Proximal Fibula | Syndesmotic Disruption | Deltoid Injury | Unstable Ankle
- Proximal fibula fracture = must assess entire syndesmosis (membrane torn)
- Syndesmotic fixation is mandatory - unstable ankle mortise
- Weber C equivalent - proximal to syndesmosis
- Do NOT fix the fibula - it is proximal and stable, syndesmosis is the issue
- Always check full leg films if medial ankle injury with no lateral malleolus fracture
- “If medial malleolus fracture or deltoid tenderness with no fibula fracture seen - get full leg films
- “Syndesmosis must be fixed, fibula fracture does not need surgery
- “External rotation mechanism with forced pronation creates the pattern
- “Cotton test under fluoroscopy confirms syndesmotic instability
Classic exam scenario: patient with isolated medial malleolus fracture or medial tenderness. Examiner asks about further imaging. Answer: full-length tibia/fibula to exclude Maisonneuve. This injury is easily missed if you only X-ray the ankle.
The fibula does NOT need fixation - it is proximal and the bone heals well. The problem is the complete syndesmotic disruption. Must fix with syndesmotic screws or suture button across tibiofibular joint.
Medial injury is mandatory for ankle instability. Either medial malleolus fracture or deltoid ligament rupture. If deltoid torn, MRI may show but clinical exam (medial tenderness, stress views) usually sufficient.
Stress testing essential. Cotton test (lateral translation under fluoro) and external rotation stress test. Greater than 4-5mm diastasis or any lateral translation = unstable syndesmosis.
- Assessment
- Usually stable, no displacement
- Treatment
- NO SURGERY - heals with rest
- Assessment
- Always completely disrupted
- Treatment
- SYNDESMOTIC FIXATION (screws or suture button)
- Assessment
- If fractured - assess displacement
- Treatment
- ORIF if displaced
- Assessment
- If intact medial malleolus - deltoid torn
- Treatment
- May heal with syndesmotic stabilization, or direct repair if open
- Assessment
- Post-reduction films critical
- Treatment
- Must be anatomic - any talar shift unacceptable
SYNDESMOSISSYNDESMOSIS - Fixation Principles
Hook:SYNDESMOSIS guides your surgical fixation approach
FIBULAFIBULA - Why NOT to Fix Proximal Fracture
Hook:FIBULA reminds you the fibula fracture itself doesn't need fixation
COTTONCOTTON - Syndesmotic Stress Test
Hook:COTTON test (after Frederick Cotton) confirms syndesmotic instability
Overview and Epidemiology
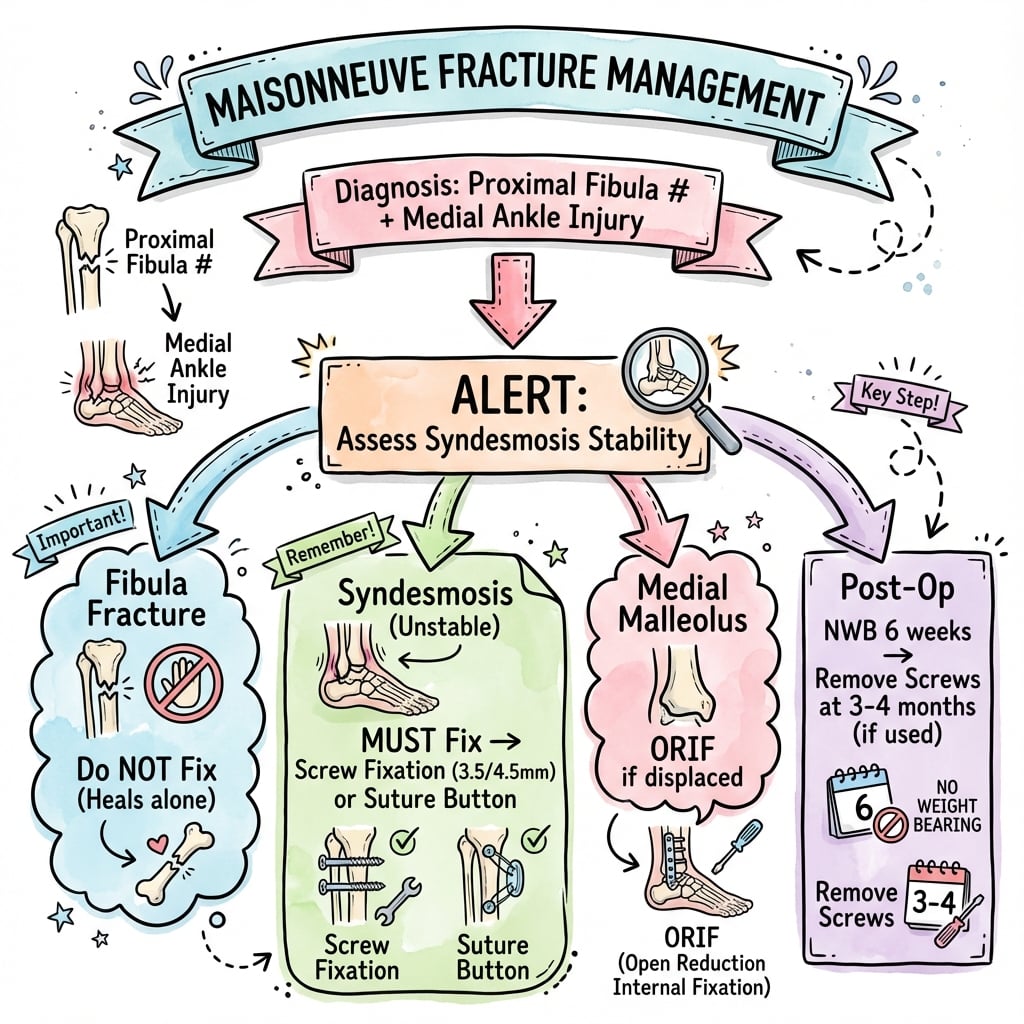
Maisonneuve fracture is a fracture of the proximal third of the fibula associated with disruption of the distal tibiofibular syndesmosis and injury to the medial ankle structures (medial malleolus fracture or deltoid ligament rupture).
Jules Germain François Maisonneuve (1809-1897), French surgeon who described this injury pattern in 1840.
The energy of the external rotation injury is transmitted through the interosseous membrane, causing the fibula to fracture proximally rather than at the ankle level. This creates a Weber C equivalent injury with complete syndesmotic disruption.
- 5% of all ankle fractures
- Often missed initially (up to 20% in some series)
- Peak incidence 20-50 years
- Equal male-female distribution
- Associated with sports injuries and falls
The classic exam scenario presents a patient with an isolated medial malleolus fracture or medial ankle tenderness without fibula fracture. You MUST order full-length tibia/fibula films to exclude Maisonneuve fracture. Missing this diagnosis leads to chronic ankle instability.
Clinical significance:
- Represents complete syndesmotic disruption
- Ankle mortise is unstable
- Requires surgical stabilization
- The proximal fibula fracture itself does NOT require fixation
Anatomy and Biomechanics
Distal tibiofibular syndesmosis:
The syndesmosis is a complex of ligaments that stabilize the distal tibiofibular joint:
-
Anterior inferior tibiofibular ligament (AITFL)
- Runs obliquely from anterolateral tibia to anterior fibula
- First structure injured in external rotation
- Prevents anterior fibular translation
-
Posterior inferior tibiofibular ligament (PITFL)
- Strongest syndesmotic ligament
- Runs from posterolateral tibia to posterior fibula
- Includes the posterior malleolus component
-
Interosseous ligament
- Thickened distal portion of interosseous membrane
- Primary restraint to syndesmotic widening
- Disrupted along entire length in Maisonneuve
-
Transverse tibiofibular ligament
- Deep component of PITFL
- Inferior continuation of posterior ligament
Interosseous membrane:
- Connects tibia and fibula along their entire length
- Transfers load from tibia to fibula (10-15% of axial load)
- In Maisonneuve, membrane torn from ankle to level of fibula fracture
- Allows proximal migration of injury energy
In Maisonneuve fracture, the interosseous membrane is torn from the ankle to the level of the fibula fracture. This represents complete syndesmotic disruption - the most severe form of syndesmotic injury.
Medial structures:
For ankle instability, medial injury is required:
- Characteristics
- Visible on X-ray, transverse pattern
- Treatment
- ORIF if displaced
- Characteristics
- Tenderness, no fracture visible
- Treatment
- May not need repair if syndesmosis stabilized
Mechanism of injury:
Foot is planted, body rotates externally. This is the same mechanism as Weber C fractures. The talus rotates externally in the mortise.
The anterior syndesmotic ligament tears first. This allows lateral shift of fibula.
Instead of fibula fracturing at ankle level, the energy propagates up through the interosseous membrane. The membrane tears sequentially.
The membrane injury stops when fibula fractures proximally. Fracture usually at junction of proximal and middle thirds.
For the ankle to dislocate/sublux, medial structures must fail. Either medial malleolus fractures or deltoid ligament ruptures.
The fibula fractures proximally because the interosseous membrane is more easily torn than the fibula. The energy travels up the leg through membrane disruption until it finds a weak point in the bone - typically the proximal third where the fibula is thinnest.
Classification Systems
Weber Classification Context
Maisonneuve fractures are classified as Weber C equivalent:
- Fibula Fracture Level
- Below syndesmosis
- Syndesmotic Injury
- Intact
- Fibula Fracture Level
- At syndesmosis level
- Syndesmotic Injury
- Partial/Variable
- Fibula Fracture Level
- Above syndesmosis
- Syndesmotic Injury
- Complete disruption
- Fibula Fracture Level
- Proximal third (far above)
- Syndesmotic Injury
- Complete disruption
The key point is that Maisonneuve fractures have the same syndesmotic implications as Weber C - complete disruption requiring fixation.
Although the fibula fracture is very proximal, Maisonneuve is treated as a Weber C equivalent because syndesmotic disruption is complete. The treatment is syndesmotic fixation, not fibula fixation.
Clinical Presentation and Assessment
History:
- Mechanism: fall, twisting injury, sports injury
- External rotation force on planted foot
- May describe "pop" or "snap" at time of injury
- Pain at ankle AND may have calf/proximal leg pain
- Unable to weight bear
Physical examination:
- Finding
- Tenderness over medial malleolus or deltoid
- Significance
- Confirms medial injury - essential component
- Finding
- May have minimal tenderness
- Significance
- No fibula fracture at ankle level
- Finding
- Tenderness at fibula head/neck
- Significance
- Key clinical finding - palpate entire fibula!
- Finding
- Tenderness along length of leg
- Significance
- Indicates membrane disruption
- Finding
- Marked swelling and ecchymosis
- Significance
- Energy of injury
- Finding
- Pain at ankle with calf squeeze
- Significance
- Positive indicates syndesmotic injury
In ANY patient with medial ankle injury without lateral malleolus fracture, you MUST palpate the entire fibula from ankle to knee. Tenderness at proximal fibula = Maisonneuve fracture until proven otherwise.
The proximal-third fibula fracture sits close to where the common peroneal nerve winds around the fibular neck, so a neurological examination is mandatory and easily forgotten in the rush to spot the syndesmotic injury:
- Test and record before any intervention: ankle and great-toe dorsiflexion and eversion (motor), and sensation over the first dorsal web space (deep peroneal) and dorsum of the foot (superficial peroneal). A foot drop or web-space numbness signals common peroneal nerve involvement.
- It is usually a traction/contusion neurapraxia from the same external-rotation energy rather than a transection, and most recover - but it must be documented at presentation so a new post-operative deficit is not wrongly blamed on later care.
- It is also a reason the proximal fibula is left alone: surgically approaching the proximal fibula/neck to "fix" the fracture needlessly puts this nerve at risk for no mechanical benefit.
Exam point: in every Maisonneuve, examine and document common peroneal nerve function (foot drop, first-web-space sensation) - the proximal fibula fracture is right at the nerve, and a missed pre-operative palsy becomes a medicolegal trap.
-
Squeeze test (Hopkinson test)
- Compress tibia and fibula at mid-calf level
- Positive: pain at ankle (indicates syndesmotic injury)
- Highly sensitive but not specific
-
External rotation stress test
- Stabilize tibia, externally rotate foot
- Pain at syndesmosis = positive
- May show widening on stress fluoroscopy
-
Cotton test (under fluoroscopy)
- Apply lateral translation force to talus
- Positive: visible lateral shift of fibula from tibia
- Definitive test for syndesmotic instability
- Isolated medial malleolus fracture seen on ankle films
- OR medial tenderness without lateral fracture
- → Palpate proximal fibula
- → If tender, order full-length tibia/fibula films
- → If proximal fibula fracture seen = Maisonneuve fracture
Investigations
Imaging is essential for:
- Confirming Maisonneuve pattern
- Assessing medial malleolus fracture
- Evaluating syndesmotic widening
- Surgical planning
Ankle series (AP, lateral, mortise):
- Key Findings
- Medial malleolus fracture, clear space widening
- Key Findings
- Tibiofibular overlap (normally greater than 1mm), clear space (normally under 4mm)
- Key Findings
- Posterior malleolus involvement, talar subluxation
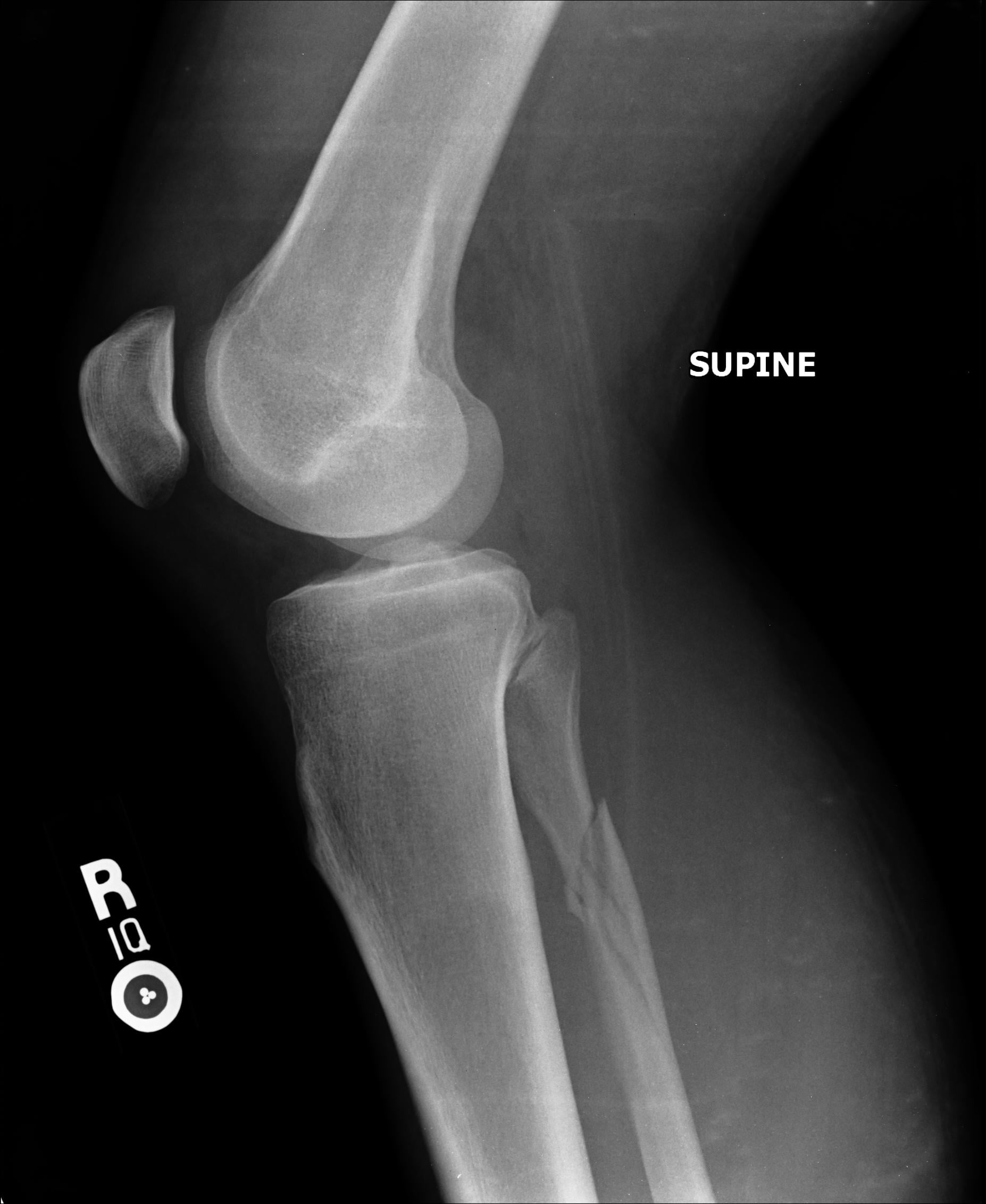
Full-length tibia/fibula films:
Essential for diagnosis! Shows:
- Proximal fibula fracture (usually spiral pattern)
- Location of fracture (typically junction of proximal and middle thirds)
- Extent of interosseous membrane disruption inferred
Order full-length films if: (1) Isolated medial malleolus fracture, (2) Tibiofibular clear space widened greater than 5mm, (3) Tibiofibular overlap under 1mm on mortise view, (4) Medial clear space greater than 4mm.
Radiographic parameters for syndesmotic injury: Tibiofibular clear space greater than 5mm (AP view), tibiofibular overlap less than 1mm (mortise view), and medial clear space greater than 4mm (mortise view).

Management Algorithm
Key principles:
-
The fibula fracture does NOT need fixation
- Proximal fibula heals well without surgery
- No mechanical advantage to fixing it
- Would require additional proximal incision with peroneal nerve risk
-
Syndesmotic fixation is mandatory
- Complete disruption = unstable ankle mortise
- Without fixation, chronic instability and arthritis develop
- Syndesmotic screws or suture button
-
Medial malleolus fixation if displaced
- Standard ORIF with screws/plate
- Separate medial incision
-
Deltoid ligament may not need repair
- If syndesmosis stabilized and mortise congruent
- Some surgeons explore and repair
- Evidence unclear on benefit of routine repair
The proximal fibula fracture is NOT fixed surgically. It heals without intervention. Attempting to fix it risks peroneal nerve injury and adds no benefit. The problem is the syndesmosis, not the fibula.
The classic teaching ("don't fix the fibula, fix the syndesmosis") is incomplete by modern CT-based standards: a posterior malleolus fracture accompanies roughly 80% of Maisonneuve injuries (Bartonicek/Rammelt), and it is frequently the missed component because attention is fixed on the proximal fibula and medial side.
Why it matters:
- The PITFL (the strongest syndesmotic ligament) inserts on the posterior malleolus, so the posterior fragment carries the posterior syndesmotic complex. Anatomically reducing and fixing a significant posterior malleolus fragment restores posterior syndesmotic stability and can reduce reliance on - or improve the reduction achieved by - trans-syndesmotic screws/buttons.
- Get a CT: the posterior malleolus is poorly characterised on plain films, and CT defines fragment size, displacement and the joint surface for surgical planning.
- Sequence matters: when a substantial posterior fragment is present, many surgeons address (reduce/fix) the posterior malleolus first, then reassess syndesmotic stability and reduce the fibula into the incisura - rather than reflexively placing a syndesmotic screw across a still-malpositioned mortise.
Exam point: in a modern Maisonneuve answer, say you would CT for the posterior malleolus (present in ~80%), fix a significant fragment first to restore the PITFL/posterior syndesmosis, then reduce the fibula anatomically into the incisura and confirm stability - not just "put a syndesmotic screw in."
Surgical Technique
- Supine on radiolucent table
- Bump under ipsilateral hip (10-15 degree internal rotation of leg)
- Tourniquet on thigh (optional)
- Fluoroscopy accessible for AP, lateral, and mortise views
- Standard fracture set
- Reduction clamps
- 3.5mm or 4.5mm cortical screws for syndesmosis
- OR suture button device (TightRope, etc.)
- Small fragment set if medial malleolus ORIF needed
Lateral approach over distal fibula for syndesmotic fixation. Medial approach if medial malleolus ORIF required. The proximal fibula is NOT approached surgically.
Complications
- Incidence
- 10-20%
- Prevention/Management
- Careful intraoperative reduction, multiple views, compare to contralateral
- Incidence
- 5-15%
- Prevention/Management
- Consider early removal (3-4 months), or use suture button
- Incidence
- 10-30%
- Prevention/Management
- Anatomic reduction of mortise, address all injuries
- Incidence
- 5-10%
- Prevention/Management
- Adequate syndesmotic fixation, treat all components
- Incidence
- 5-10%
- Prevention/Management
- Occurs in interosseous membrane, rarely symptomatic
- Incidence
- 10-20%
- Prevention/Management
- Early motion when stable, aggressive physiotherapy
- Incidence
- 5%
- Prevention/Management
- Standard wound care, wait for wrinkle test if swollen
Syndesmotic malreduction:
The most important complication to avoid. Malreduction occurs when:
- Fibula is externally rotated in the incisura
- Fibula is posteriorly translated
- Fibula is overcompressed or undercompressed
Even 1-2mm of malreduction increases contact pressures and leads to arthritis. Intraoperative CT may detect subtle malreduction not seen on fluoroscopy.
Studies show syndesmotic malreduction rates of 15-25% even among experienced surgeons. This emphasizes the importance of careful reduction technique and multiple imaging views.
Screw management:
- Many surgeons remove syndesmotic screws at 3-4 months
- Allows return to full activity without screw breakage
- If screw breaks after union, fragments can be left
- Suture button devices avoid this issue (no removal needed)
Proximal fibula concerns:
The proximal fibula fracture typically heals without intervention. Rarely:
- Delayed union (very rare)
- Painful hardware if inadvertently fixed
- Peroneal nerve injury if surgical approach attempted
Leave the proximal fibula alone - it will heal.
Postoperative Care
Rehabilitation protocol:
- Posterior splint or cast
- Non-weightbearing with crutches/walker
- Elevation to control swelling
- Wound checks at 2 weeks
- Active toe movement encouraged
- Convert to removable boot
- Begin ROM exercises out of boot
- Dorsiflexion/plantarflexion exercises
- Continue non-weightbearing
- Physiotherapy referral
- Begin weight-bearing as tolerated in boot
- Progress to regular shoes with support
- Strengthening exercises (theraband, calf raises)
- Balance and proprioception work
- Radiographic check at 6-8 weeks
- Full weight-bearing in regular shoes
- Progressive activity increase
- If screws in place, consider removal at 3-4 months before full activity
- Sport-specific training
- Full recovery expected by 6 months
Screw removal:
- When
- 3-4 months
- Considerations
- Allows full activity without risk of breakage
- When
- If painful/stiff
- Considerations
- Some screws become prominent
- When
- If asymptomatic
- Considerations
- May break with full activity but often tolerated
- When
- No removal needed
- Considerations
- Dynamic fixation, no hardware removal surgery
Return to work/sport:
- Sedentary work: 2-4 weeks (with limitations)
- Manual labor: 3-6 months
- Running/jogging: 4-6 months
- Contact sports: 6 months minimum
- Full recovery: 6-12 months
Most protocols keep patients non-weightbearing for 6 weeks after syndesmotic fixation. This allows membrane healing. Some surgeons allow earlier weightbearing with suture button devices due to dynamic fixation properties.
Outcomes and Prognosis
- Accurate syndesmotic reduction
- Early surgical treatment
- Anatomic medial malleolus fixation
- Compliant patient with rehabilitation
- Syndesmotic malreduction
- Delayed diagnosis/treatment
- Associated cartilage damage
- Persistent mortise widening
- Older age, obesity, smoking
- Result
- 85-90%
- Result
- 85-95 points (good to excellent)
- Result
- 10-30% radiographic changes, fewer symptomatic
- Result
- 80-90% at same level
Long-term outcomes:
With proper treatment:
- Most patients achieve good functional outcomes
- Some degree of stiffness may persist (especially dorsiflexion)
- Radiographic arthritis may develop but often asymptomatic
- Chronic instability rare with adequate fixation
Anatomic reduction of the mortise is the single most important factor for good outcomes. Even mild malreduction (2-3mm) significantly increases rates of arthritis and chronic pain. Intraoperative vigilance is critical.
Guidelines, Registries & Global Practice
Global epidemiology. Maisonneuve fractures account for roughly 5 to 7% of all ankle fractures and represent the most proximal expression of a pronation-external-rotation injury. In the largest dedicated series (70 patients, mean age 48 years; PMID 32349489) men predominated, the female share rose after age 50, a posterior malleolus fracture accompanied 77% of cases, a medial malleolus fracture 39% and a complete deltoid rupture 51%, with intact medial structures in only 10%. Contemporary CT-based reviews report posterior malleolar involvement in about 80% of cases (PMID 37185026). The pattern is consistent worldwide; differences between centres reflect imaging access and reduction technique rather than true biological variation.
Major guidance, side by side. No society publishes a Maisonneuve-specific guideline; recommendations are extrapolated from syndesmotic and ankle-fracture guidance.
- Position relevant to Maisonneuve
- Unstable syndesmosis requires anatomic reduction of the fibula into the incisura and fixation; open reduction preferred when malreduction risk is high; proximal fibula fracture itself not fixed
- Basis / evidence level
- Expert consensus / principle-based
- Position relevant to Maisonneuve
- Ankle-fracture appropriate-use and clinical-practice work supports operative stabilisation of unstable syndesmotic injuries; emphasises confirmation of reduction
- Basis / evidence level
- Consensus informed by Level I-II data
- Position relevant to Maisonneuve
- Open ankle and ankle-fracture standards: prompt reduction of dislocation, soft-tissue-led timing of definitive fixation, senior decision-making, anatomic mortise restoration
- Basis / evidence level
- Standard of care (consensus)
- Position relevant to Maisonneuve
- Non-complex fracture guidance (NG38): operative fixation for unstable ankle fractures; no device mandated
- Basis / evidence level
- Consensus / health-economic review
- Position relevant to Maisonneuve
- Increasing preference for dynamic suture-button fixation and routine post-operative CT to detect malreduction
- Basis / evidence level
- Supported by Level I RCT and meta-analysis
Registry and high-level evidence. Joint registries do not track syndesmosis implants discretely, so the evidence base is randomised rather than registry-derived. A Level I RCT (PMID 29298255) and a meta-analysis of five RCTs (PMID 30503612) both show dynamic suture-button fixation gives equal-or-better function, less late tibiofibular widening and far fewer implant failures than a static screw, while a cadaveric study (PMID 23405026) shows screw diameter and number of cortices have little mechanical effect. Across all constructs, malreduction is the dominant driver of poor outcome (PMID 22357084).
Global practice variation. High-resource settings increasingly favour open reduction of the distal fibula, suture-button or screw fixation, and post-operative CT to confirm reduction. Limited-resource settings rely more on closed reduction and screw fixation under fluoroscopy; because closed reduction is malreduced in up to 50% of cases (PMID 37185026), low-cost screws remain widely used where suture-button devices or CT are unavailable. Hardware-removal practice also differs (routine versus selective screw removal) - an issue largely avoided by suture-button constructs.
- Distinguishing features
- Proximal-third fibula fracture, complete syndesmotic disruption, medial injury (malleolus or deltoid)
- Key discriminator
- Proximal fibula tenderness plus widened medial clear space; full-length films diagnostic
- Distinguishing features
- Fracture at the syndesmosis level, variable stability
- Key discriminator
- Fracture seen at the ankle on standard views; proximal fibula not tender
- Distinguishing features
- Suprasyndesmotic fibula fracture with syndesmotic disruption
- Key discriminator
- Fibula fracture is distal/mid, not in the proximal third; same management principle of syndesmotic fixation
- Distinguishing features
- Medial-side injury without syndesmotic widening
- Key discriminator
- Normal medial clear space, no proximal fibula tenderness, stable on stress views
- Distinguishing features
- Direct blow or avulsion, no ankle injury
- Key discriminator
- Ankle examination and mortise normal; no syndesmotic widening
- Distinguishing features
- Foot drop / sensory loss with proximal fibula injury
- Key discriminator
- Neurological deficit dominates; assess nerve in any proximal fibula fracture
The Maisonneuve fracture is an exam favourite because it tests:
- Recognition of the injury pattern (missed diagnosis scenario)
- Understanding of syndesmotic anatomy
- Knowledge that the fibula does not need fixation
- Syndesmotic fixation technique and the screw-versus-suture-button debate
- Postoperative management including hardware removal
Expect a scenario with isolated medial ankle injury where you must recognise the need for full-length films, then justify your fixation choice with the randomised evidence above.
MCQ Practice Points
Q: What is the mechanism of Maisonneuve fracture? A: External rotation with pronation (PER mechanism). The foot is everted, and external rotation force on the planted foot causes sequential failure of medial structures, syndesmosis, and proximal fibula.
Q: What imaging should be ordered for a patient with isolated medial malleolus fracture? A: Full-length tibia/fibula radiographs to exclude Maisonneuve fracture. The medial injury without lateral ankle fracture should prompt assessment for proximal fibula fracture.
Q: Should the proximal fibula fracture in Maisonneuve be surgically fixed? A: No. The proximal fibula heals well without intervention. The problem is the syndesmosis, which must be fixed. Attempting to fix the proximal fibula risks peroneal nerve injury without benefit.
Q: What is the optimal position for syndesmotic screw placement? A: 2cm proximal to the ankle joint, angled 25-30 degrees anterior to the coronal plane (parallel to the syndesmosis). The foot should be in neutral or slight dorsiflexion during fixation.
Q: How is Maisonneuve fracture classified in the Weber system? A: Weber C equivalent. Although the fibula fracture is proximal, the complete syndesmotic disruption makes it functionally equivalent to a Weber C injury requiring syndesmotic fixation.
Q: When should syndesmotic screws be removed? A: Typically 3-4 months post-fixation, before return to full activity. This prevents screw breakage. Alternatively, suture button devices provide dynamic fixation and do not require removal.
MAISONMAISON - Maisonneuve Key Points
Hook:MAISON (French for house) - the injury is named after French surgeon Jules Maisonneuve
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old man presents to ED after twisting his ankle playing soccer. Ankle X-rays show an isolated medial malleolus fracture with no fibula fracture visible. There is 6mm medial clear space widening. What is your assessment and management?”
“You are in theatre fixing a Maisonneuve fracture. The medial malleolus has been fixed. You are now addressing the syndesmosis. Describe your technique for syndesmotic reduction and fixation. How do you confirm adequate reduction?”
“You have fixed a Maisonneuve fracture 3 months ago. The patient is doing well, walking in a boot, but is keen to return to running. The syndesmotic screws are intact on X-ray. What are your recommendations?”
DIAGNOSIS
- Proximal fibula fracture + syndesmotic disruption + medial injury
- Weber C equivalent - complete syndesmosis tear
- MISSED INJURY - always palpate entire fibula
- Order full-length films if isolated medial injury
MECHANISM
- External rotation with pronation (PER)
- Energy propagates through interosseous membrane
- Fibula fractures proximally where it's thinnest
- Medial malleolus or deltoid must fail for instability
SURGICAL PRINCIPLES
- DO NOT FIX the proximal fibula
- MUST FIX the syndesmosis (screws or suture button)
- ORIF medial malleolus if displaced
- Deltoid repair not mandatory if syndesmosis stable
SYNDESMOTIC FIXATION
- 2cm proximal to joint, angle 25-30 degrees anterior
- Tricortical or quadricortical (either acceptable)
- Foot in neutral/dorsiflexion during fixation
- Cotton test to confirm stability
RADIOGRAPHIC PARAMETERS
- Tibiofibular overlap greater than 1mm (mortise view)
- Tibiofibular clear space under 5mm (AP view)
- Medial clear space equal to superior clear space
- Any diastasis or talar shift = unacceptable
POSTOPERATIVE
- Non-weightbearing 6 weeks
- Protected weightbearing weeks 6-12
- Screw removal at 3-4 months if used
- Suture button: no removal needed
OUTCOMES
- 90%+ good/excellent outcomes
- Malreduction rate 15-25%
- Malreduction = strongest predictor of poor outcome
- Full recovery 6 months
EXAM TRAPS
- Missing the diagnosis (not palpating proximal fibula)
- Recommending fibula fixation
- Not understanding syndesmosis is the key issue
- Allowing full activity with screws in place
Evidence Base
- Prospective bilateral-CT study of 68 operatively treated syndesmotic injuries: 39% were malreduced versus the uninjured side. Malreduction was far commoner after closed reduction (44%) than open reduction (15%). Malreduced patients had significantly worse SMFA and Olerud-Molander functional scores at minimum 2 years.
- Series of 70 Maisonneuve fractures (mean age 48 years; male predominance, rising female share after age 50). A posterior malleolus fracture was present in 77%, a medial malleolus fracture in 39% and a complete deltoid rupture in 51%; medial structures were intact in only 10%. In 24% the proximal fibula fracture was visible only on the lateral lower-leg radiograph, and AITFL/PITFL injury was confirmed in all openly reduced cases.
- Randomised trial of 97 patients (48 suture button, 49 quadricortical screw). At 2 years the suture-button group had higher median AOFAS (96 vs 86) and Olerud-Molander scores, less pain on walking, and less radiographic widening: a tibiofibular distance difference of 2mm or more occurred in 20/40 screw versus 8/40 suture-button ankles. Seven screw patients had symptomatic recurrent diastasis versus none with suture button.
- Cadaveric study of 3.5mm and 4.5mm screws with tricortical and quadricortical purchase found no significant difference in distal fibular force or displacement between any size or cortex combination. External foot torque (internal tibial torque) on a loaded ankle produced the greatest screw-bending displacement.
- Retrospective comparison of 108 unstable distal fibula fractures: AAOS Foot and Ankle scores did not differ between deltoid repair, trans-syndesmotic fixation, or combined fixation at mean 4.6 years. No deltoid-repair patient required reoperation versus 26% of the trans-syndesmotic group (mainly hardware removal).
- Meta-analysis of 5 RCTs (280 patients). Suture button gave a small but statistically higher 1-year AOFAS score (mean difference 5.5) and a markedly lower implant-failure rate (odds ratio 0.03). Wound and infection rates were not significantly different.
- Contemporary CT-based review: a posterior malleolus fracture accompanies roughly 80% of Maisonneuve injuries, and closed reduction of the distal fibula is malreduced in up to 50% of cases. Anatomic reduction of the fibula into the incisura, restoration of a fractured posterior malleolus, and routine post-operative CT are advocated.