The Neural Grid of the Lower Limb
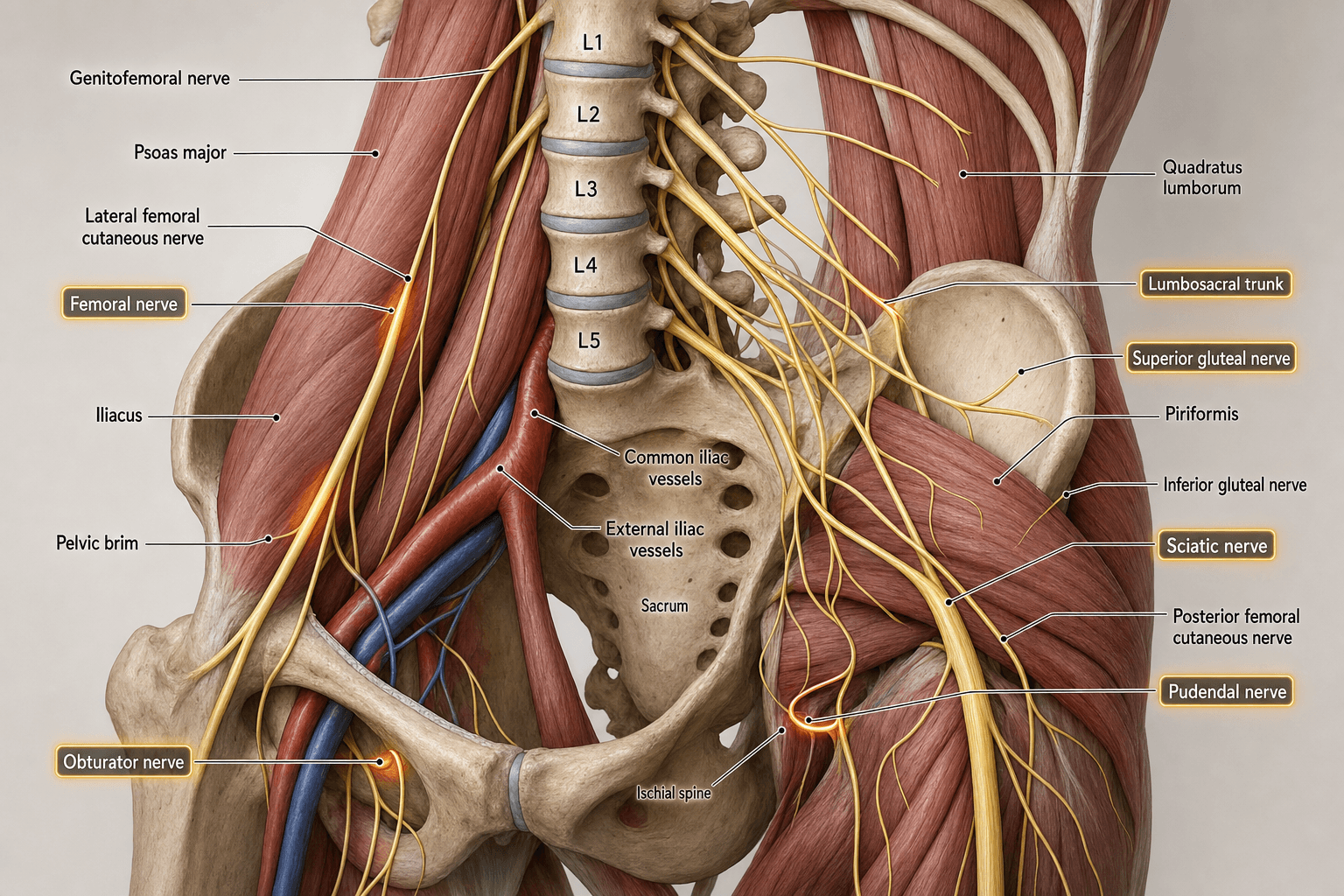
- Lumbar Plexus forms WITHIN the substance of Psoas Major.
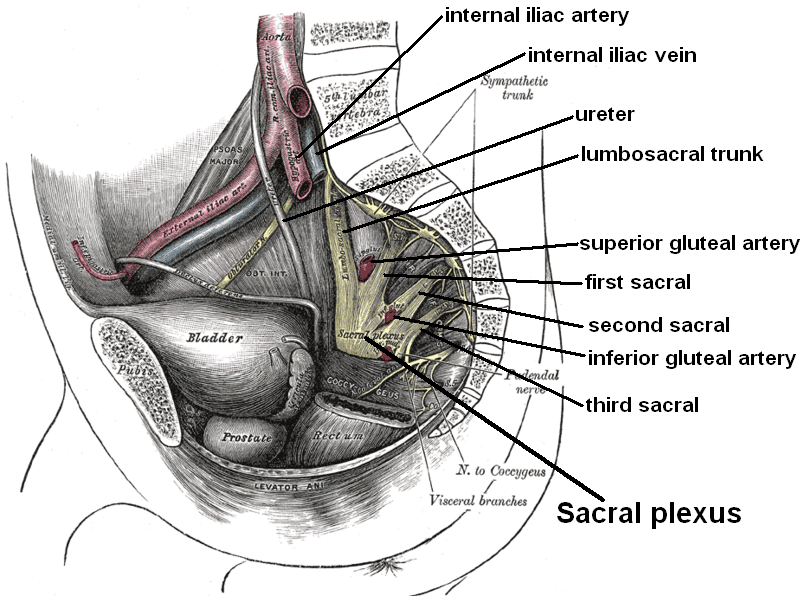
- Sacral Plexus forms on the ANTERIOR surface of Piriformis.
- Femoral and Obturator nerves arise from same roots (L2,3,4) but diverge (Femoral = Posterior division, Obturator = Anterior).
- Genitofemoral nerve runs ON the surface of Psoas (L1,2).
- Lateral Cutaneous Nerve of Thigh (L2,3) passes under Inguinal Ligament (ASIS compression).
- “Obturator nerve is the only branch of the Lumbar plexus to enter the thigh via the obturator foramen.
- “Furcal Nerve: The specific root (usually L4) that contributes to BOTH plexuses via the Lumbosacral Trunk.
- “Femoral Nerve is formed by POSTERIOR divisions (supplies extensors/anterior skin).
- “Obturator Nerve is formed by ANTERIOR divisions (supplies adductors/medial skin).
Trans-Psoas Approach.
- The lumbar plexus lies in the posterior third of the psoas muscle.
- As you go from L1 to L5, the plexus migrates anteriorly.
- Risk: At L4/5, the nerve roots are very frequent and anterior. Neural monitoring is mandatory.
Retroperitoneal Hematoma.
- Fractures of the pelvis/sacrum can cause massive bleeding.
- Compression of the lumbosacral plexus manifests as diffuse weakness (Femoral + Sciatic).
- Roots
- T12, L1
- Motor
- Transversus/Oblique
- Sensory
- Suprapubic/Gluteal
- Roots
- L1
- Motor
- Transversus/Oblique
- Sensory
- Groin/Scrotum
- Roots
- L1, L2
- Motor
- Cremaster
- Sensory
- Ant Thigh/Scrotum
- Roots
- L2, L3
- Motor
- None
- Sensory
- Lateral Thigh
- Roots
- L2, L3, L4
- Motor
- Quads/Iliacus/Sart
- Sensory
- Ant Thigh/Med Leg
- Roots
- L2, L3, L4
- Motor
- Adductors
- Sensory
- Medial Thigh
I Get Leftovers On FridaysLumbar Plexus Branches
Hook:The order they emerge (superior to inferior).
2 from 1, 2 from 2, 2 from 3Root Values - Rule of 2s
Hook:Nerves get bigger as you go down.
S-I-P-P-SSacral Plexus Branches
Hook:Major branches leaving the pelvis.
Overview
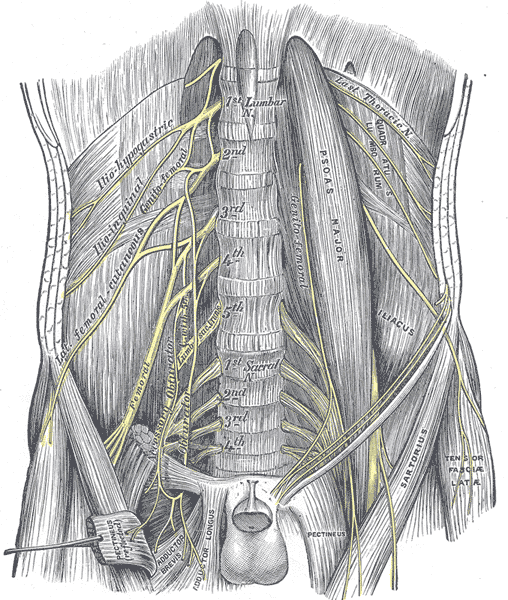
The Lumbosacral Plexus is the neural network supplying the lower limb, pelvis, and perineum. It is functionally two plexuses (Lumbar and Sacral) connected by the Lumbosacral Trunk. The lumbar plexus forms within the Psoas major muscle, while the sacral plexus lies on the surface of the Piriformis muscle.
Neurovascular
Lumbar Plexus (T12-L4)
Formed by the ventral rami of L1-L4 (with contribution from T12).
- Embedded within the posterior third of the Psoas Major muscle, anterior to the transverse processes of lumbar vertebrae.
- Lateral Border: Iliohypogastric, Ilioinguinal, Lateral Cutaneous, Femoral.
- Anterior Surface: Genitofemoral.
- Medial Border: Obturator, Lumbosacral Trunk.
Beyond the five big branches (SIPPS), the sacral plexus gives small muscular and autonomic branches that examiners use to separate strong candidates:
- Nerve to quadratus femoris (and inferior gemellus): L4-S1; runs deep to the sciatic nerve on the ischium and gives an articular twig to the hip joint.
- Nerve to obturator internus (and superior gemellus): L5-S2; leaves the pelvis through the greater sciatic foramen, hooks around the ischial spine, and re-enters through the lesser sciatic foramen.
- Nerve to piriformis: S1-S2.
- Pelvic splanchnic nerves (nervi erigentes): S2-S4 parasympathetic fibres to the pelvic viscera - they mediate erection and bladder/bowel emptying, which is why a low sacral plexus or cauda equina lesion threatens continence and sexual function.
So a "sacral plexus" answer that stops at the sciatic nerve is incomplete - the small rotator branches matter for hip external rotation and the parasympathetic outflow for pelvic-organ control.
Anatomical Imaging
Lumbar and Sacral Plexus
Surface Anatomy
Key Surface Landmarks
- ASIS: Anterior Superior Iliac Spine. Origin of Inguinal Ligament.
- Pubic Tubercle: Insertion of Inguinal Ligament.
- Psoas Major: Palpable in thin patients in the iliac fossa (flex hip against resistance).
Nerve Projections
- Femoral Nerve: Mid-inguinal point (midway between ASIS and Pubic Symphysis). Lateral to the pulse.
- LFCN: 2cm medial and inferior to the ASIS (variable).
- Sciatic: Midpoint between Ischial Tuberosity and Greater Trochanter.
- Pudendal: Medial to Ischial Spine (trans-vaginal or trans-gluteal palpation).
Knowledge of these landmarks facilitates targeted nerve blocks in the emergency department (e.g., Fascia Iliaca Block).
Classification Systems
Anatomical Variants (Zones of Emergence)
While not a formal classification, the relationship of the Lumbar Plexus to the Psoas is categorized for lateral spine surgery:
- Zone 1 (Posterior): Safe zone.
- Zone 2 (Middle): Danger zone (Femoral Nerve).
- Zone 3 (Anterior): Vascular zone.
The plexus migrates from Zone 1 to Zone 2/3 as you descend from L1 to L4.
Clinical Implication:
- At L1/2, the plexus is dorsal (Zone 1), making lateral access safe.
- At L4/5, the plexus is ventral (Zone 2/3), making lateral access high risk.
Pre-operative MRI is essential to map this migration in each patient.
Clinical Assessment
- Distribution: Weakness spanning both Femoral (Quads) and Sciatic (Hamstrings/Ankle) territories.
- Reflexes: Loss of both Knee (L3/4) and Ankle (S1) jerks.
- Sensation: Widespread loss.
- Cremasteric Reflex (L1/2): Stroke inner thigh → Testicle elevation (Genitofemoral).
- Meralgia Paresthetica: Burning pain lateral thigh. Tapping ASIS (Tinel's).
Root vs Plexus
- Root (Radiculopathy)
- Dermatomal (Single strip)
- Plexus
- Multi-dermatomal / Regional
- Root (Radiculopathy)
- Myotomal (Specific muscles)
- Plexus
- Multiple muscles + compartments
- Root (Radiculopathy)
- Radiating (Electric shock)
- Plexus
- Deep, aching, poorly localized
- Root (Radiculopathy)
- Denervated (EMG positive)
- Plexus
- Normal (Sparing)
Localising a deficit to a root versus the plexus needs the segmental map - the high-yield essentials:
- L2 - hip flexion (iliopsoas).
- L3 - knee extension (quadriceps).
- L4 - ankle dorsiflexion and inversion (tibialis anterior).
- L5 - great-toe extension (EHL) and hip abduction.
- S1 - ankle plantarflexion and eversion; hip extension.
- Knee jerk = L3-L4 (femoral nerve).
- Ankle jerk = S1-S2 (tibial nerve).
L1 groin, L2 anterior thigh, L3 medial knee, L4 medial leg and medial malleolus, L5 lateral leg and dorsum of foot (to the great toe), S1 lateral foot and sole.
A single-root pattern (one myotome plus one dermatome plus one reflex) points to a radiculopathy; a multi-myotomal deficit crossing femoral and sciatic territories with spared paraspinals points to a plexopathy.
Investigations
MRI
- MRI Lumbar Spine: Rule out disc pathology.
- MRI Pelvis (Neurogram): The gold standard for plexus visualization. Can identify:
- Tumors (Neurofibroma, Schwannoma).
- Psoas Hematoma (Hypointense/Heterogeneous).
- Piriformis pathology.
CT
- CT Abdomen/Pelvis: Essential in trauma to identify retroperitoneal bleed or fractures compressing the plexus (LI/SI joint).
Contrast is required to differentiate hematoma from muscle for accurate sizing.
Differential Diagnosis
A regional lower-limb deficit can arise at the root, plexus or peripheral nerve. The table below separates the common mimics of a lumbosacral plexopathy.
- Distribution
- Multi-myotomal, often femoral + sciatic
- Discriminator
- Paraspinals spared; reduced SNAPs
- Key Test
- MR neurogram + EMG/NCS
- Distribution
- Multi-dermatomal, may be bilateral
- Discriminator
- Saddle anaesthesia, bladder/bowel signs; SNAPs preserved
- Key Test
- Urgent MRI lumbosacral spine
- Distribution
- Single dermatome/myotome
- Discriminator
- Denervated paraspinals; preserved SNAPs
- Key Test
- MRI + EMG paraspinal sampling
- Distribution
- Quads weak, knee jerk lost
- Discriminator
- Adductors (obturator) spared
- Key Test
- Saphenous SNAP, femoral imaging
- Distribution
- Asymmetric proximal, painful, weight loss
- Discriminator
- Subacute onset in diabetic; monophasic
- Key Test
- Clinical + EMG, glucose
- Distribution
- Lateral thigh sensory only
- Discriminator
- No motor loss; Tinel at ASIS
- Key Test
- LFCN block / nerve conduction
- Distribution
- Activity-related, relieved by rest
- Discriminator
- Pulses, ankle-brachial index abnormal
- Key Test
- ABI, duplex / angiography
Management Strategy
Management Principles
- Management
- Reverse agents, Observe
- Surgical Indication
- Progressive deficit / Compartment Syn
- Management
- Reduce fracture, Stabilize
- Surgical Indication
- Bone fragment on nerve
- Management
- Biopsy, Resect
- Surgical Indication
- Mass effect / Malignancy
- Management
- Glycemic control, Pain mgmt
- Surgical Indication
- None
- Observation: Most stretch injuries or hematomas recover with time.
- Surgery: Direct repair of plexus injuries is technically difficult and outcomes are guarded. Decompression (e.g., removing bone fragment or hematoma) is more common.
Timing of surgery depends on the progression of neurological deficit and the stability of the patient.
Surgical Technique
Protecting the Plexus
- Acetabular Surgery: In anterior approach (Ilioinguinal), isolate Femoral Nerve and protect with vessel loop.
- Spine Surgery (XLIF): Use EMG monitoring. Place dilators in the anterior third of the disc space at L4/5 to avoid the forward-migrating plexus.
Strict hemostasis is vital to prevent post-op retroperitoneal hematoma.
Complications
- Chronic Pain: Complex Regional Pain Syndrome (CRPS) is a risk.
- Motor Deficit: Quadriceps weakness (Femoral) leads to knee instability (Buckling). Adductor weakness leads to gait disturbance.
- Sensory Loss: Ulceration in anesthetic areas (Foot/Heel).
- Sexual Dysfunction: Pudendal nerve involvement can cause erectile dysfunction or loss of sensation.
- Lumbosacral Trunk Injury: Often missed in pelvic fractures. Presents with non-specific foot drop and weak glutes. Requires screw removal if caused by excessive length during fixation.
- Abdominal Wall Weakness: Iliohypogastric nerve injury (via lateral ports) causes a bulge (pseudo-hernia) due to paralysis of the conjoint tendon.
Rehabilitation Protocol
- Gait Training: Knee bracing for femoral neuropathy (locking knee during stance).
- Strengthening: Core and unharmed limb compensation.
- Desensitization: For neuropathic pain.
- Orthotics: AFO for foot drop (Sciatic component).
Prognosis
- Stretch/Compression: Good prognosis if cause removed early.
- Diabetic Amyotrophy: Self-limiting but takes 12-18 months.
- Trauma (Avulsion): Poor prognosis. Root avulsions do not recover.
- Hematoma: Variable. Early decompression improves outcome.
Guidelines, Registries & Global Practice
Global Epidemiology
- Iatrogenic plexus risk in lateral spine surgery: Transient thigh/groin sensory symptoms or psoas weakness occur in roughly a quarter of trans-psoas lateral interbody fusions, with persistent motor deficit in around 1 percent (Spiessberger et al., meta-analysis of more than 13,000 patients). Risk concentrates at L4-5.
- Traumatic lumbosacral plexus injury: Reported in approximately 10 to 25 percent of displaced pelvic ring and sacral fractures, especially vertical-shear and Denis zone III sacral patterns; the L5 root / lumbosacral trunk at the sacral ala is the classic site.
- Meralgia paresthetica: A common entrapment neuropathy, associated with obesity, pregnancy, diabetes, tight belts and prone positioning; the lateral femoral cutaneous nerve lies within 2 cm of the medial ASIS in around 90 percent of people.
Side-by-Side Guidance
- Domain
- Lateral interbody fusion
- Key Position
- Stay in posterior-mid disc at upper levels, move anterior at L4-5; intraoperative neuromonitoring recommended
- Domain
- Neuromonitoring
- Key Position
- Triggered and free-run EMG plus saphenous SSEP / quadriceps MEP to protect the femoral nerve in trans-psoas corridors
- Domain
- Pelvic ring injury
- Key Position
- Early neurological documentation, transfer of complex ring injuries to a major trauma centre with pelvic and spinal expertise
- Domain
- Peripheral nerve injury
- Key Position
- Serial examination; baseline and follow-up electrodiagnostics at 3-6 weeks; refer non-recovering lesions for nerve specialist assessment
Registry & High- vs Limited-Resource Practice
- Registry signal: Arthroplasty registries (NJR, AOANJRR, AJRR, Swedish/Norwegian) capture nerve palsy as a revision-associated complication of complex/dysplastic hip reconstruction; case complexity rather than lengthening per se drives risk (Eggli et al.).
- High-resource settings: Intraoperative neuromonitoring, MR neurography and dedicated peripheral nerve / pelvic trauma services are routinely available, enabling early targeted decompression.
- Limited-resource settings: Where neuromonitoring or neurography is unavailable, surface anatomy and the documented "safe zones" become the primary safeguard, and serial clinical examination replaces electrodiagnostics for triage. Chronic neuropathic pain and CRPS remain major causes of long-term disability worldwide and benefit from early multidisciplinary pain management.
Controversies & Areas of Uncertainty
- Neuromonitoring efficacy in trans-psoas surgery: Triggered EMG is standard, but it monitors motor roots poorly and does not reliably detect femoral nerve stretch. Saphenous SSEP and quadriceps MEP improve sensitivity, yet no randomised trial proves a reduction in permanent deficit, and limiting retraction time alone is insufficient.
- Prepsoas (ATP/OLIF) vs trans-psoas access: Lower neural morbidity favours prepsoas corridors, but they carry sympathetic chain and vascular risks and cannot reach every level. The optimal corridor at L4-5 remains debated.
- Immunotherapy for diabetic / non-diabetic radiculoplexus neuropathy: Microvasculitis suggests an immune mechanism, but controlled evidence for corticosteroids or IVIg is weak; most clinicians treat supportively given the monophasic natural history.
- Timing of decompression for compressive lesions: For retroperitoneal/iliopsoas haematoma, the threshold between reversal-and-observe versus surgical evacuation is not standardised; decisions rest on progression of deficit and haemodynamics rather than haematoma size alone.
- Surgical repair of traumatic plexus injury: Direct repair of the lumbosacral plexus is technically demanding with guarded results, and the role and timing of nerve grafting versus tendon transfers and orthotics is unresolved.
MCQ Practice Points
Q: How do you differentiate L3 radiculopathy from Femoral Neuropathy clinically? A: Adductor strength. Both supply hip flexors/knee extensors (L2/3/4), but the Adductors are supplied by the Obturator Nerve (also L2/3/4).
- If Adductors clearly spared: Femoral Neuropathy.
- If Adductors weak: Plexus or Root lesion.
Q: What is the course of the Genitofemoral Nerve? A: It pierces the Psoas Major muscle anteriorly. This makes it distinct from others that emerge from the borders.
Q: What is the 'Furcal Nerve'? A: The L4 root. It is 'forked' because it contributes to both the Lumbar Plexus (via Femoral/Obturator) and the Sacral Plexus (via Lumbosacral Trunk).
Q: What are the root values of the Lateral Cutaneous Nerve of the Thigh? A: L2, L3. Posterior divisions.
Q: Which roots form the Pudendal Nerve? A: S2, S3, S4. 'S2, 3, 4 keeps the poo off the floor'.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A patient has severe groin pain and quadriceps weakness after an angiogram (femoral puncture). What is happening?”
“A slightly obese patient complains of burning pain in the lateral thigh, worse with standing or tight belts. Examination shows sensory loss in the lateral thigh but no motor deficit. Diagnosis?”
“High energy pelvic fracture. Vertical shear injury. Patient has a foot drop and weak glutes. Where is the lesion?”
Anatomy
- Lumbar: L1-L4 (in Psoas)
- Sacral: L4-S4 (on Piriformis)
- Trunk: L4/5 (Connects them)
- Femoral/Obt: L2/3/4
Clinical
- Femoral: Quads (Ext)
- Obturator: Adductors
- LFCN: Lat Thigh Sensory
- Sciatic: Hamstrings/Leg
Pathology
- Meralgia: Compressive (ASIS)
- Hematoma: Warfarin/Bleed
- XLIF: Iatrogenic L4/5
- Diabetes: Amyotrophy
Evidence Base
Anatomical Safe Working Zones for the Transpsoas Approach
- Cadaveric study (20 lumbar segments): all of the lumbar plexus, including roots, lay within psoas dorsal to the posterior quarter of the vertebral body (Zone IV)
- Safe disc-space target was the mid-posterior quarter (Zone III) from L1-2 to L3-4, but moved anteriorly to the Zone II/III junction (mid-vertebral body) at L4-5
- Genitofemoral nerve emerges from the medial psoas border at L3-4 and is at risk in Zone I anteriorly at lower levels
Transpsoas vs Prepsoas Lateral Interbody Fusion: Neural Complications
- Meta-analysis of 115 studies and 13,260 patients (2,450 prepsoas, 10,810 transpsoas)
- Transient psoas weakness or thigh/groin numbness was far higher with the transpsoas approach (26% vs 4%)
- Motor neural injury was also higher transpsoas (1.3% vs 0.4%); vascular and visceral injury rates were similar between approaches
Femoral Nerve Monitoring During Lateral Lumbar Interbody Fusion
- Multicentre series of 172 transpsoas LLIF procedures using femoral nerve evoked potentials (saphenous SSEP plus quadriceps MEP)
- In 11% the surgeon was alerted to femoral nerve deterioration during retraction; prompt countermeasures (loosen/remove retractor, raise blood pressure) restored signals with no postoperative deficit
- The two cases that ignored alerts both developed anterior thigh numbness and quadriceps weakness; limiting retraction time alone did not prevent injury
Diabetic and Nondiabetic Lumbosacral Radiculoplexus Neuropathy
- Diabetic amyotrophy is a subacute, painful, asymmetric lower-limb neuropathy with weight loss that becomes bilateral and motor-predominant
- Nerve biopsy shows ischaemic injury and microvasculitis, supporting an immune-mediated rather than purely metabolic mechanism
- It is a monophasic illness with prolonged morbidity but gradual recovery; immunomodulatory therapy remained under trial
Nerve Palsy and Leg Lengthening in THA for Hip Dysplasia
- Review of 508 THAs for developmental dysplasia: eight nerve palsies (six sciatic, two femoral)
- No statistical correlation between the amount of lengthening and palsy (p=0.47)
- Palsy correlated instead with operative difficulty - prior surgery, severe deformity, acetabular defect or flexion contracture (p=0.041)
Topographic Anatomy of the LFCN in Meralgia Paresthetica
- Cadaveric study of 33 specimens mapping the lateral femoral cutaneous nerve at the inguinal ligament
- Mean ASIS-to-LFCN distance was 8.8 mm; in around 90% the nerve lay within 2 cm of the medial ASIS and in 76% within 1 cm
- The nerve crossed the inguinal ligament at a mean angle of 83 degrees, defining a consistent but variable entrapment point
Lumbosacral Plexus Injury in Pelvic Fractures (Classic Series)
- Landmark cadaveric and clinical series describing lumbosacral plexus and trunk injury in displaced pelvic and sacral fractures
- The L4-L5 lumbosacral trunk crosses the sacral ala and is vulnerable in vertical-shear and posterior ring disruptions
- Prognosis depends on mechanism, with traction/stretch lesions recovering better than laceration