 (left iliac vein mobilization)
- •Counsel males about retrograde ejaculation risk before L5-S1 TDR
- •Non-inferior to fusion but different complication profile
- •Strict patient selection = key to success (expanding criteria = poor outcomes)