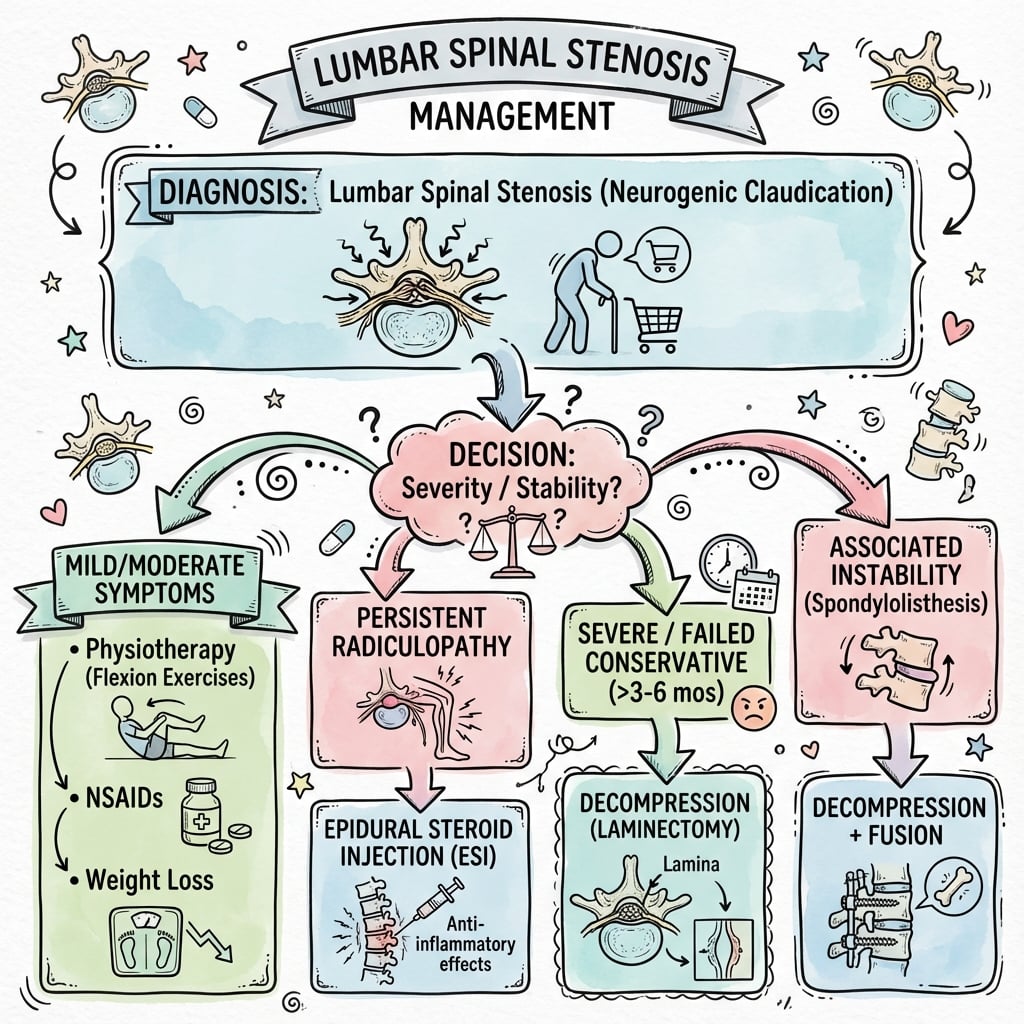
Canal narrowing causing leg symptoms with walking - relieved by flexion (shopping cart sign)
- Neurogenic vs vascular claudication: neurogenic relieved by FLEXION, vascular by stopping
- Shopping cart sign: patient prefers flexed position (opens canal)
- Absolute stenosis: less than 10mm AP diameter, relative: 10-12mm
- SPORT trial: surgery superior at 2-4 years for symptomatic stenosis
- Add fusion if instability or spondylolisthesis present
- “Often normal neurological examination at rest - symptoms reproduced with walking
- “Wide-based gait and forward-flexed posture are classic
- “L4-5 most commonly affected level followed by L3-4
- “MRI is gold standard - CT myelogram if MRI contraindicated
Lumbar Spinal Stenosis
The key clinical distinction is NEUROGENIC vs VASCULAR claudication! Neurogenic: leg symptoms with walking, relieved by FLEXION (shopping cart sign). Vascular: calf pain, relieved by stopping (not necessarily flexing). Examiners love this distinction!
Overview and Epidemiology
Lumbar spinal stenosis (LSS) is one of the most common causes of low back and leg symptoms in older adults. It represents progressive narrowing of the spinal canal leading to compression of neural elements.
Epidemiology
Prevalence and Demographics
- Value
- 20-30% in population over 60 (imaging)
- Value
- 5-10% of those with imaging stenosis
- Value
- 60-70 years
- Value
- Equal or slight male predominance
- Value
- Number one reason for spine surgery in patients over 65
Most Affected Levels
- L4-5: Most commonly affected (80%)
- L3-4: Second most common
- Multi-level: Common in advanced disease
- L5-S1: Less common (protected by iliolumbar ligament)
Pathophysiology
Canal Anatomy
Normal Dimensions
- Normal Value
- 15-18mm
- Stenosis Threshold
- Under 11mm (absolute)
- Normal Value
- 20-25mm
- Stenosis Threshold
- Under 15mm
- Normal Value
- 200-400mm2
- Stenosis Threshold
- Under 100mm2 (severe)
- Normal Value
- 5-7mm
- Stenosis Threshold
- Under 3mm (stenosis)
- Normal Value
- 20-23mm
- Stenosis Threshold
- Under 15mm
Stenosis Types
- Location
- Spinal canal
- Structures Affected
- Cauda equina
- Clinical Pattern
- Bilateral claudication
- Location
- Between pedicle and facet
- Structures Affected
- Traversing root
- Clinical Pattern
- Radiculopathy pattern
- Location
- Neural foramen
- Structures Affected
- Exiting root
- Clinical Pattern
- Radiculopathy pattern
- Location
- Beyond foramen
- Structures Affected
- Exiting root
- Clinical Pattern
- Often missed on imaging
Pathophysiology
Contributing Factors to Stenosis
- Contribution
- Anterior narrowing
- Mechanism
- Bulging, height loss
- Contribution
- Posterolateral narrowing
- Mechanism
- Hypertrophy, arthrosis
- Contribution
- Posterior narrowing
- Mechanism
- Hypertrophy, infolding
- Contribution
- Lateral narrowing
- Mechanism
- Congenital short pedicle
- Contribution
- Dynamic narrowing
- Mechanism
- Forward translation
Pathophysiology of Symptoms
- Effect
- Direct neural compression
- Effect
- Impaired venous drainage, edema
- Effect
- Reduced blood flow during exercise
- Effect
- Chemical irritation of nerves
Why flexion helps: Flexion INCREASES canal diameter (ligamentum flavum stretches, foramina open). Extension DECREASES canal diameter (ligamentum flavum buckles, foramina narrow). This explains the "shopping cart sign" - patients prefer flexion!
Classification Systems
Anatomical Classification
- Structures
- Canal narrowing
- Symptoms
- Bilateral claudication, diffuse leg symptoms
- Structures
- Anterolateral gutter
- Symptoms
- Radiculopathy, unilateral or asymmetric
- Structures
- Neural foramen
- Symptoms
- Radiculopathy, dermatomal pattern
- Structures
- Multiple areas
- Symptoms
- Mixed symptoms
Clinical Presentation
History
Cardinal Symptom: Neurogenic Claudication
- Description
- With walking or prolonged standing
- Description
- Buttocks, thighs, legs (often bilateral)
- Description
- Heaviness, burning, aching, cramping
- Description
- Sitting, bending forward (flexion)
- Description
- Progressively shortened
Key History Questions
- Walking distance before symptoms (claudication distance)
- Relief with flexion (sitting, leaning forward)
- Cycling tolerance (usually good - flexed position)
- Ascending vs descending stairs (descending often worse - extension)
- Back pain component (may be less prominent than leg symptoms)
- Bowel/bladder symptoms (cauda equina screening)
WALKINGCLAUDICATION Symptoms
Hook:Symptoms that come with WALKING!
Neurogenic vs Vascular Claudication
- Neurogenic
- Buttocks, thighs, diffuse
- Vascular
- Calves primarily
- Neurogenic
- With walking OR standing
- Vascular
- With walking only
- Neurogenic
- Sitting/flexing forward
- Vascular
- Standing still
- Neurogenic
- Variable, may take minutes
- Vascular
- Rapid (1-2 minutes)
- Neurogenic
- Usually tolerated well
- Vascular
- May provoke symptoms
- Neurogenic
- Positive (prefers flexion)
- Vascular
- Negative
- Neurogenic
- Normal
- Vascular
- May be diminished
- Neurogenic
- Often better
- Vascular
- Worse
- Neurogenic
- Often worse
- Vascular
- Better
Clinical Examination Findings

Physical Examination
General Observation
- Wide-based, shuffling gait
- Forward-flexed posture (simian stance)
- Uses assistive devices
Lumbar Spine Examination
- Technique
- Flexion/extension
- Finding in Stenosis
- Extension often limited or provocative
- Technique
- Maintain extension 30 seconds
- Finding in Stenosis
- May reproduce leg symptoms
- Technique
- Walk then stop flexed
- Finding in Stenosis
- Longer walking if allowed to flex
- Technique
- Cycling (flexed)
- Finding in Stenosis
- Better tolerance than walking
Neurological Examination
- Findings
- Often normal at rest
- Notes
- May develop weakness after walking
- Findings
- May have patchy changes
- Notes
- Multi-dermatomal in central stenosis
- Findings
- Variable, may be diminished
- Notes
- L4 (knee jerk), S1 (ankle jerk)
- Findings
- Normal
- Notes
- Important to document (exclude vascular)
SHOPNeurogenic Claudication Signs
Hook:They prefer to SHOP (use a cart)!
Investigations
Imaging Algorithm
Standard Approach
- Investigation
- Weight-bearing X-rays
- Purpose
- Alignment, instability, spondylolisthesis
- Investigation
- MRI lumbar spine
- Purpose
- Canal dimensions, soft tissue, neural compression
- Investigation
- CT (if needed)
- Purpose
- Bony detail, surgical planning
- Investigation
- CT myelogram
- Purpose
- MRI contraindicated, dynamic assessment
Plain Radiographs
Key Findings
- Disc space narrowing
- Facet arthropathy
- Spondylolisthesis (dynamic films if suspected)
- Scoliosis
- Sagittal alignment
Flexion-Extension Views
- Instability: Over 3-4mm translation or over 10-15 degrees angular change
- Important for surgical planning (fusion decision)
MRI Findings
- Description
- Loss of CSF signal around cauda
- Significance
- Indicates compression
- Description
- Concentric disc expansion
- Significance
- Anterior canal narrowing
- Description
- Hypertrophy on T1/T2
- Significance
- Posterior canal narrowing
- Description
- Enlarged facet joints
- Significance
- Lateral narrowing
- Description
- Roots pressed together
- Significance
- Severe stenosis
- Description
- Loss of epidural fat
- Significance
- Canal compromise
- Description
- Elongated, tortuous, serpiginous cauda equina roots above (± below) the stenosis on sagittal T2
- Significance
- Marker of severe, long-standing stenosis; associated in some series with poorer/slower recovery
MRI Grading (Schizas Classification)
A 7-grade scheme (A1-A4, B, C, D) based on dural sac morphology on axial T2 MRI and the rootlet/CSF ratio. Simplified:
- Description
- Rootlets clearly separated, CSF still visible
- CSF
- Present
- Description
- Rootlets occupy the whole sac but still separable, CSF still present
- CSF
- Present
- Description
- No rootlets distinguishable; epidural fat still posteriorly
- CSF
- Absent around roots
- Description
- No rootlets distinguishable AND no posterior epidural fat
- CSF
- Absent
Imaging-Clinical Correlation: Many patients have radiographic stenosis but are asymptomatic. Always correlate imaging with clinical symptoms. The level of maximum stenosis should match the clinical syndrome!
MRI Examples

Additional Investigations
- Indication
- Unclear diagnosis, radiculopathy vs neuropathy
- Information
- Localizes nerve dysfunction
- Indication
- Suspected vascular claudication
- Information
- Under 0.9 suggests PVD
- Indication
- Suspected tumor, infection
- Information
- Uptake pattern
- Indication
- Osteoporosis assessment
- Information
- Guides fusion considerations

Differential Diagnosis
- Distinguishing Features
- Calf pain, absent pulses, rapid relief with standing
- Investigation
- ABI, Doppler, angiography
- Distinguishing Features
- Groin pain, limited hip ROM, FABER positive
- Investigation
- Hip X-ray, MRI hip
- Distinguishing Features
- Stocking-glove distribution, diabetic history
- Investigation
- EMG/NCS, glucose, B12
- Distinguishing Features
- Radicular pattern, positive SLR, younger patient
- Investigation
- MRI shows focal disc
- Distinguishing Features
- Buttock pain, positive SI tests, FABER pain
- Investigation
- SI X-rays, CT, injection
- Distinguishing Features
- Bladder/bowel dysfunction, saddle anesthesia
- Investigation
- Urgent MRI
- Distinguishing Features
- Buttock pain, positive piriformis tests
- Investigation
- Clinical, MRI may show muscle
- Distinguishing Features
- Night pain, constitutional symptoms, progressive
- Investigation
- MRI with contrast
Management
Conservative Treatment
Duration: 6-12 weeks trial, may continue if improving
Flexion-based activities (cycling, swimming). Avoid prolonged extension. Rest breaks during walking. Walking aids if needed. Weight loss if applicable.
First-line: Paracetamol, NSAIDs (short course). Second-line: Gabapentin/pregabalin for neuropathic component. Muscle relaxants for acute spasm. Avoid: Prolonged opioids.
Flexion-based exercises (Williams flexion). Core strengthening. Aerobic conditioning. Postural training. Manual therapy. Aquatic therapy excellent.
Lumbar epidural steroid injection. Interlaminar or transforaminal approach. Short-term benefit (weeks to months). May delay surgery in some patients. Diagnostic value for surgical planning.
Complications
Conservative Treatment Complications
- Cause
- Natural history
- Prevention
- Monitor symptoms
- Cause
- Activity avoidance
- Prevention
- Encourage exercise
- Cause
- Prolonged use
- Prevention
- PPI cover, limit duration
- Cause
- Chronic use
- Prevention
- Avoid prolonged opioids
Surgical Complications
- Rate
- 5-10%
- Management
- Primary repair, fibrin glue
- Rate
- 2-5%
- Management
- Bed rest, blood patch if needed
- Rate
- 1-3%
- Management
- Antibiotics, debridement if deep
- Rate
- 0.5-1%
- Management
- Prevent with careful technique
- Rate
- 5-10% (late)
- Management
- Fusion if symptomatic
- Rate
- 10-15% at 10 years
- Management
- Revision surgery
- Rate
- 2-3% per year (if fused)
- Management
- Surveillance, may need extension
DURALLaminectomy Complications
Hook:Protect the DURAL sac!
Postoperative Care
Laminectomy Protocol
Immediate (Day 0-2)
- Mobilize day 0-1 (walking)
- DVT prophylaxis
- Pain management (multimodal)
- Wound check daily
- Neurological monitoring
Early (Weeks 1-6)
- Wound check at 2 weeks
- Gradually increase activity
- No bending, lifting, twisting initially
- Walking encouraged
- Physiotherapy referral at 4-6 weeks
Intermediate (Weeks 6-12)
- Progressive strengthening
- Return to sedentary work 4-6 weeks
- Return to manual work 8-12 weeks
- Full activity by 3 months
Expected Recovery
- Recovery Pattern
- Often immediate improvement
- Recovery Pattern
- Progressive improvement over weeks
- Recovery Pattern
- May take longer to improve
- Recovery Pattern
- Variable, may not fully resolve
- Recovery Pattern
- Gradual improvement if preoperative deficit
Guidelines, Registries & Global Practice
Global Epidemiology
- Radiographic stenosis is present in 20-30% of people over 60; only 5-10% are symptomatic
- Lumbar decompression is among the most common spine operations in adults over 65 worldwide
- L4-5 is the most frequently operated level across populations
Side-by-Side Society Guidance
- Position
- Evidence-based guideline supports decompression for symptomatic stenosis after failed non-operative care; routine fusion not recommended for stenosis without instability
- Position
- Conservative care first (exercise, analgesia); image only when surgery is being considered; decompression for refractory neurogenic claudication
- Position
- Stepwise conservative trial then decompression; epidural steroid for short-term relief with limited durable benefit
- Position
- Decompression remains gold standard; add fusion selectively for instability or deformity
Decompression Alone vs Decompression Plus Fusion
The SLIP (Ghogawala, NEJM 2016) and Swedish Spinal Stenosis Study (Forsth, NEJM 2016) trials addressed whether stenosis with degenerative spondylolisthesis needs added fusion. They reached differing conclusions, so practice varies: many surgeons add fusion for clear dynamic instability or significant slip, while decompression alone is increasingly accepted for stable Grade 1 slips. Registry data (e.g. national spine registries) show rising fusion rates without proportionate outcome gains, prompting more selective use.
High- vs Limited-Resource Variation
- High-resource settings: ready MRI access, microscope or tubular (minimally invasive) decompression, instrumented fusion, and Enhanced Recovery After Surgery (ERAS) pathways with early mobilisation
- Limited-resource settings: greater reliance on clinical diagnosis and plain films/CT, open laminectomy as the default decompression, and longer conservative trials where surgical capacity is constrained
Medication Principles (non-billing)
- First-line analgesia: paracetamol and a short course of NSAIDs with gastroprotection
- Neuropathic agents (gabapentin/pregabalin) have limited evidence in stenosis and should be reserved for a clear neuropathic component
- Avoid prolonged opioids
MCQ Practice Points
Q: What are the key distinguishing features between neurogenic and vascular claudication? A: Neurogenic claudication (lumbar stenosis): relieved by sitting or bending forward (shopping cart sign), proximal-to-distal spread, variable walking distance, pulses present, and the bicycle (flexed) test is tolerated. Vascular claudication (PVD): relieved by standing still, distal-to-proximal spread, fixed walking distance, and diminished or absent pulses. Always check pulses to avoid missing PVD.
Q: What defines absolute lumbar spinal stenosis on imaging? A: Absolute stenosis: AP canal diameter under approximately 10-11mm OR dural sac cross-sectional area under 100mm². Relative stenosis: AP diameter 10-13mm. Lateral recess under 3mm and foraminal height under 15mm are additional thresholds. MRI is the gold standard; the Schizas morphological grade adds prognostic value beyond raw area.
Q: What did the SPORT stenosis trial show and what are the surgical indications? A: SPORT showed decompression was superior to nonoperative care in the as-treated analysis, with benefit sustained to 4 years; the intention-to-treat result was diluted by high crossover. Surgery is indicated for failed 6-12 weeks of conservative care, progressive neurological deficit, cauda equina syndrome (emergency), and intractable symptoms limiting function.
Q: What are the surgical options and when is fusion added? A: Decompression alone (laminectomy/laminotomy, preserving over 50% of each facet) for a stable spine. Add fusion for spondylolisthesis, segmental instability on flexion-extension films, more than 50% facetectomy, or recurrent stenosis. The most common intraoperative complication is dural tear (5-10%).
Common Examination Pitfalls
- Confusing neurogenic and vascular claudication (always check pulses)
- Missing spondylolisthesis on imaging (look for it specifically)
- Forgetting to assess stability with flexion-extension views
- Not correlating imaging stenosis with clinical symptoms
- Overlooking cauda equina red flags
At a Glance
- Key Information
- Canal narrowing causing neural compression
- Key Information
- 60-70 years (degenerative)
- Key Information
- L4-5, then L3-4
- Key Information
- Neurogenic claudication
- Key Information
- Pain with walking, relief with sitting/bending forward
- Key Information
- Shopping cart sign (flexion preference)
- Key Information
- MRI gold standard
- Key Information
- Under 11mm AP canal diameter
- Key Information
- Laminectomy plus/minus fusion
NARROWLumbar Stenosis Key Features
Hook:The canal gets NARROW!
FLEXEDStenosis vs Vascular Claudication
Hook:Neurogenic = FLEXED position helps!
NVCDNeurogenic vs Vascular Claudication
Hook:Neurogenic: Cart helps. Vascular: Circulation problem!
SILLFusion Indications in Lumbar Stenosis
Hook:SILL patients need fusion for STability!
CESSCauda Equina Syndrome
Hook:CESS = Surgical Emergency, don't wait!
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is your diagnosis and management approach?”
“How does spondylolisthesis affect your surgical planning?”
“What are the surgical considerations for multilevel stenosis in this high-risk patient?”
Key Definitions
- Canal narrowing causing neural compression and neurogenic claudication
- Absolute stenosis: Under 11mm AP diameter or under 100mm2 cross-sectional area
- Types: Central, lateral recess, foraminal, or combined stenosis
- Etiology: Degenerative (most common), congenital, post-traumatic, iatrogenic
Clinical Features
- Most common level: L4-5 (80%), then L3-4
- Cardinal symptom: Neurogenic claudication - leg symptoms with walking, relieved by flexion
- Key sign: Shopping cart sign - prefers flexion (opens canal)
- Extension worsens symptoms - ligamentum flavum buckles, foramina narrow
Neurogenic vs Vascular Claudication
- Neurogenic: flexion relief, better uphill, can cycle, normal pulses
- Vascular: standing still relief, calf pain, worse uphill, diminished pulses
- Neurogenic relief timing: Variable (minutes); Vascular: rapid (1-2 min)
- Both: Progressive reduction in walking distance
Imaging
- First-line: MRI - shows canal dimensions, soft tissue, neural compression
- Flexion-extension films: Assess for instability (over 3-4mm translation)
- Schizas grading: A (mild) to D (severe) based on CSF and root visibility
- CT myelogram: Alternative if MRI contraindicated, excellent bony detail
Management
- Conservative Rx: Flexion exercises, NSAIDs, physio, epidurals; trial 6-12 weeks
- Surgery indication: Failed conservative Rx, functional limitation, progressive deficit
- Standard surgery: Laminectomy (preserve over 50% facet to avoid instability)
- Add fusion if: Spondylolisthesis, instability, over 50% facetectomy
Evidence and Complications
- SPORT trial: Surgery superior in as-treated analysis; 80% improved at 2-4 years
- Dural tear: Most common intraop complication (5-10%); primary repair with fibrin glue
- Recurrent stenosis: 10-15% at 10 years may need revision
- Adjacent segment disease: 2-3% per year if fused
Evidence Base
Natural History
- Progressive decline in walking distance
- Neurological deterioration in minority
- Some patients stable for years
- Rarely causes complete paralysis
Evidence Base
SPORT Trial - Spinal Stenosis (without spondylolisthesis)
- Randomized (n=289) plus observational (n=365) cohorts at 13 US spine centers; stenosis without spondylolisthesis
- High crossover: by 2 years 67% of surgery-assigned had surgery, 43% of nonsurgical-assigned had surgery
- Intention-to-treat favored surgery on SF-36 bodily pain (mean difference 7.8, 95% CI 1.5-14.1) but not physical function or Oswestry
- As-treated (combined cohorts, adjusted): significant surgical advantage on all primary outcomes by 3 months, sustained at 2 years
SPORT Stenosis - 4-Year Results
- 4-year outcomes of the SPORT stenosis cohort (RC n=289, OC n=365)
- As-treated treatment effects favoring surgery: bodily pain 12.6 (95% CI 8.5-16.7), physical function 8.6 (95% CI 4.6-12.6)
- Oswestry Disability Index treatment effect -9.4 (95% CI -12.6 to -6.2)
- Early surgical advantages in satisfaction and self-rated progress maintained through 4 years
Verbiest - Developmental Lumbar Canal Stenosis
- First description of the radicular syndrome from developmental (congenital) narrowing of the lumbar vertebral canal
- Established the concept of absolute versus relative bony canal stenosis
- Foundational paper defining lumbar spinal stenosis as a distinct clinical entity
Schizas Morphological Grading of Stenosis Severity
- 7-grade classification (A1-A4, B, C, D) of dural sac morphology on axial T2 MRI based on the rootlet/CSF ratio
- Grades A and B retain visible CSF; grades C and D show no CSF around the rootlets
- Morphological grade identifies different patients than cross-sectional area alone; CSA over- or under-diagnosed stenosis in many cases
- Grades C and D were more likely to fail conservative treatment
Interspinous Process Device vs Conventional Decompression
- Double-blind RCT (n=159) of interspinous process device versus standard bony decompression for neurogenic claudication
- Device not superior at 8 weeks: Zurich Claudication Questionnaire success 63% (device) vs 72% (decompression)
- No difference in disability or other outcomes through 1 year
- Substantially higher early reoperation after the device (29% vs 8%, P less than 0.001)
Epidural Glucocorticoid Injections for Lumbar Stenosis
- Double-blind RCT (n=400) of epidural glucocorticoid plus lidocaine versus lidocaine alone for central LSS
- No significant difference in Roland-Morris disability at 6 weeks (adjusted difference -1.0, 95% CI -2.1 to 0.1)
- No significant difference in leg pain intensity (adjusted difference -0.2, 95% CI -0.8 to 0.4)
- Result held for both interlaminar and transforaminal approaches
References
- Weinstein JN, et al. Surgical versus nonsurgical therapy for lumbar spinal stenosis. NEJM 2008;358:794-810.
- Weinstein JN, et al. SPORT lumbar stenosis: four-year results. Spine 2010;35:1329-38.
- Phan K, Mobbs RJ. Minimally invasive versus open laminectomy for lumbar stenosis. Eur Spine J 2016;25:654-65.
- Moojen WA, et al. Effectiveness of interspinous implant surgery in patients with intermittent neurogenic claudication. Lancet 2013;381:1199-206.
- Verbiest H. A radicular syndrome from developmental narrowing of the lumbar vertebral canal. J Bone Joint Surg Br 1954;36:230-7.
- Amundsen T, et al. Lumbar spinal stenosis: conservative or surgical management? Spine 2000;25:1424-35.
- Malmivaara A, et al. Surgical or nonoperative treatment for lumbar spinal stenosis? Spine 2007;32:1-8.
- Kreiner DS, et al. An evidence-based clinical guideline for the diagnosis and treatment of lumbar disc herniation with radiculopathy. Spine J 2014;14:180-91.