The Classic Connective Tissue Disorder
- FBN1 Gene: Fibrillin-1 mutation.
- Aortic Root: Annual echo screening essential.
- Scoliosis: Common, may be progressive.
- Protrusio Acetabuli: Characteristic finding.
- Dural Ectasia: Expand the dural sac.
- “FBN1 mutation
- “Aortic root is main mortality cause
- “Scoliosis screening needed
- “Protrusio is characteristic
Aortic root dilation and dissection are the main causes of death in Marfan Syndrome.
- Annual echocardiogram is MANDATORY.
- Beta-blockers reduce aortic root growth.
- Avoid strenuous/contact sports.
- Pre-operative cardiac clearance for scoliosis surgery.
- Description
- 30-50%
- Management
- Bracing, surgery if progressive
- Description
- Excavatum or Carinatum
- Management
- Surgical repair if severe
- Description
- Medial protrusion of acetabulum
- Management
- Usually observation
- Description
- Flat feet, hypermobile
- Management
- Orthotics
MARFSMarfan Features
Hook:MARFS - Marfanoid, Aortic, Retinal, FBN1, Scoliosis.
PPPSSkeletal Features
Hook:PPPS - Pectus, Protrusio, Pes planus, Scoliosis.
GHENTGhent Criteria
Hook:GHENT criteria - Genetics, Heart, Eyes, Numbers, Tests.
Overview/Epidemiology
Marfan Syndrome is a connective tissue disorder.
- Genetics: Autosomal dominant. FBN1 (Fibrillin-1) gene on chromosome 15.
- Incidence: 1 in 5,000-10,000.
- Pathophysiology: Defective fibrillin leads to abnormal elastic fibers and increased TGF-β signaling.
- Diagnosis: Ghent criteria (revised 2010).
Dural Ectasia: Definition, Measurement and Significance
Dural ectasia appears throughout this topic — in the must-know list, the Ghent criteria, investigations and as a surgical complication — but it is worth defining precisely because it is both a diagnostic criterion and an operative hazard.
What it is
- Dural ectasia is widening (ballooning) of the dural sac, most marked in the lumbosacral spine where CSF hydrostatic pressure is greatest. The chronically stretched, fibrillin-deficient dura expands, can scallop the posterior vertebral bodies, widen neural foramina, and form anterior sacral meningocoeles or nerve-root-sleeve (Tarlov) cysts.
- It is present in the large majority of adults with Marfan syndrome and may first appear or progress during adulthood, so a normal scan in childhood does not exclude it later.
How it is measured
- Diagnosis is radiological (MRI, or CT if MRI is contraindicated). The most-used quantitative measure is the dural sac ratio — the dural sac diameter divided by the vertebral body diameter at the same level; in ectasia the dural sac is wider relative to the vertebral body (a ratio above the threshold), the opposite of the normal taper.
- There is no single agreed cut-off, which is why reported prevalence varies; one validated proposal raises the S1 dural-sac-ratio threshold to about 0.64. Supportive qualitative signs include posterior vertebral scalloping, a widened sac and anterior meningocoele.
Why it matters clinically and surgically
- It can cause postural (low-pressure) headaches, low back pain and proximal leg pain, and rarely genitourinary symptoms from a large meningocoele.
- For the spine surgeon it is the key reason to image the lumbosacral dura before fusion: the thin, distended dura raises the risk of incidental durotomy and CSF leak, and it complicates pedicle-screw purchase where bone is scalloped.
Dural ectasia = ballooning of the lumbosacral dural sac, quantified by an elevated dural sac ratio (dural sac wider than the vertebral body). It is a Ghent systemic-score feature and, before scoliosis surgery, a red flag for durotomy and CSF leak — always image it pre-operatively.
Pathophysiology and Mechanisms
Connective Tissue Abnormalities
- Fibrillin is a component of elastic fibers.
- Abnormal elastic fibers affect aorta, ligaments, lens zonules.
- Increased TGF-β signaling contributes to aortic disease.
Why Scoliosis Develops
- Ligamentous laxity + abnormal connective tissue.
- Curves may resemble idiopathic scoliosis but can be more severe.
Classification Systems
Ghent Criteria (Revised 2010)
- Aortic root dilation (Z-score ≥2) or dissection.
- Ectopia lentis (lens dislocation).
- FBN1 mutation.
- Systemic score ≥7 (skeletal features).
- Dural ectasia.
2 major features from different systems OR FBN1 + 1 major.
Clinical Assessment
- Family history.
- Cardiac symptoms (palpitations, chest pain).
- Visual symptoms.
- Musculoskeletal symptoms.
- General: Tall, thin, arm span greater than height.
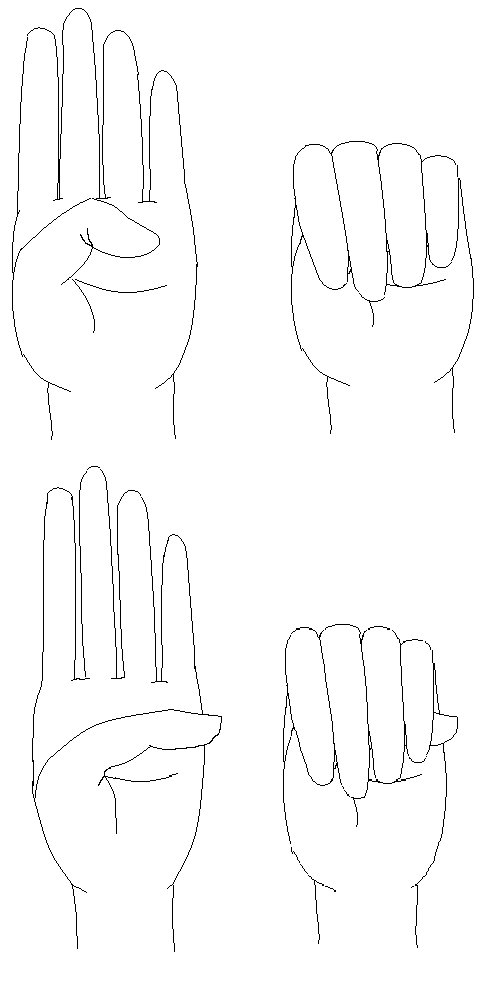
- Arachnodactyly: Long fingers. Walker-Murdoch (thumb overlaps fifth finger around wrist). Steinberg (thumb extends beyond ulnar border).
- Pectus: Excavatum or carinatum.
- Spine: Scoliosis.
- Hips: Protrusio (limited IR).
- Feet: Pes planus, hindfoot valgus.
- Eyes: Slit lamp for lens dislocation.

Investigations
- FBN1 mutation: Confirmatory.
- Echocardiogram: Aortic root measurement. Annual.
- Slit lamp: Lens dislocation.
- Spine X-ray: Scoliosis.
- Pelvis X-ray: Protrusio acetabuli.
- MRI Spine: Dural ectasia.
Differential Diagnosis
Marfan-like Syndromes:
- Gene
- FBN1
- Key Differentiator
- Aortic root dilation, lens UP
- Gene
- TGFBR1/2
- Key Differentiator
- Bifid uvula, hypertelorism
- Gene
- CBS
- Key Differentiator
- Lens DOWN, thrombosis, cognitive issues
- Gene
- COL3A1
- Key Differentiator
- Thin skin, arterial rupture
- Gene
- COL2A1
- Key Differentiator
- Flat face, hearing loss, retinal detachment
- Gene
- FBN2
- Key Differentiator
- Crumpled ears, camptodactyly
Key Distinguishing Features:
- Lens dislocation direction: Marfan UP, Homocystinuria DOWN
- Cognitive function: Normal in Marfan, impaired in Homocystinuria
- Uvula: Normal in Marfan, bifid in Loeys-Dietz
- Gene: FBN1 for Marfan, FBN2 for Beals
Management Algorithm
Cardiac Management
- Annual Echo: Monitor aortic root.
- Beta-Blockers: Reduce aortic root growth rate.
- Losartan: May also help (TGF-β blocker).
- Surgery: Aortic root replacement if dilated.
- Activity Restriction: No contact sports, strenuous activity.
Surgical Techniques
Posterior Spinal Fusion
Indications: Progressive scoliosis greater than 40-50 degrees.
Pre-op: Cardiac clearance. Echo. Avoid hypotension.
Technique: Standard posterior fusion. Curves often longer than idiopathic.
Considerations: Dural ectasia may cause CSF leak. Blood pressure management critical.
Complications
- Context
- Perioperative
- Management
- Careful BP control
- Context
- Spine surgery
- Management
- CSF leak risk
- Context
- Weak bone/tissue
- Management
- Monitor
Pulmonary Manifestations and Spontaneous Pneumothorax
The self-assessment flags "pneumothorax from apical blebs" as an anaesthetic concern, but the pulmonary involvement deserves explicit treatment because it changes how these patients tolerate surgery and ventilation.
The lung in Marfan
- The same fibrillin-deficient connective tissue weakens the lung parenchyma, producing apical bullae and blebs. Their rupture causes spontaneous pneumothorax, which occurs in a meaningful minority of Marfan patients (far above the general-population rate) and is often recurrent.
- There is also a restrictive component: severe pectus excavatum and scoliosis reduce chest-wall compliance and lung volumes, lowering pulmonary reserve. Obstructive sleep apnoea is more common (craniofacial and airway laxity).
Why it matters perioperatively
- A patient presenting with sudden pleuritic chest pain and breathlessness has a pneumothorax until proven otherwise — and the same symptoms can herald aortic dissection, so both must be excluded.
- Under general anaesthesia, positive-pressure ventilation can convert a simple pneumothorax or rupture a bleb into a tension pneumothorax; combined with the chest-wall restriction of pectus/scoliosis, this reduces ventilatory margin during long prone spinal fusions.
- Recurrent pneumothorax may need pleurodesis; document baseline lung status before major surgery.
In a Marfan patient with acute chest pain and dyspnoea, think of two emergencies at once: spontaneous pneumothorax (apical blebs) and aortic dissection. Both are connective-tissue consequences and both can present identically — exclude each. Remember positive-pressure ventilation can tension a pneumothorax intra-operatively.
Postoperative Care
- Cardiac Monitoring: Blood pressure control.
- Standard Spine Protocol: Mobilization, physiotherapy.
Outcomes/Prognosis
- Life Expectancy: Reduced (median 40-50 years historically). Improved with aortic monitoring and surgery.
- Orthopaedic: Scoliosis surgery outcomes similar to idiopathic.
Guidelines, Registries & Global Practice
Global epidemiology. Prevalence is approximately 1 in 5,000 worldwide with no clear ethnic or geographic predilection. Inheritance is autosomal dominant with high penetrance but markedly variable expressivity; roughly 25 percent of cases arise from de novo FBN1 mutations and so present without a family history.
Side-by-side guidelines:
- Position
- Diagnostic standard worldwide; aortic root and ectopia lentis are cardinal; systemic score of 7 or more
- Position
- Annual imaging of aortic root; elective root replacement at approximately 5.0 cm (lower with family history of dissection, rapid growth, or pregnancy)
- Position
- Similar surveillance; root surgery typically at 5.0 cm, individualised; valve-sparing root replacement favoured in expert centres
- Position
- Posterior spinal fusion is the dominant approach; pre-operative MRI to define dural ectasia; cardiac clearance mandatory
Surgical orthopaedic thresholds (broadly concordant globally). Brace curves of 25 to 40 degrees in the growing child; operate on curves over 40 to 50 degrees, which progress faster and respond less to bracing than idiopathic curves. Observe asymptomatic protrusio acetabuli.
Registry and resource notes. No dedicated Marfan implant registry exists; arthroplasty data are sparse because protrusio rarely requires replacement before late adulthood. National Marfan patient organisations (for example The Marfan Foundation in the US, the Marfan Trust in the UK, and equivalent bodies in many countries) coordinate multidisciplinary clinics.
High- vs limited-resource practice. In well-resourced settings, lifelong echocardiographic (and cross-sectional CT/MRI) aortic surveillance, FBN1 sequencing, valve-sparing root replacement, and neuromonitored spinal fusion are standard. Where genetic testing and advanced imaging are limited, diagnosis leans on the clinical Ghent features and echocardiography; the priority everywhere is recognising aortic risk, restricting high-intensity isometric and contact sport, and arranging cardiac assessment before any major orthopaedic surgery.
Controversies & Areas of Uncertainty
- Losartan vs beta-blockade. The Pediatric Heart Network trial (Lacro 2014) found no significant difference between losartan and atenolol for aortic-root growth, and subsequent meta-analyses suggest the two are broadly comparable. Whether combination therapy or angiotensin-receptor blockade adds benefit over beta-blockade alone remains unsettled.
- Optimal aortic-root replacement threshold. The 5.0 cm threshold is pragmatic, not absolute; family history of early dissection, rapid growth (over 3 to 5 mm/year), and planned pregnancy all argue for earlier surgery, while the relative merits of valve-sparing versus composite root replacement are debated.
- Prophylactic surgery for protrusio acetabuli. Older recommendations for triradiate closure in growing children are largely abandoned; Sponseller's data show most protrusio is well tolerated, so intervention is now reserved for genuinely symptomatic or rapidly progressive cases.
- Defining dural ectasia. There is no universally accepted radiographic cut-off; differing dural-sac-ratio thresholds affect reported prevalence and its weight within the Ghent systemic score.
- Fusion levels and approach in syndromic scoliosis. Curve length, kyphosis, pelvic obliquity, and bone fragility complicate level selection; the shift to posterior-only constructs is clear, but distal fusion levels and the role of pelvic fixation remain individualised.
MCQ Practice Points
Q: What gene is mutated in Marfan Syndrome? A: FBN1 (Fibrillin-1) on chromosome 15.
Q: What is the main cause of death in Marfan? A: Aortic dissection/rupture.
Q: What hip finding is characteristic of Marfan? A: Protrusio acetabuli.
Q: In which direction does the lens dislocate in Marfan? A: Superiorly (upward). Compare to Homocystinuria where it dislocates inferiorly.
Q: What must be done before scoliosis surgery in Marfan? A: Pre-op cardiac clearance with echo is MANDATORY. Watch for dural ectasia (CSF leak risk), curves often longer than idiopathic, and blood pressure control is critical.
Q: What are the Walker-Murdoch and Steinberg signs? A: Walker-Murdoch: Thumb overlaps fifth finger when grasping wrist. Steinberg: Thumb extends beyond ulnar border of closed fist. Both indicate arachnodactyly.
Self-Assessment Quiz
Additional Quiz Questions
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“15-year-old male with known Marfan Syndrome. Scoliosis of 45 degrees. Aortic root is 4.2cm on recent echo.”
“How do you diagnose Marfan Syndrome?”
“X-ray shows protrusio acetabuli. What is this and how do you manage?”
GENETICS
- FBN1 Mutation
- Chromosome 15
- Autosomal Dominant
- Fibrillin-1 defect
CARDIAC
- Aortic root dilation
- Annual echo
- Beta-blockers
- Main mortality cause
SKELETAL
- Scoliosis 30-50%
- Protrusio acetabuli
- Pectus
- Pes planus
DIAGNOSIS
- Ghent criteria
- Aortic root + FBN1
- Systemic score ≥7
- Ectopia lentis
CLINICAL SIGNS
- Walker-Murdoch sign
- Steinberg sign
- Arm span exceeds height
- Arachnodactyly
SURGERY PEARLS
- Cardiac clearance first
- Dural ectasia risk
- BP control critical
- Curves often longer
Evidence Base
- International expert panel re-weighted criteria toward cardiovascular disease
- Aortic root aneurysm and ectopia lentis are now the two cardinal features; together they are sufficient for diagnosis when there is no family history
- New weighted systemic score (threshold of 7 or more) and greater emphasis on FBN1 testing; molecular confirmation possible in over 95 percent
- Randomised trial, 608 children and young adults with aortic-root z-score over 3.0
- No significant difference in rate of aortic-root z-score change between losartan and atenolol over 3 years (P=0.08)
- No difference in aortic-root surgery, dissection, or death between groups
- Cross-sectional study, 173 patients (346 hips) with Marfan syndrome
- Prevalence of protrusio 16 to 27 percent depending on the radiographic criterion; rises through the first two decades then plateaus
- Only a slight reduction in hip range of motion and no clinically meaningful loss of Iowa hip score
- Prospective 10-year cohort; 45 of 46 Marfan patients had dural ectasia at follow-up
- Dural ectasia may first appear or worsen during adulthood; anterior sacral meningocoele present in roughly half
- Proposed dural-sac-ratio cut-off at S1 raised to 0.64 for diagnosis
- National database, 314 (1,410 weighted) Marfan patients undergoing spinal fusion 2003 to 2014
- Posterior spinal fusion rose from 67 percent to 92 percent of cases
- Marfan patients had higher neurologic complications than matched non-Marfan controls (2.4 vs 0.79 percent)
- Matched cohort, 20 Marfan vs 40 adolescent idiopathic scoliosis patients after posterior spinal fusion
- Marfan patients used more inpatient opioid (4.9 vs 2.1 mg/kg morphine-equivalents) despite similar pain scores
- Marfan was the only independent predictor of an outpatient opioid request (odds ratio 4.1)