White and Panjabi | Dynamic Imaging | Fusion Decisions
- White & Panjabi: loss of ability to maintain normal motion pattern
- Radiographic: greater than 4mm translation OR greater than 10-15° angular motion
- Clinical diagnosis supported by imaging, not purely radiographic
- Bilateral greater than 50% facetectomy OR complete unilateral = iatrogenic instability
- Add fusion if extensive decompression creates instability
- “Instability is CLINICAL with radiographic support
- “Flexion-extension films must be standing/weight-bearing
- “Degenerative cascade: dysfunction → instability → restabilization
- “Three-column theory: 2+ columns = unstable
Loss of ability to maintain normal motion pattern under physiologic loads without neurological deficit, major deformity, or incapacitating pain.
Flexion-extension films. Greater than 4mm translation OR greater than 10-15° angular motion at single segment indicates instability.
Facetectomy threshold. Bilateral greater than 50% OR complete unilateral facetectomy significantly increases instability risk. Add fusion!
Clinical diagnosis. Imaging supports but doesn't define instability. Symptoms and function guide treatment decisions.
- Clinical Instability
- Symptomatic motion disorder
- Radiographic Instability
- Excessive motion on imaging
- Clinical Instability
- History, exam, function
- Radiographic Instability
- Flexion-extension X-rays
- Clinical Instability
- Pain with movement
- Radiographic Instability
- Greater than 4mm or greater than 10-15°
- Clinical Instability
- Failed conservative care
- Radiographic Instability
- If symptomatic
- Clinical Instability
- Clinical diagnosis primary
- Radiographic Instability
- Supports clinical diagnosis
PANJABIWhite and Panjabi Instability Criteria
Hook:Remember PANJABI for the stability expert's criteria!
AMPThree-Column Theory (Denis)
Hook:AMP up your spine stability knowledge - 2+ columns = unstable!
PANPanjabi's Three Subsystems
Hook:PAN-jabi's three subsystems for spinal stability!
DIRDegenerative Cascade Phases
Hook:DIR-ect path of degenerative cascade from dysfunction to restabilization!
Overview and Epidemiology
White and Panjabi's definition is exam gold. Instability = loss of spine's ability to maintain normal motion pattern under physiologic loads without neurological deficit, major deformity, or incapacitating pain. This is CLINICAL!
Epidemiology Key Points
- Exact prevalence uncertain due to diagnostic variability
- Estimated 10-25% of chronic low back pain cases have instability component
- Increases with age due to degenerative cascade progression
- Age: Degenerative instability peaks at 40-65 years
- Gender: Female 2:1 higher incidence (ligamentous laxity, hormonal factors)
- Occupation: Heavy manual labor increases risk
- Genetics: Familial clustering observed in degenerative spine disease
- L4-L5 most commonly affected (50-60% of cases)
- L5-S1 second most common (20-30%)
- Multilevel involvement in approximately 20%
- Upper lumbar levels less common but occur with trauma or iatrogenic causes
- Significant contributor to chronic disability and lost work days
- Fusion surgery for degenerative instability among most common spine procedures
- Substantial economic burden from conservative and surgical care
Pathophysiology and Mechanisms
Spinal Stability Biomechanics
- Anterior column: ALL, anterior VB and disc (compression loads)
- Middle column: PLL, posterior VB and disc (critical for stability)
- Posterior column: Pedicles, facets, lamina, ligaments (tension and rotation)
Injury to TWO or more columns indicates mechanical instability requiring stabilization.
- Resist 20% of axial load in neutral position
- Resist 40-50% in extension
- Greater than 50% bilateral facetectomy significantly increases flexion-extension motion
- Complete unilateral facetectomy increases axial rotation and lateral bending
- Intact annulus provides torsional stiffness
- Discectomy reduces torsional stiffness by approximately 30%
- Large annular defects increase instability risk
Understanding biomechanics guides surgical decision-making about fusion necessity.
Surgical decompression can CREATE instability. Bilateral facetectomy greater than 50% OR complete unilateral facetectomy significantly increases risk. If extensive decompression needed, plan for fusion to prevent postoperative instability and progressive deformity.
The body explains Panjabi's three subsystems, but the concept examiners most want to hear - the neutral zone (NZ) - is only buried in an evidence card. Know it explicitly:
- Definition: within a segment's total range of motion, the NZ is the inner region around the neutral posture where there is minimal resistance to motion (the "slack" of the segment), bounded by the elastic zone where ligamentous/disc resistance rapidly rises.
- Why it matters more than range of motion: Panjabi showed the NZ is a more sensitive marker of instability than total ROM. Degeneration (annular tears, facet/capsular laxity) enlarges the neutral zone - the segment becomes "loose" around neutral even when end-range ROM looks normal, which is why standard flexion-extension thresholds can miss early clinical instability.
- How treatments work through the NZ: anything that reduces an enlarged neutral zone reduces pain - osteophytes/restabilisation in the degenerative cascade, fusion (abolishes the NZ surgically), and crucially active muscle activation (multifidus/transversus abdominis). This is the biomechanical reason core-stabilisation physiotherapy works: it shrinks the NZ via the active subsystem without surgery.
Exam point: define the neutral zone as the low-resistance region around neutral; state that an enlarged NZ is the most sensitive marker of instability (more than ROM); and explain that fusion, osteophytes and muscle activation all relieve pain by reducing it - tying the cascade, conservative care and fusion together.
Classification Systems
Classification by Etiology
- Mechanism
- Disc and facet degeneration
- Typical Age
- 40-65 years
- Key Features
- Most common, L4-L5
- Mechanism
- Pars defect with spondylolisthesis
- Typical Age
- 15-35 years
- Key Features
- Athletes, L5-S1
- Mechanism
- Post-laminectomy, facetectomy
- Typical Age
- Post-surgery
- Key Features
- Excessive bone removal
- Mechanism
- Fracture-dislocation
- Typical Age
- Any age
- Key Features
- Three-column injury
- Mechanism
- Tumor, infection
- Typical Age
- Any age
- Key Features
- Bone destruction
Etiological classification guides treatment approach and prognosis.
Clinical Assessment
- Instability catch: Sharp pain with movement transitions
- Giving way sensation: Back feels unstable
- Positional relief: Better sitting than standing
- Activity limitation: Avoids bending, twisting
- Hand support: Needs to support back with hands
- Mechanical pattern: Worse with activity
- Positional: Worse prolonged standing
- Relief: Better with sitting or lying
- Morning stiffness: After inactivity
- No night pain: Unless severe degeneration
Physical Examination
- Loss of lumbar lordosis (muscle spasm)
- Forward-flexed posture
- Palpable step-off if spondylolisthesis
- Asymmetric paraspinal muscle bulk
- Paraspinal muscle spasm
- Midline tenderness over affected level
- Step-off palpable in spondylolisthesis
- Guarded movements
- Limited flexion and extension
- Instability catch during flexion-to-extension transition
- Often NORMAL in pure mechanical instability
- May have radiculopathy if associated stenosis or foraminal narrowing
- Lower extremity strength, sensation, reflexes
Special Tests
- Technique
- Flex then extend spine
- Positive Finding
- Sharp catch pain during transition
- Technique
- Prone, legs off table, press spinous process
- Positive Finding
- Pain relieved with leg lift
- Technique
- Prone, PA pressure on spinous process
- Positive Finding
- Excessive motion or pain
- Technique
- Forward bend while palpating
- Positive Finding
- Excessive segmental motion felt
High specificity for lumbar instability. Patient prone with legs off table. Examiner applies PA pressure to spinous process - pain indicates instability. Patient lifts legs (activates paraspinals) - pain relief with muscle activation confirms dynamic instability. Positive likelihood ratio approximately 4.0.
Differential Diagnosis
- Pain pattern
- Mechanical, worse with activity/transition, relief with sitting
- Discriminating feature
- Instability catch, giving-way; positive prone instability test
- Key test
- Standing flexion-extension radiographs (greater than 4mm / greater than 10-15°)
- Pain pattern
- Neurogenic claudication, worse standing/walking, relief with flexion
- Discriminating feature
- Symptoms positional and neurogenic, not motion-triggered
- Key test
- MRI showing canal/lateral recess stenosis
- Pain pattern
- Axial pain worse with flexion/sitting
- Discriminating feature
- Provoked by sustained flexion, not by motion transition
- Key test
- MRI HIZ/Modic changes; no abnormal dynamic motion
- Pain pattern
- Axial pain worse with extension/rotation
- Discriminating feature
- Relief with medial branch block
- Key test
- Diagnostic facet/medial branch block (greater than 50% relief)
- Pain pattern
- Mechanical back pain ± radiculopathy in young athlete
- Discriminating feature
- Pars defect; step-off; commonest L5-S1
- Key test
- Oblique radiograph / CT pars; lateral standing film
- Pain pattern
- Buttock pain below L5, often unilateral
- Discriminating feature
- Provocation cluster positive; pain over PSIS
- Key test
- SIJ provocation tests / image-guided block
Investigations
Plain Radiographs - KEY Investigation
- MUST be weight-bearing (supine misses instability)
- Assess disc height, alignment, osteophytes
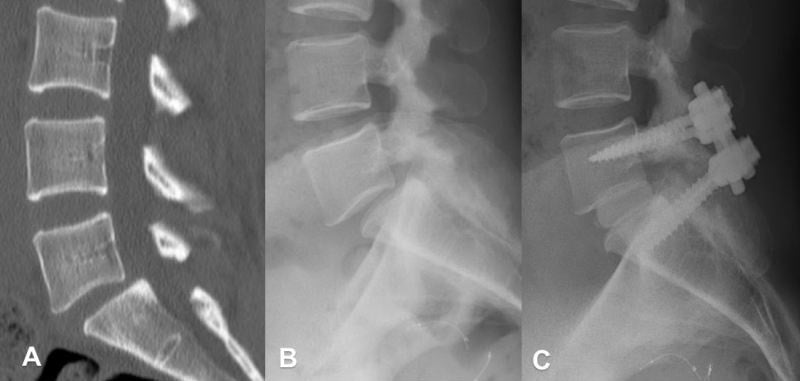
- Measure slip if spondylolisthesis present
- GOLD STANDARD for diagnosing instability
- Patient performs maximal safe flexion and extension
- Measure translation and angular motion
- Translation: greater than 4mm sagittal plane shift
- Angular: greater than 10-15 degrees segmental motion
- Traction spur: horizontal osteophyte indicates chronic instability
- Translation: measure posterior body offset between adjacent vertebrae
- Angular: measure change in segmental Cobb angle from flexion to extension
- Use same anatomic landmarks on both views
Dynamic radiographs essential - static films miss functional instability.
Imaging Atlas - Diagnostic Assessment
Management Algorithm
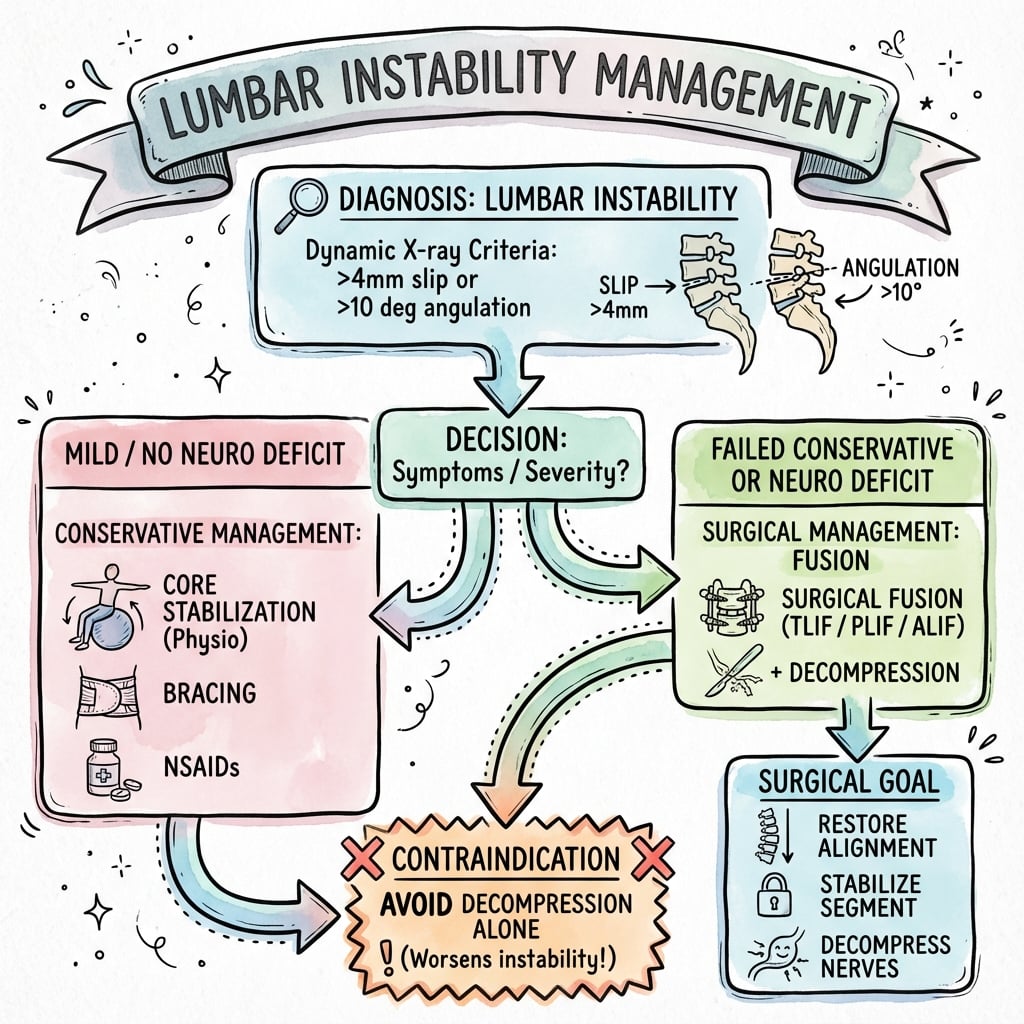
Non-Operative Management - First Line
- Mild to moderate symptoms
- No progressive deformity
- No neurological deficit
- Patient preference
- Medical comorbidities precluding surgery
- Target transversus abdominis and multifidus
- Proprioceptive training
- Postural education
- Goal: enhance active subsystem compensation
- 6-12 weeks structured program
- Most important non-surgical intervention
- Avoid repetitive bending and twisting
- Proper lifting mechanics
- Ergonomic workplace assessment
- Weight loss if obese
- Short-term use for acute flares (2-4 weeks maximum)
- Lumbosacral corset provides external support
- Prolonged use causes muscle deconditioning
- Wean as core strength improves
- NSAIDs for inflammation and pain
- Muscle relaxants for spasm (short-term)
- Neuropathic agents if radicular component
- Avoid opioids for chronic mechanical pain
- Epidural steroid injections if radicular symptoms
- Facet joint injections (diagnostic and therapeutic)
- Medial branch blocks
- Radiofrequency ablation for facet-mediated pain
- Approximately 30-40% adequate improvement with conservative care
- Better outcomes with structured physiotherapy program
- Predictors of success: mild symptoms, good compliance, no significant deformity
Minimum 6 months conservative trial before considering surgery (unless progressive neurology).
Smoking significantly increases pseudarthrosis risk. Nicotine impairs bone healing and fusion rates. Non-smokers: 90-95% fusion. Smokers: 70-80% fusion. Strongly encourage smoking cessation minimum 4 weeks pre-op and throughout healing. Consider bone morphogenetic protein (BMP) in smokers.
The complications section warns about flatback and sagittal imbalance, but the parameters that prevent them - now core exam material - are not stated. Plan fusion against the spinopelvic numbers, not just the unstable segment:
- Pelvic incidence (PI) is a fixed, morphological pelvic parameter (PI = pelvic tilt + sacral slope). It sets how much lumbar lordosis (LL) the patient needs.
- The PI-LL mismatch is the key target: aim for lumbar lordosis within roughly 10 degrees of the pelvic incidence (PI minus LL of about 10 degrees or less). Fusing the lumbar spine in relative hypolordosis (a large PI-LL mismatch) forces compensatory pelvic retroversion (high pelvic tilt) and increases the sagittal vertical axis (SVA) - producing the stooped, fatiguing flatback posture.
- Why it matters for instability surgery: a malaligned fusion not only causes flatback and poor function but accelerates adjacent-segment breakdown, because the unfused levels overwork to keep the eyes level. So even a "good" single-level construct can fail if it locks in hypolordosis.
Exam point: before fusing, measure PI, PT, SS, LL and SVA, restore lumbar lordosis to match the pelvic incidence (minimise PI-LL mismatch) and keep the SVA balanced - "fuse in lordosis" - to avoid iatrogenic flatback and accelerated adjacent-segment failure.
Complications
Early Complications (under 6 weeks)
- Dural tear (5-10%): Primary repair, bed rest, avoid Valsalva
- Neural injury (1-2%): Nerve root or cauda equina from retraction or instrumentation
- Vascular injury (under 1%): Aorta, vena cava, iliac vessels (ALIF higher risk)
- Excessive bleeding: Epidural venous plexus, bone bleeding
- Wound infection (2-5%): Superficial or deep, higher with multilevel, obesity
- Hematoma: Epidural or wound, may cause neurological compression
- CSF leak: From unrecognized or inadequately repaired dural tear
- Medical: DVT/PE, MI, pneumonia, UTI
- Meticulous hemostasis
- Prophylactic antibiotics
- DVT prophylaxis
- Careful retraction and neural handling
Early recognition and management critical for optimal outcomes.
Guidelines, Registries & Global Practice
Global Epidemiology
Lumbar instability is most often a manifestation of degenerative disc and facet disease, the leading structural driver of low back pain (LBP). According to PubMed, a systematic review of 165 studies from 54 countries estimated the global mean point prevalence of LBP at approximately 11.9% and the 1-month prevalence at approximately 23.2%, with the highest burden in women and those aged 40-80 years (Hoy et al. 2012, DOI). LBP is consistently ranked the single leading cause of years lived with disability worldwide, and the absolute number affected is rising with population ageing.
- Most affected segment: L4-L5 (degenerative spondylolisthesis), then L5-S1
- Sex: Degenerative spondylolisthesis is markedly more common in women
- Trend: Lumbar fusion volumes have risen faster than decompression in high-income systems, without a fall in reoperation rates (Martin et al. 2007, DOI)
Guideline & Society Positions
- Position on fusion for instability
- Do NOT offer fusion for non-specific LBP outside a trial; reserve for deformity/instability with clear indication
- Evidence basis
- RCT-informed, conservative
- Position on fusion for instability
- Decompression PLUS fusion supported for symptomatic degenerative spondylolisthesis with instability
- Evidence basis
- Level I/II (SPORT, Herkowitz, Fischgrund)
- Position on fusion for instability
- MDT assessment; fusion for documented instability or iatrogenic destabilisation after wide decompression
- Evidence basis
- Consensus + RCT
- Position on fusion for instability
- Reserve fusion for true instability, deformity, or post-decompression destabilisation; favour selective single-level constructs
- Evidence basis
- Consensus + biomechanical
Registry & Trial Evidence
- SPORT (NEJM 2007): as-treated benefit of surgery over non-operative care for degenerative spondylolisthesis at 2 years (Weinstein et al., DOI).
- Fischgrund 1997 Volvo Award: instrumentation raised fusion rate (82% vs 45%) without improving 2-year clinical outcome (DOI) — a recurring theme in registry analyses.
- National spine registries (e.g. Swespine, the British Spine Registry, and the Norwegian/Danish spine registries) collect PROMs (Oswestry Disability Index, EQ-5D) to benchmark fusion outcomes; routine reporting of reoperation and adjacent-segment surgery is now standard.
Practice Variation
Marked international and intra-national variation exists in fusion rates for degenerative lumbar disease, driven by reimbursement, surgeon training, and differing thresholds for diagnosing "instability." Conservative-first pathways (physiotherapy-led core stabilisation, activity modification, judicious injections) are universally endorsed before elective fusion, except for progressive neurological deficit, cauda equina syndrome, or progressive deformity. Minimally invasive and navigation/robotic-assisted fusion techniques (TLIF/PLIF) are increasingly available at tertiary centres internationally, and structured multidisciplinary post-operative rehabilitation, including occupational therapy and vocational return-to-work coordination, supports recovery and reintegration.
MCQ Practice Points
Q: What radiographic findings on flexion-extension X-rays define lumbar instability? A: Translation greater than 4mm (or greater than 10% of vertebral body width) OR angular motion greater than 10-15 degrees between adjacent segments. These are the classic White-Panjabi criteria for clinical instability.
Q: How much facet resection causes iatrogenic instability requiring fusion? A: Greater than 50% bilateral facetectomy or complete unilateral facetectomy. The facet joints contribute 40-50% of torsional stability. Partial medial facetectomy (less than 50% per side) typically preserves stability.
Q: What is the difference between clinical and mechanical instability? A: Clinical instability produces symptoms (pain, neurological signs) with motion; mechanical instability is radiographic abnormal motion that may be asymptomatic. Surgical fusion addresses mechanical instability but is only indicated when clinically symptomatic.
Q: When should fusion be added to decompression for degenerative conditions? A: When pre-existing instability exists (greater than 4mm translation), when decompression creates iatrogenic instability (extensive facetectomy), or when deformity correction is required. SPORT trial showed no benefit of routine fusion for stable stenosis.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 58-year-old woman underwent L4-L5 laminectomy for stenosis 18 months ago with initial good relief of leg symptoms. She now presents with mechanical back pain worse with activity. Flexion-extension X-rays show 6mm translation at L4-L5. How would you manage this?”
“You are planning L4-L5 decompression for severe central and lateral recess stenosis. Pre-operative flexion-extension films show no instability. Intraoperatively, you find you need bilateral 60% facetectomy to adequately decompress. What do you do?”
“A 52-year-old manual laborer has chronic mechanical low back pain worse with activity. MRI shows severe L4-L5 disc degeneration with facet arthropathy. Flexion-extension films show 3mm translation and 8 degrees angular motion - below instability thresholds. He has failed 12 months of physiotherapy. Does he have instability? Would you offer surgery?”
Key Definitions
- White & Panjabi: Loss of spine's ability to maintain normal motion pattern under physiologic loads without neurological deficit, major deformity, or incapacitating pain
- Clinical instability: CLINICAL diagnosis supported by imaging, not purely radiographic
- Radiographic thresholds: Greater than 4mm translation OR greater than 10-15° angular motion on flexion-extension films
- Panjabi subsystems: Passive (osteoligamentous), Active (muscular), Neural (proprioceptive control)
Classification
- Etiological: Degenerative (most common), isthmic (pars defect), iatrogenic (post-laminectomy), traumatic, pathological
- Three columns (Denis): Anterior (ALL, anterior VB/disc), Middle (PLL, posterior VB/disc - KEY), Posterior (facets, ligaments)
- Degenerative cascade: Dysfunction (15-45y) → Instability (35-70y) → Restabilization (60+y)
- Instability rule: Injury to 2 or more columns = mechanical instability
Clinical Assessment
- History: Mechanical back pain worse with activity, instability catch, giving way sensation, relief with sitting
- Prone instability test: PA pressure on spinous process causes pain, relieved with leg lift (muscle activation)
- Flexion-extension radiographs: GOLD STANDARD - must be weight-bearing
- MRI findings: Disc degeneration, facet effusion, Modic Type II changes, high-intensity zone in annulus
Surgical Indications
- Failed conservative management minimum 6 months (unless progressive neurology)
- Documented instability on imaging with symptom correlation
- Iatrogenic: Bilateral greater than 50% facetectomy OR complete unilateral facetectomy
- Progressive deformity with functional impairment
- Add fusion to decompression if creating instability
Surgical Techniques
- Posterolateral fusion with instrumentation: Gold standard, 85-95% fusion rate
- TLIF: Unilateral approach, less neural retraction, excellent foraminal decompression
- PLIF: Bilateral approach, direct neural decompression, higher dural tear risk
- ALIF: Anterior approach, large graft area, useful for spondylolisthesis reduction
Complications
- Pseudarthrosis: 5-10% instrumented PLF. Risk factors: smoking, obesity, multilevel, diabetes
- Adjacent segment disease: 2-3% per year, 15-20% require surgery at 10 years
- Dural tear: 5-10%. Management: primary repair, bed rest, avoid Valsalva
- Smoking increases pseudarthrosis risk: 90-95% fusion non-smokers vs 70-80% smokers
Evidence Pearls
- White & Panjabi (1990): Foundation definition and radiographic thresholds
- Panjabi three subsystem model: Explains variable clinical presentation
- Abumi facetectomy study: Bilateral greater than 50% = significant motion increase
- Kirkaldy-Willis cascade: Dysfunction → Instability → Restabilization phases
- Conservative success 30-40%, surgical 70-80% good/excellent outcomes
Evidence Base
Panjabi: Clinical Spinal Instability and Low Back Pain
- Clinical instability defined as loss of the normal pattern of spinal motion causing pain and/or neurological dysfunction
- Stabilising system comprises three subsystems: spinal column, spinal muscles, and the neural control unit
- The neutral zone is a more sensitive parameter than range of motion for detecting destabilisation and restabilisation
- Reduction of an enlarged neutral zone (by fusion, osteophytes, or muscle activation) correlates with pain relief
Panjabi Three Subsystem Model
- Described spinal stability as interaction of passive (osteoligamentous), active (muscular), and neural control subsystems
- Explained how dysfunction of any subsystem can be compensated, adapted to, or lead to injury and clinical instability
- Provided framework for understanding why structural findings do not always correlate with symptoms
- Supported role of rehabilitation targeting the active and neural subsystems
Kirkaldy-Willis Degenerative Cascade
- Described three phases: dysfunction, instability, and restabilisation
- Instability phase characterised by abnormal motion and mechanical pain
- Restabilisation phase shows decreased motion but stenosis develops
- Natural history shows transition from mechanical to neurogenic symptoms
Abumi: Graded Facetectomies and Lumbar Stability
- In vitro study of fresh human functional spinal units under six load modes (range of motion and neutral zone measured)
- Medial facetectomy (partial) and division of supraspinous/interspinous ligaments did NOT significantly affect stability
- Total facetectomy, even when created unilaterally, rendered the lumbar segment unstable (increased flexion and axial rotation)
- Provides the biomechanical basis for preserving at least the lateral facet and for adding fusion when total facetectomy is required
Martin: Reoperation Rates After Lumbar Surgery
- Washington State discharge registry; adults having lumbar surgery for degenerative disease in 1990-1993 (n=24,882)
- Cumulative incidence of reoperation was 19% over the subsequent 11 years
- For spondylolisthesis, reoperation was LESS likely after fusion than after decompression alone (17.1% vs 28.0%, P=0.002)
- For other degenerative diagnoses, reoperation was HIGHER after fusion than decompression alone (21.5% vs 18.8%, P=0.008); 62.5% of post-fusion reoperations involved device complication or pseudarthrosis
Herkowitz & Kurz: Decompression vs Decompression + Arthrodesis
- 50 patients with spinal stenosis and degenerative spondylolisthesis prospectively studied (mean follow-up 3 years)
- Concomitant intertransverse-process arthrodesis gave significantly better relief of back and leg pain than decompression alone
- Established that an unstable spondylolisthetic segment should be fused at the time of decompression
- Landmark evidence behind fusing the listhetic level during decompression
Fischgrund (1997 Volvo Award): Instrumentation and Fusion
- 76 patients randomised to instrumented versus non-instrumented posterolateral fusion after decompression
- Successful arthrodesis: 82% instrumented vs 45% non-instrumented (P=0.0015)
- Clinical outcome excellent/good in 76% instrumented vs 85% non-instrumented (P=0.45, not significant)
- Pedicle-screw instrumentation improves fusion rate but did not improve 2-year clinical pain outcome
SPORT: Surgical vs Nonsurgical for Degenerative Spondylolisthesis
- 607 patients across 13 US centres (randomised + observational cohorts); high crossover (~40% each way) in the randomised arm
- As-treated analysis showed a significant advantage for surgery at 2 years: bodily pain effect 18.1, physical function 18.3, Oswestry -16.7
- Surgically treated patients had substantially greater improvement in pain and function than nonsurgical care over 2 years
- Little evidence of harm from either treatment
References
- White AA, Panjabi MM. Clinical Biomechanics of the Spine. 2nd ed. Philadelphia: Lippincott; 1990.
- Panjabi MM. The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement. J Spinal Disord. 1992;5(4):383-389.
- Kang CH, Shin MJ, Kim SM, Lee SH, Lee CS. MRI of paraspinal muscles in lumbar degenerative kyphosis patients and control patients with chronic low back pain. Clin Radiol. 2007;62(5):479-486.
- Kirkaldy-Willis WH, Farfan HF. Instability of the lumbar spine. Clin Orthop Relat Res. 1982;(165):110-123.
- Kalichman L, Li L, Kim DH, et al. Facet joint osteoarthritis and low back pain in the community-based population. Spine. 2008;33(23):2560-2565.
- Battié MC, Videman T, Parent E. Lumbar disc degeneration: epidemiology and genetic influences. Spine. 2004;29(23):2679-2690.
- Sengupta DK, Herkowitz HN. Degenerative spondylolisthesis: review of current trends and controversies. Spine. 2005;30(6 Suppl):S71-81.
- Martin BI, Deyo RA, Mirza SK, et al. Expenditures and health status among adults with back and neck problems. JAMA. 2008;299(6):656-664.
- Adams MA, Roughley PJ. What is intervertebral disc degeneration, and what causes it? Spine. 2006;31(18):2151-2161.
- Fujiwara A, Lim TH, An HS, et al. The effect of disc degeneration and facet joint osteoarthritis on the segmental flexibility of the lumbar spine. Spine. 2000;25(23):3036-3044.
- Ghiselli G, Wang JC, Bhatia NN, Hsu WK, Dawson EG. Adjacent segment degeneration in the lumbar spine. J Bone Joint Surg Am. 2004;86(7):1497-1503.
- Abumi K, Panjabi MM, Kramer KM, Duranceau J, Oxland T, Goel VK. Biomechanical evaluation of lumbar spinal stability after graded facetectomies. Spine. 1990;15(11):1142-1147.
- Denis F. The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine. 1983;8(8):817-831.
- Kim DH, Vaccaro AR, Berta SC. Spinal Instrumentation: Surgical Techniques. New York: Thieme; 2005.
- Meyerding HW. Spondylolisthesis. Surg Gynecol Obstet. 1932;54:371-377.
- Kalichman L, Kim DH, Li L, Guermazi A, Hunter DJ. Computed tomography-evaluated features of spinal degeneration: prevalence, intercorrelation, and association with self-reported low back pain. Spine J. 2010;10(3):200-208.
- Panjabi MM. Clinical spinal instability and low back pain. J Electromyogr Kinesiol. 2003;13(4):371-379.
- Pearcy MJ, Tibrewal SB. Lumbar intervertebral disc and ligament deformations measured in vivo. Clin Orthop Relat Res. 1984;(191):281-286.
- Nachemson AL. Newest knowledge of low back pain. A critical look. Clin Orthop Relat Res. 1992;(279):8-20.
- Frymoyer JW, Selby DK. Segmental instability. Rationale for treatment. Spine. 1985;10(3):280-286.
- Hides JA, Richardson CA, Jull GA. Multifidus muscle recovery is not automatic after resolution of acute, first-episode low back pain. Spine. 1996;21(23):2763-2769.
- MacDonald D, Moseley GL, Hodges PW. Why do some patients keep hurting their back? Evidence of ongoing back muscle dysfunction during remission from recurrent back pain. Pain. 2009;142(3):183-188.
- O'Sullivan PB, Twomey LT, Allison GT. Evaluation of specific stabilizing exercise in the treatment of chronic low back pain with radiologic diagnosis of spondylolysis or spondylolisthesis. Spine. 1997;22(24):2959-2967.
- Weinstein JN, Lurie JD, Tosteson TD, et al. Surgical versus nonsurgical treatment for lumbar degenerative spondylolisthesis. N Engl J Med. 2007;356(22):2257-2270.
- Herkowitz HN, Kurz LT. Degenerative lumbar spondylolisthesis with spinal stenosis. A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am. 1991;73(6):802-808.
- Martin BI, Mirza SK, Comstock BA, Gray DT, Kreuter W, Deyo RA. Reoperation rates following lumbar spine surgery and the influence of spinal fusion procedures. Spine. 2007;32(3):382-387.