Young thrower with medial elbow pain | Open medial epicondyle apophysis is the weak link | Rest early, image carefully, protect against avulsion
- Definition: Little League elbow is a valgus-overload spectrum in a skeletally immature thrower, centred on the medial epicondyle apophysis before skeletal maturity
- Weak link: in the young elbow, the open apophysis fails before the adult ulnar collateral ligament pattern dominates
- Do not over-treat the film: medial epicondylar fragmentation and ultrasound avulsive changes can be seen in young throwers without matching symptoms
- Red flag: sudden pain, a pop, swelling, loss of extension, ulnar nerve symptoms, or a displaced fragment means think medial epicondyle avulsion fracture
- First-line answer: stop throwing, remove valgus load, regain pain-free motion and strength, correct workload and kinetic-chain risk factors, then gradual return to throwing
- “A painful open medial epicondyle apophysis is the paediatric equivalent of an adult medial-sided valgus-overload injury - but the growth plate fails first
- “Ask specifically about pre-existing elbow pain before an acute throw - in the Zheng avulsion-fracture series, most patients had pain before the fracture event
- “Compare the symptomatic elbow with the other side cautiously: asymptomatic throwing elbows may still show medial changes, so clinical correlation is everything
- “Never miss an incarcerated medial epicondyle fragment after paediatric elbow dislocation - it can sit in the joint and block reduction or healing
In a skeletally immature thrower, valgus force loads the medial epicondyle apophysis. The adult answer is often ulnar collateral ligament insufficiency; the paediatric answer is usually apophyseal stress, widening, fragmentation, or avulsion.
Sakoda found medial osseous abnormalities were common in symptomatic young throwers with an open physis, and McGinley found ultrasound avulsive changes in asymptomatic dominant throwing elbows. Match the image to pain, tenderness, motion, and stability.
Sudden medial pain, a pop, swelling, loss of extension, displacement on radiographs, ulnar nerve symptoms, or elbow dislocation means medial epicondyle avulsion fracture until proven otherwise.
Rest alone is incomplete. The child needs a workload plan, coach and parent buy-in, shoulder and scapular control, trunk and hip strength, and a staged throwing progression only after pain-free examination.
Overview
Little League elbow is an overuse injury spectrum in the skeletally immature throwing athlete. The classic patient is a young baseball pitcher with medial elbow pain during or after throwing. The core lesion is stress at the medial epicondyle apophysis, the growth-related attachment region for the flexor-pronator mass and ulnar collateral ligament complex.
The exam idea is simple: the child is not a small adult. In an adult thrower, valgus overload often declares itself as ulnar collateral ligament pain or insufficiency. In a child with an open medial apophysis, the growth plate is the vulnerable structure, so repetitive valgus load produces apophyseal widening, fragmentation, sub-apophyseal avulsion change, or, at the severe end, an acute medial epicondyle avulsion fracture.
The practical approach is to separate three groups:
- Sore open apophysis: gradual medial pain, tenderness, no displaced fracture, stable elbow.
- Image-positive but clinically quiet elbow: ultrasound or radiographic change that may not equal active disease.
- Avulsion fracture or dislocation pattern: acute event, displaced fragment, instability, nerve symptoms, or entrapped fragment.
The safest examiner answer is: stop throwing early, examine carefully, image the medial epicondyle, rehabilitate the whole kinetic chain, and do not miss the avulsion fracture.
Pathophysiology / Anatomy
The throwing elbow sees a large valgus moment during late cocking and early acceleration. The medial side is distracted, while the lateral radiocapitellar joint is compressed. In a mature athlete the ulnar collateral ligament is a key restraint; in the skeletally immature athlete, the medial epicondyle apophysis is the weak link.
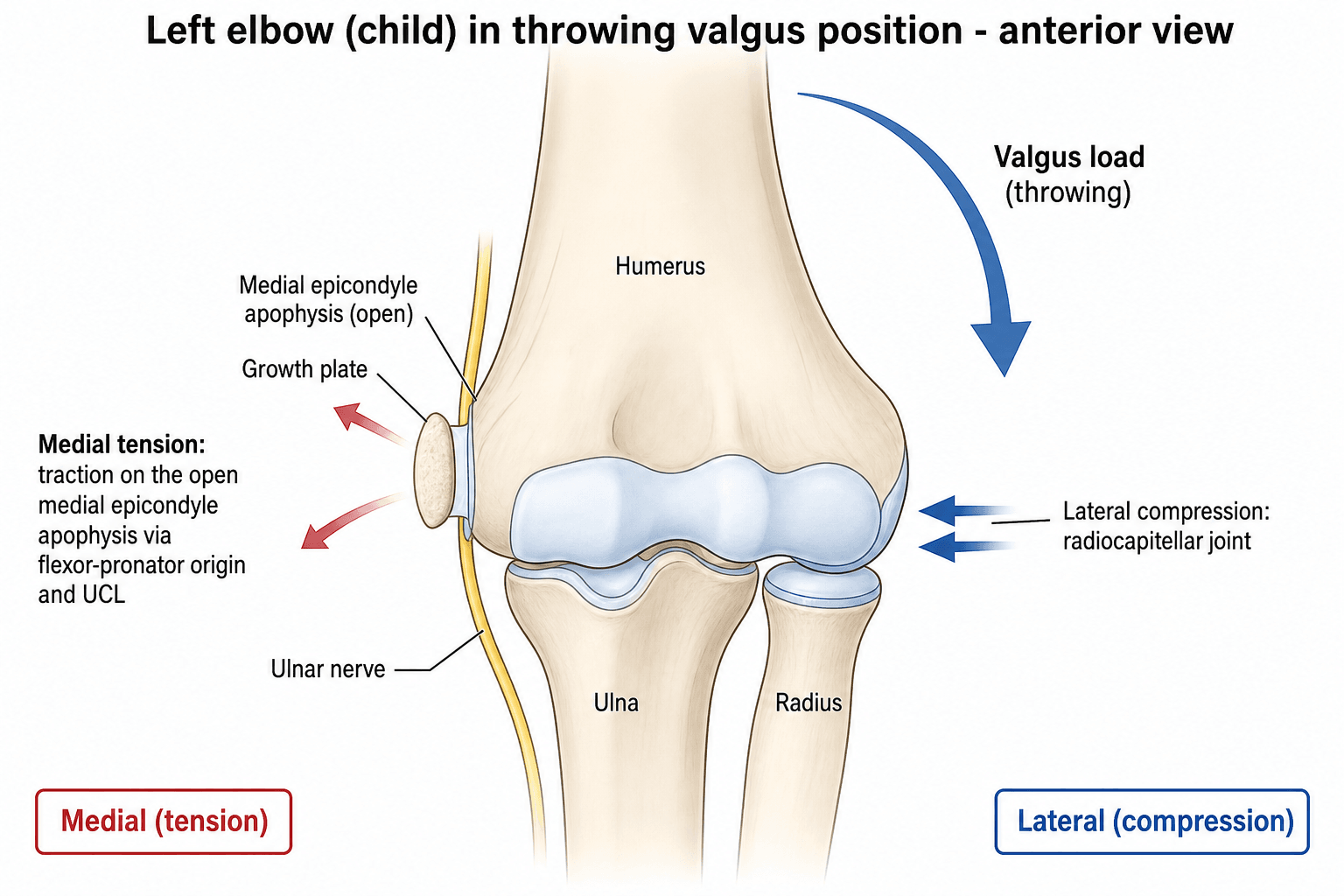
The flexor-pronator origin and ulnar collateral ligament complex load the medial epicondyle. Repeated traction across an open apophysis explains medial tenderness, widening, fragmentation, and avulsion.
Valgus load also compresses the radiocapitellar joint. That is why a throwing-elbow assessment should not stop at the medial side, especially if pain is lateral or motion is blocked.
The ulnar nerve runs behind the medial epicondyle. Ask about ring-finger and little-finger paraesthesia, examine intrinsic power, and treat nerve symptoms as a red flag in fracture or dislocation patterns.
Shoulder internal rotation deficit, scapular dyskinesis, trunk weakness, and hip stiffness can increase elbow load. Rehabilitation must therefore extend beyond the elbow.
Sakoda's radiographic study supports the load-and-maturity model: medial epicondylar abnormalities were much more common in elbows with an open physis than with a closed physis, and were strongly associated with throwing elbows rather than nonthrowing elbows.
If the examiner asks "why children get apophysitis rather than UCL rupture", answer: because the open apophysis is weaker than the ligament-bone complex, so repetitive valgus traction fails through the growth-related medial epicondyle region first.
Classification
There is no single universally used formal classification for Little League elbow. In the viva, classify by site and severity, because that is what changes management.
This is the common exam picture: gradual medial elbow pain in a skeletally immature thrower, tenderness over the medial epicondyle, pain with throwing, and radiographic or ultrasound change around the apophysis. It is a load-related diagnosis and must be interpreted with symptoms.
- Finding
- Gradual medial pain during throwing, often worse with pitching volume
- Management implication
- Stop painful throwing and identify workload error
- Finding
- Medial epicondyle tenderness, pain with valgus loading, usually preserved neurovascular status
- Management implication
- Stable and pain-limited elbows usually start non-operatively
- Finding
- Open apophysis with widening or fragmentation may be seen
- Management implication
- Do not call every fragment a fracture needing fixation
The key is correlation: pain, tenderness, and function decide whether the image represents active injury.
Lateral Compartment: Osteochondritis Dissecans and Panner Disease
The same valgus throw that distracts the medial apophysis compresses the lateral radiocapitellar joint, so the paediatric throwing elbow has a lateral-compartment differential that the medial story can hide. The two key lateral lesions are Panner disease and osteochondritis dissecans (OCD) of the capitellum, separated mainly by age and prognosis.
- Panner disease
- Younger child (about 5 to 10 years)
- Capitellar OCD
- Adolescent (about 11 to 15 years)
- Panner disease
- Osteochondrosis (avascular necrosis) of the whole capitellar ossific nucleus
- Capitellar OCD
- Focal subchondral osteochondral lesion from repetitive compression
- Panner disease
- Self-limiting; revascularises and remodels with rest
- Capitellar OCD
- Can fragment, form loose bodies and lead to later degeneration
- Panner disease
- No
- Capitellar OCD
- Yes if the fragment separates (unstable lesion)
- Panner disease
- Rest and activity modification; good prognosis
- Capitellar OCD
- Stable lesion rest; unstable lesion (fragmentation, loose body, closed physis) needs surgery
Capitellar OCD presents with lateral elbow pain, loss of extension, and catching or locking from a loose body, and is graded as stable (intact overlying cartilage, open physis, good prognosis with rest) versus unstable (fragmentation, a loose body, or a closed physis), which is the trigger for surgery - drilling of a stable but non-healing lesion, or fragment fixation, microfracture or osteochondral grafting for unstable disease. MRI is the key test when a lateral lesion is suspected.
Think Panner in the child, OCD in the adolescent. Panner disease is a self-limiting osteochondrosis of the whole capitellum in a young child (the "Perthes of the elbow"), while capitellar OCD is a focal lesion in an older throwing adolescent that can fragment and form loose bodies - lateral pain, locking or a block to extension should prompt MRI.
Clinical Presentation
History
Ask the history like a sports surgeon, not just like an elbow clinic.
Medial pain during throwing is the classic complaint. Clarify whether it is gradual soreness, pain after innings, pain during acceleration, or a sudden acute event with a pop.
Ask about pitching volume, multiple teams, year-round play, recent tournament spikes, catcher duties, and whether the child kept throwing through pain.
Ask about loss of velocity, loss of control, early fatigue, shoulder tightness, and whether symptoms settle with rest but recur when throwing resumes.
Pop, swelling, bruising, locking, loss of extension, frank instability, numbness in the ring and little fingers, or prior elbow dislocation all change the pathway.
Examination
Inspect for swelling and carrying-angle asymmetry, then assess range of motion. Palpate the medial epicondyle and flexor-pronator origin. Stress the elbow gently in valgus if fracture is not suspected, and compare the ulnar nerve examination with the other side.
- How to do it
- Check swelling, bruising, flexion, extension, pronation, and supination
- Positive finding
- Effusion or blocked extension suggests more than simple apophysitis
- How to do it
- Use one finger directly over the medial apophysis
- Positive finding
- Focal tenderness supports medial apophyseal stress
- How to do it
- With the elbow partly flexed, apply gentle valgus load only if fracture is not suspected
- Positive finding
- Pain or apprehension suggests medial-sided overload
- How to do it
- Test sensation in ring and little fingers and intrinsic hand strength
- Positive finding
- Paraesthesia or weakness is a fracture-dislocation red flag
In the viva, say out loud that you would not force a valgus stress test in a child with an acute pop, swelling, or a visible medial epicondyle fragment. Image first, stress later if safe.
Investigations
The investigation aim is to confirm the site of injury, judge skeletal maturity, and rule out avulsion fracture, dislocation, loose body, or lateral compression disease.
Start with anteroposterior and lateral elbow radiographs. Oblique views can help the medial epicondyle. Look for physeal widening, fragmentation, displaced fragment, elbow alignment, effusion, and the radiocapitellar joint.
A comparison radiograph can help in a developing elbow, but it is not magic. The dominant throwing elbow may have changes that the other side does not, even without symptoms.
Useful for dynamic, low-risk assessment of medial epicondyle and ulnar collateral ligament-apophyseal changes. McGinley used high-frequency ultrasound and showed that asymptomatic players can still have dominant-side avulsive changes.
Reserve for persistent pain, unclear radiographs, suspected cartilage or radiocapitellar injury, UCL complex concern, or when symptoms and plain films do not match.
After paediatric elbow dislocation, the medial epicondyle can be avulsed and trapped in the joint. If the reduction looks odd, extension is blocked, the medial fragment is absent from its usual position, or the child has ulnar nerve symptoms, escalate urgently.
What to report on the image
- Report it because
- Open physis supports apophyseal stress pattern
- Action if abnormal
- Advise throwing rest and follow clinically
- Report it because
- May be stress-related in young throwers
- Action if abnormal
- Correlate with tenderness and pain
- Report it because
- Displacement changes fracture management
- Action if abnormal
- Refer to paediatric orthopaedics
- Report it because
- Dislocation or subluxation can hide an incarcerated fragment
- Action if abnormal
- Urgent reduction and post-reduction imaging
- Report it because
- Valgus overload can compress the radiocapitellar joint
- Action if abnormal
- Consider MRI if lateral symptoms or motion block
The report should answer management questions, not just name the condition.
Management
Management depends on whether this is apophyseal stress without displacement or an avulsion fracture / instability pattern. The safest first sentence is: "I stop throwing and protect the physis, then I look for red flags that would move the child out of the simple-rest pathway."
Initial treatment is non-operative.
- Stop pitching and painful throwing until the elbow is pain-free at rest, during daily activity, and on examination.
- Analgesia and short activity modification are used for comfort, but the treatment is load control, not medication.
- Restore motion without forcing painful valgus stress.
- Rehabilitate the kinetic chain: shoulder rotation, scapular control, trunk and hip strength, forearm conditioning, and throwing mechanics.
- Address workload with the family, coach, and athlete so the same overload is not recreated on return.
The child should not return just because the pain is quieter for a few days; the elbow must be clinically quiet and the throwing plan must change.
For exams, do not promise a fixed number of weeks for every child. Say: "return is based on a painless examination, restored motion and strength, corrected workload, and a graduated throwing programme."
Complications
Most complications come from missed severity or premature return to load.
- Mechanism
- Return to throwing before the apophysis and kinetic chain are quiet
- How to prevent or manage
- Stop throwing again, reassess workload, and rebuild return programme
- Mechanism
- Repetitive valgus stress culminating in acute failure
- How to prevent or manage
- Recognise pop, swelling, displaced fragment, and pre-existing pain
- Mechanism
- Displaced fragment heals in residual position or fails to unite
- How to prevent or manage
- Follow symptoms, stability, and sport demand; refer if painful or unstable
- Mechanism
- Medial fragment or UCL-apophyseal complex fails to restore restraint
- How to prevent or manage
- Assess stability and throwing demand; consider specialist management
- Mechanism
- Traction, swelling, fragment displacement, or dislocation around the medial epicondyle
- How to prevent or manage
- Document nerve status and escalate if paraesthesia or weakness persists
- Mechanism
- Valgus overload compresses radiocapitellar joint
- How to prevent or manage
- Ask about lateral pain and motion block; image further if suspected
A child with persistent pain after "rest" has either not truly unloaded, has not corrected the kinetic-chain driver, or has a diagnosis beyond simple medial apophysitis. Reassess rather than repeating the same advice.
Clinical Relevance
Little League elbow is high-yield because it tests paediatric principles, sports workload, imaging judgement, and family-centred counselling in one topic. The examiner is looking for maturity of thinking: you must protect the growth plate, avoid over-calling normal or adaptive findings, and at the same time avoid missing the acute avulsion fracture.
The modern nuance is that imaging abnormalities can be common in throwing elbows. Sakoda showed radiographic medial abnormalities in many symptomatic open-physeal elbows, while McGinley showed ultrasound avulsive changes even in asymptomatic dominant elbows. Therefore, the best answer is never "the scan says it, so operate". It is: match symptoms, examination, skeletal maturity, stability, and displacement.
The clinical conversation is also important. A young athlete may be anxious about losing a season; parents and coaches may focus on tournaments. Explain that pain is a warning sign from a growth region. Early rest and controlled return are what preserve the child's future throwing, not what ends it.
Throwing Workload Guidelines (Pitch Smart)
Prevention is examinable in its own right, and the widely cited framework is the USA Baseball and MLB Pitch Smart guidance, which limits the throwing dose rather than just the technique.
- Practical rule
- Daily maximums rise with age (for example roughly 50 at age 7 to 8, up to about 105 by age 17 to 18)
- Why it matters
- Limits acute overload of the open apophysis
- Practical rule
- Required rest days scale with the number of pitches thrown
- Why it matters
- Allows recovery before the next high load
- Practical rule
- Avoid more than about 100 innings in a calendar year and take at least 4 months off overhead throwing
- Why it matters
- Year-round play is a strong risk factor
- Practical rule
- Avoid combining high-throw roles and avoid pitching on consecutive days when young
- Why it matters
- Reduces cumulative valgus load
- Practical rule
- Stop with arm pain or loss of velocity or control
- Why it matters
- Pain is a warning from the growth region
A crucial nuance is that pitch counts alone are not fully protective: in Pytiak's prospective MRI study, players fully compliant with pitch-count rules still developed medial elbow changes, and year-round play rather than pitch type drove the change. Counselling must therefore include off-season rest and shoulder internal-rotation maintenance, not pitch counts in isolation. The historical fear of the curveball has also softened - workload and year-round specialisation matter more than the specific pitch.
Pitch counts are necessary but not sufficient. Age-based daily limits with rest days, a cap of about 100 innings a year, at least 4 months off overhead throwing, and never pitching through pain are the core rules - but year-round single-sport play remains the dominant modifiable risk even when pitch counts are obeyed.
Guidelines, Registries & Global Practice
Little League elbow is a worldwide youth-sport problem, but formal orthopaedic guidelines are less central than sport workload rules, paediatric sports-medicine prevention, and local access to imaging and therapy.
- Global high-yield point
- Seen in skeletally immature throwers; baseball-heavy regions recognise it most, but any repetitive overhead throwing can load the medial apophysis
- Exam answer
- Name the risk as valgus overload of an open apophysis, not a country-specific disease
- Global high-yield point
- There is no single AAOS, NICE, BOAST, AO, or registry guideline dedicated specifically to Little League elbow
- Exam answer
- Use principles: pain means stop throwing, image red flags, protect the physis, graded return
- Global high-yield point
- No arthroplasty or implant registry applies to routine apophysitis; fracture fixation evidence comes from paediatric series rather than national registries
- Exam answer
- Do not invent registry statistics for this topic
- Global high-yield point
- High-resource settings may use early ultrasound or MRI; limited-resource settings rely more on history, examination, radiographs, rest, and referral when fracture signs appear
- Exam answer
- The management principles are the same even when imaging access differs
- Global high-yield point
- Pitch-count and rest-day systems vary by league and country, but the shared principle is avoiding year-round high-volume throwing and stopping when pain starts
- Exam answer
- Avoid quoting billing or country-specific administrative codes
The global exam answer is therefore principle-based: protect the open medial apophysis, recognise the avulsion fracture, avoid over-treating incidental imaging findings, and coordinate workload change with family and coach.
Memory aids
THROWHistory of the Painful Young Thrower
Hook:THROW keeps the viva history practical: Timing, Handed workload, Red flags, Other kinetic-chain sites, What position and pitch.
RESTManagement Ladder
Hook:REST is not passive: remove load, examine and image, strengthen the chain, then throw gradually.
POPAvulsion Fracture Red Flags
Hook:A young thrower with a POP needs fracture thinking, not just rest advice.
Clinical Imaging
Visually verified CC BY images
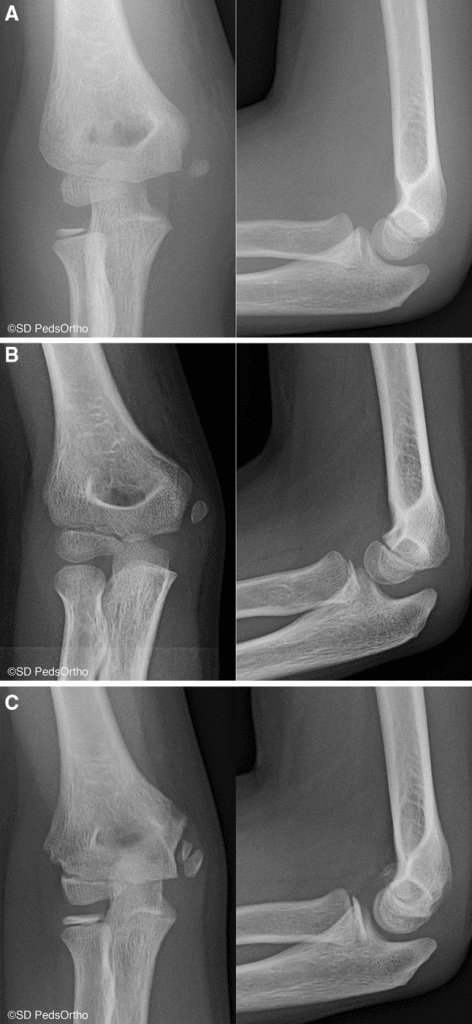
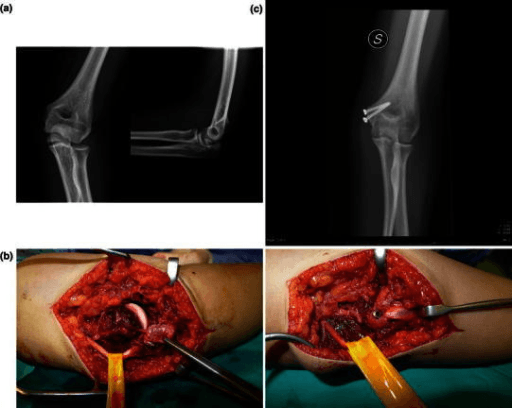
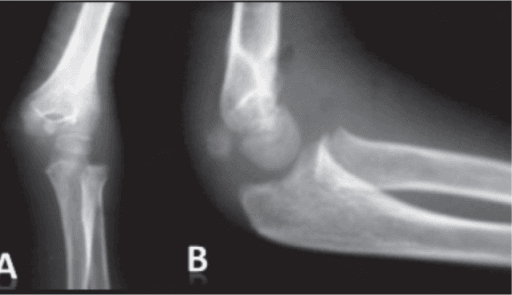
The available CC BY images show the fracture and incarceration end of the Little League elbow spectrum. A perfect CC BY image of isolated medial epicondylar apophysitis was not used because the Open-i candidate with that exact finding did not have an acceptable CC BY or CC0 licence.
These images are used to teach the red-flag fracture patterns that must not be mistaken for simple medial apophyseal soreness.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 12-year-old baseball pitcher has gradual medial elbow pain after pitching. Radiographs show an open medial epicondyle apophysis with mild fragmentation but no displaced fragment. How do you assess and manage him?”
“A 14-year-old pitcher felt a pop on the medial side of the elbow during a throw and now has swelling and loss of extension. Radiographs show a displaced medial epicondyle fragment. What is your approach?”
“A 13-year-old tournament baseball player has no elbow pain, but screening ultrasound reports a united sub-apophyseal avulsion change at the dominant medial elbow. The parent asks whether he needs surgery or a season off.”
Core Diagnosis
- Skeletally immature thrower with medial elbow pain
- Valgus overload loads the medial epicondyle apophysis
- Open apophysis is the weak link before adult UCL pattern dominates
- Image changes need clinical correlation
History and Exam
- Ask workload: pitches, teams, tournaments, year-round play, throwing through pain
- Ask red flags: pop, swelling, locking, extension block, numbness
- Examine medial epicondyle tenderness, motion, ulnar nerve, shoulder and kinetic chain
- Do not force valgus testing if acute fracture is suspected
Investigations
- AP and lateral radiographs first; oblique if needed for medial epicondyle
- Look for physeal widening, fragmentation, displacement, dislocation, and radiocapitellar disease
- Ultrasound can show sub-apophyseal avulsive change but may be positive without symptoms
- MRI for persistent pain, unclear films, lateral symptoms, cartilage concern, or UCL complex concern
Management
- No displaced fracture: stop throwing, restore motion, rehabilitate kinetic chain, correct workload
- Return only when pain-free with full motion, restored strength, and staged throwing plan
- Avulsion fracture: assess displacement, stability, ulnar nerve, dislocation, and incarceration
- Minimally displaced fracture may be non-operative; displaced or unstable high-demand cases need specialist discussion
Exam Traps
- Do not call it adult UCL rupture first in an open-physis athlete
- Do not operate on imaging alone in an asymptomatic athlete
- Do not miss an incarcerated medial epicondyle fragment after elbow dislocation
- Do not return the child to the same workload that caused the injury
Evidence: Little League Elbow
Medial Epicondylar Abnormalities Track with Open Physis and Throwing Load
- Retrospective observational study of 506 elbows from athletes aged 19 years or younger presenting with elbow pain
- Osseous abnormalities were identified in 186 of 323 elbows with an open physis, compared with 19 of 183 elbows with a closed physis
- Abnormalities were observed in 204 of 409 throwing elbows compared with 1 of 97 nonthrowing elbows
- No osseous abnormalities were identified in nondominant elbows in the study cohort
Asymptomatic Youth Baseball Players Can Have Sub-apophyseal Avulsive Changes
- Ultrasound study of 65 male youth baseball players, evaluating 129 elbows with a mean age of 12.5 years
- Avulsive changes were observed in 23 of 64 dominant elbows, including avulsions and united avulsions
- No avulsive changes were seen in nondominant elbows
- Avulsion status was not associated with athlete characteristics, self-reported function, or pain with elbow palpation in this asymptomatic cohort
Medial Epicondylar Apophyseal Avulsion Fracture Is a Severe Variant
- Case series of 50 skeletally immature throwers with medial epicondylar apophyseal avulsion fracture
- Among patients with documentation, 31 of 37 reported pre-existing elbow pain before the acute injury
- Five of 12 patients who had shoulder examinations demonstrated glenohumeral internal rotation deficit
- Twenty-two patients underwent open reduction and internal fixation, 27 were treated non-operatively, and all patients returned to sports
- Each additional millimetre of displacement increased the odds of surgical intervention, and secondary screw removal occurred in 9 of 22 applicable ORIF patients
Pitch-Count Guidelines Alone Do Not Prevent Medial Elbow Changes
- Prospective cohort of 26 Little League players aged 10-13 with pre- and postseason bilateral elbow MRI
- Despite 100% compliance with pitch-count guidelines, 12 players (48%) developed abnormal MRI findings and 28% had in-season pain
- Distal humeral physeal width widened significantly over the season (1.54 to 2.31 mm) with an average 11-degree loss of shoulder internal rotation
- Pitch count, position and curveballs/sliders were NOT significantly associated with MRI change, but year-round play was