Exercise-Induced Leg Pain | Bone Stress Continuum | Training Errors | Activity Modification
- Clinical diagnosis - diffuse posteromedial tenderness exceeding 5cm length
- Continuum with stress fractures - same pathophysiology, different severity
- Training load errors are the most common modifiable risk factor
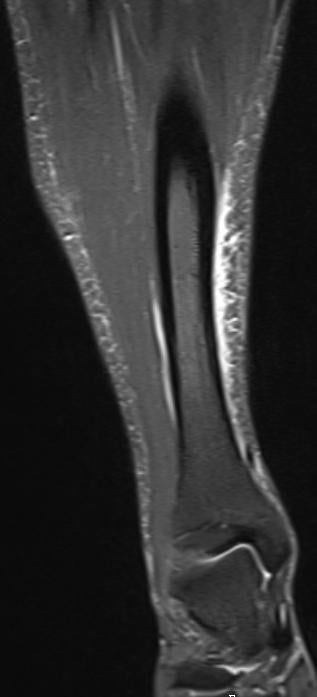
- MRI gold standard if imaging needed - shows periosteal/marrow edema
- Activity modification, not complete rest - evidence-based approach
- “MTSS pain improves with warm-up; stress fracture pain worsens with activity
- “Female athlete triad/RED-S must be screened in recurrent cases
- “Bone scan has high sensitivity but poor specificity for MTSS
- “Shock-wave therapy emerging as promising treatment modality
- MTSS is a CLINICAL diagnosis - imaging not required for typical presentations
- Diffuse tenderness over greater than 5cm of posteromedial tibial border
- Pain on palpation of the distal two-thirds of the medial tibial border
- Exclude stress fracture: focal tenderness, night pain, worsening with activity
- Traction periostitis from soleus, FDL, tibialis posterior insertions
- Bone stress reaction from repetitive bending loads on tibia
- Continuum from periosteal reaction through to cortical stress fracture
- Risk factors: training errors, biomechanics, low bone density, female sex
- MRI is GOLD STANDARD - periosteal and marrow edema visible
- X-ray usually normal but may show periosteal reaction chronically
- Bone scan: sensitive but NOT specific (high false positive rate)
- CT rarely indicated - better for established stress fractures
- Activity MODIFICATION not complete rest - pain-guided return
- Address training load errors - 10% rule for weekly increase
- Correct biomechanics: orthoses, footwear, gait retraining
- Screen for RED-S/female athlete triad in recurrent cases
Overview and Epidemiology
Medial tibial stress syndrome (MTSS), commonly known as "shin splints," is the most common cause of exercise-induced leg pain, affecting up to 35% of athletes at some point. It represents a stress reaction of the tibial cortex along the posteromedial border, existing on a continuum with tibial stress fractures. MTSS is a clinical diagnosis but understanding its relationship to stress fractures is critical for exam success.
MTSS vs tibial stress fracture exists on a continuum of bone stress injury:
- MTSS: Periosteal reaction, diffuse tenderness over greater than 5cm, pain that improves with exercise warm-up
- Stress fracture: Focal cortical involvement, point tenderness less than 5cm, pain that worsens with continued exercise
Both conditions share common risk factors (training errors, biomechanics, bone health) but management differs significantly.
Exercise-induced leg pain has several serious mimics:
Must exclude:
- Tibial stress fracture - point tenderness, worsening pain, risk of complete fracture
- Chronic exertional compartment syndrome - requires pressure testing
- Popliteal artery entrapment - vascular claudication, requires ABI/angiography
- Lumbar radiculopathy - dermatomal symptoms, neural tension signs
- Deep vein thrombosis - swelling, warmth, Homans sign
If symptoms are unilateral, focal, or include neurological/vascular features, investigate further before diagnosing MTSS.
Pathophysiology and Mechanisms
The posteromedial tibial border serves as the attachment site for multiple deep posterior compartment muscles:
- Soleus - via soleal line and middle third of tibia
- Flexor digitorum longus (FDL) - posterior tibia
- Tibialis posterior - interosseous membrane and posterior tibia
Repetitive traction from these muscles, combined with tibial bending stresses, causes periosteal reaction and bone stress injury at the posteromedial border - the classic "shin splints" location.
Tibial Anatomy
- Distal 2/3 most commonly affected
- Junction of posterior and medial tibial surfaces
- Direct subcutaneous position allows easy palpation
- Attachment of deep crural fascia
- Minimal soft tissue coverage
- Soleus - soleal line to middle tibia
- FDL - posterior tibial surface
- Tibialis posterior - interosseous membrane
- All exert traction force on periosteum
- Repetitive loading causes inflammation
Pathophysiology
- MTSS
- Diffuse (over 5cm)
- Stress Fracture
- Focal (under 5cm)
- MTSS
- Typically improves
- Stress Fracture
- Worsens with activity
- MTSS
- Uncommon
- Stress Fracture
- Common
- MTSS
- Periosteal edema only
- Stress Fracture
- Marrow edema + cortical line
- MTSS
- Usually normal
- Stress Fracture
- May show fracture line
- MTSS
- 6-8 weeks modification
- Stress Fracture
- 6-12 weeks rest
- MTSS
- Low with proper management
- Stress Fracture
- Risk of complete fracture
The classic teaching (and several mnemonics) call MTSS a traction periostitis from the soleus/FDL/tibialis posterior pulling on the periosteum - but the modern, examinable understanding has moved on, and this is exactly the kind of "do you know the current evidence?" point examiners probe:
- Histology does not support pure traction periostitis (Moen 2009, cited in this topic's evidence base). Instead, MTSS reflects a localised bone-stress/remodelling failure - osteoclastic resorption outpacing osteoblastic formation in the posteromedial tibial cortex under repetitive bending load. The periosteal oedema seen on MRI is the surface marker of this bony overload, not a primary tendinopathy.
- The muscle-attachment story is also debated: cadaveric work shows the tibialis posterior frequently does not even attach at the distal posteromedial site where MTSS pain occurs, and the soleus and the deep crural fascia are more consistent contributors. So "which muscle causes it" is less important than the bending-overload concept.
- Why this matters: framing MTSS as bone overload (not soft-tissue periostitis) is precisely why it sits on a single continuum with tibial stress fracture (same bone, same load mechanism, increasing severity) and why management targets load, bone health and energy availability rather than just stretching a muscle.
Exam point: if asked the mechanism, say MTSS is best understood as a bone-stress injury - resorption outpacing formation under repetitive tibial bending - on a continuum with stress fracture, and note that "traction periostitis" is an older, histologically-unsupported label.
Bone Stress Continuum
Classification Systems
The Fredericson classification grades tibial stress injuries on MRI. Higher grades correlate with longer recovery times and greater activity restriction. This is the most clinically useful system for guiding return-to-play timelines.
Grade 1 - Periosteal Edema Only:
- T2-weighted signal in periosteum only
- No marrow involvement
- Recovery: 2-3 weeks
- Management: Activity modification
Grade 2 - Periosteal + Marrow Edema (T2):
- Periosteal AND bone marrow edema on T2/STIR
- No T1 marrow signal change
- Recovery: 4-6 weeks
- Management: Reduce training load 50%
Grade 3 - Marrow Edema on All Sequences:
- Marrow edema visible on T1 AND T2 images
- More extensive marrow involvement
- Recovery: 6-9 weeks
- Management: Non-impact activity only
Grade 4a - Multiple Focal Cortical Changes:
- Multiple focal intracortical signal abnormalities
- No discrete fracture line
- Recovery: 9-12 weeks
- Management: Complete rest from running
Grade 4b - Cortical Fracture Line:
- Linear cortical fracture line visible
- Highest risk of progression
- Recovery: 12-16+ weeks
- Management: Protected weight bearing, possible surgery
Higher grades require progressively longer recovery periods.
GRADES
Fredericson MRI Classification
Hook:GRADES of stress injury - higher grade = longer recovery
- MRI Findings
- Periosteal edema only
- Recovery Time
- 2-3 weeks
- Management
- Activity modification
- MRI Findings
- Periosteal + marrow edema (T2)
- Recovery Time
- 4-6 weeks
- Management
- Reduce training load 50%
- MRI Findings
- Marrow edema T1 and T2
- Recovery Time
- 6-9 weeks
- Management
- Non-impact activity only
- MRI Findings
- Focal cortical abnormalities
- Recovery Time
- 9-12 weeks
- Management
- Complete rest from running
- MRI Findings
- Linear fracture line
- Recovery Time
- 12-16+ weeks
- Management
- Protected WB, possible surgery
Clinical Assessment
MTSS is diagnosed clinically. Key examination features:
Positive findings:
- Diffuse tenderness along posteromedial tibial border (greater than 5cm)
- Location: distal two-thirds of tibia most common
- Pain on resisted ankle plantarflexion or toe flexion (loads deep compartment)
Negative findings (should be absent):
- No focal "point" tenderness (suggests stress fracture)
- No neurological deficits (suggests radiculopathy)
- No vascular compromise (suggests PAES or DVT)
- No compartment fullness/pain with passive stretch (suggests CECS)
Physical Examination
- Diffuse posteromedial tenderness exceeding 5cm
- Tenderness along distal 2/3 of tibial border
- Pain with resisted plantarflexion
- Pain with single-leg hop (provocative test)
- May have slight palpable periosteal thickening
- Focal tenderness less than 5cm (stress fracture)
- Swelling of compartments (CECS or DVT)
- Neurological deficit (radiculopathy, nerve entrapment)
- Diminished pulses or claudication (vascular)
- Night pain, systemic symptoms (exclude tumor)
Differential Diagnosis
- Key Features
- Diffuse posteromedial tenderness, improves with warm-up
- Investigation
- Clinical diagnosis, MRI if needed
- Key Features
- Focal tenderness, worsens with activity, night pain
- Investigation
- MRI or bone scan
- Key Features
- Cramping/burning with exercise, resolves with rest
- Investigation
- Compartment pressure testing
- Key Features
- Claudication, diminished pulses with exercise
- Investigation
- ABI, duplex, angiography
- Key Features
- Swelling, warmth, calf tenderness
- Investigation
- D-dimer, duplex ultrasound
- Key Features
- Dermatomal symptoms, neural tension signs
- Investigation
- MRI lumbar spine
Investigations
MTSS is a clinical diagnosis - imaging is NOT required for typical presentations.
Indications for imaging:
- Diagnostic uncertainty (focal tenderness, atypical features)
- Failure to improve with 4-6 weeks of appropriate management
- High-level athlete needing accurate prognosis/timeline
- Concern for stress fracture progression
MRI is the gold standard - demonstrates periosteal edema, marrow edema, and fracture lines with high sensitivity and specificity.
Imaging Modalities
Findings: Usually NORMAL in MTSS
- May show periosteal reaction in chronic cases
- Stress fracture may show cortical irregularity, fracture line (late finding)
- Sensitivity less than 50% for stress injuries
Role: Primarily to exclude other pathology (tumor, infection)
Limitations: Cannot differentiate MTSS from early stress fracture
Laboratory Testing
Not routinely indicated for typical MTSS
Consider if:
- Recurrent stress injuries
- Suspected metabolic bone disease
- Female athlete triad/RED-S
- Systemic symptoms present
- Vitamin D (25-OH vitamin D)
- Calcium (serum and 24hr urine)
- PTH if calcium abnormal
- TSH for thyroid dysfunction
- Bone density (DEXA) if concern
Management
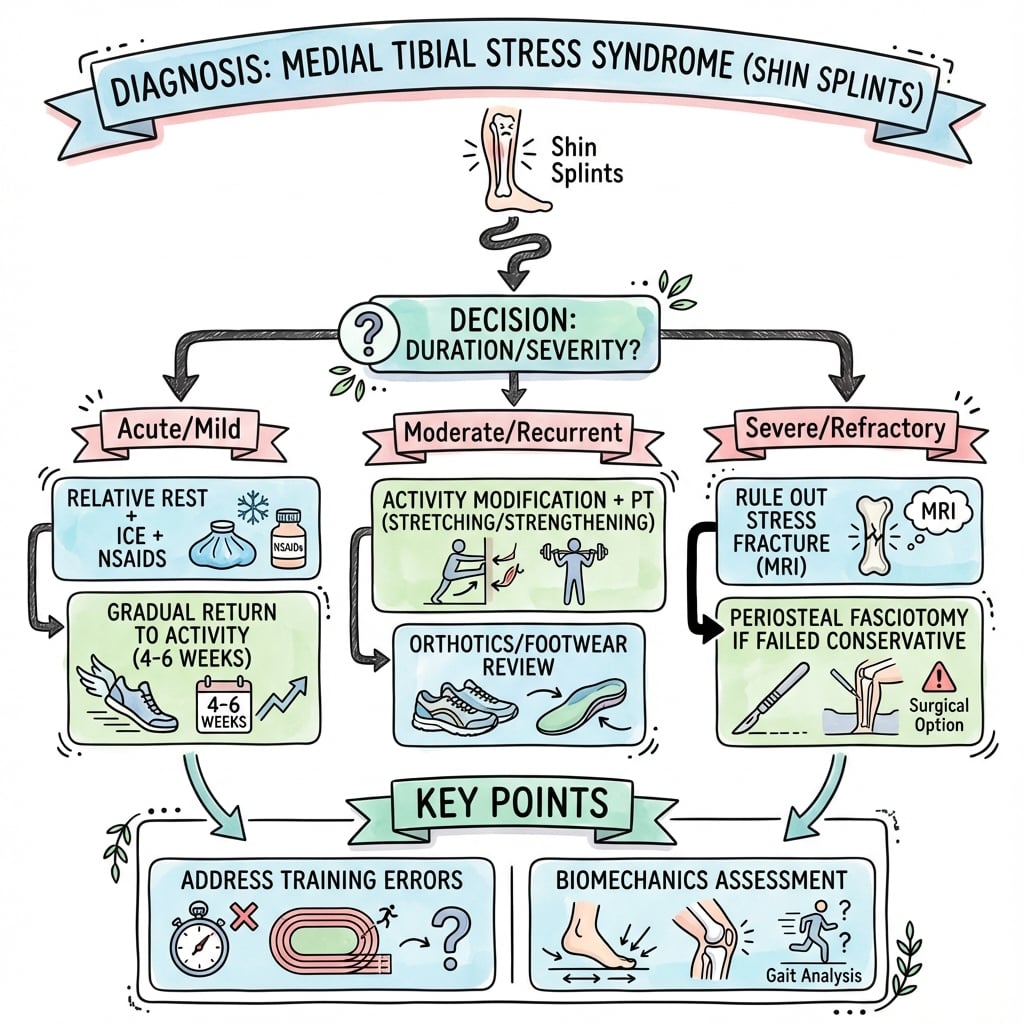
Modern MTSS management emphasizes activity modification rather than complete rest:
Key principles:
- Reduce load - decrease running volume/intensity, cross-train
- Address risk factors - training errors, biomechanics, footwear
- Pain-guided return - activities that don't cause pain during or after
- Screen for RED-S - energy availability, bone health, menstrual function
- Progressive return - gradual increase in impact activities
Complete rest is generally NOT recommended - it leads to deconditioning without addressing underlying factors.
Non-Operative Management
Immediate phase:
- Reduce running volume by 50-75%
- Avoid high-impact activities
- Cross-train: swimming, cycling, elliptical
Pain-guided return:
- Activity should not cause pain during exercise
- No pain within 2 hours after activity
- No pain next morning
If pain occurs, reduce load and progress more slowly
Return to Running Protocol
Surgical Technique
Surgical intervention for MTSS is rarely needed (less than 5% of cases) and reserved for refractory symptoms despite comprehensive conservative management. Most cases resolve with activity modification and addressing underlying risk factors.
Consider surgery only if:
- Persistent symptoms despite 6+ months of appropriate conservative treatment
- Significant impact on athletic or military career
- Documented fascial involvement on imaging (thickened deep posterior fascia)
- Failed trial of all non-operative options including biomechanical correction
- Patient understands variable success rates and rehabilitation requirements
Contraindications:
- Active training errors not addressed
- Underlying RED-S or bone health issues not optimized
- Unrealistic expectations
- Less than 6 months conservative management
Procedure:
- Release of deep posterior fascia overlying tibialis posterior and FDL
- Reduces traction on tibial periosteum
- Can be performed open or endoscopically
Technique:
- Longitudinal incision over posteromedial tibia
- Identify deep crural fascia
- Release fascia covering tibialis posterior and FDL
- Ensure complete release over symptomatic area
- Inspect periosteum (may cauterize if inflamed)
Evidence: Variable success rates (60-90% in small series)
Complications and Prevention
The primary concern with inadequately managed MTSS is progression to tibial stress fracture:
Risk factors for progression:
- Continued training through pain
- Failure to address training load errors
- Underlying low energy availability (RED-S)
- Low bone density
- Female sex
Prevention: Pain-guided activity modification and addressing modifiable risk factors prevents progression in the vast majority of cases.
The topic repeatedly notes that anterior tibial cortex fractures are "high-risk" - here is why, because this is the single most important distinction once MTSS progresses to a frank stress fracture:
- Posteromedial (compression side) = LOW risk. Typical MTSS-continuum stress fractures sit on the posteromedial tibia, which is the compression side of the bending tibia and is well-vascularised - these heal reliably with load modification.
- Anterior mid-diaphyseal cortex = HIGH risk. The anterior tibial cortex is the tension side of the bending tibia and is relatively hypovascular, so fractures here are prone to delayed union, non-union, progression to complete (sometimes displaced) fracture, and recurrence. The radiographic hallmark is the "dreaded black line" - a transverse anterior cortical lucency, often with cortical hypertrophy around it.
- Management differs accordingly: a true anterior-cortex high-risk stress fracture often does not reliably respond to rest alone and may require prolonged protected loading, bone-stimulation/optimisation, or surgical intramedullary nailing - quite unlike the conservative pathway for posteromedial MTSS.
Exam point: when shin pain progresses to a stress fracture, localise the cortex - posteromedial (compression) is low-risk and conservative, while an anterior "dreaded black line" (tension side, hypovascular) is high-risk for non-union/complete fracture and frequently needs intramedullary nailing.
Prevention Strategies
- Training errors - sudden volume/intensity increases
- Footwear - worn shoes, inappropriate for foot type
- Surface - excessive hard surface running
- Biomechanics - overpronation, muscle imbalances
- Energy availability - inadequate nutrition
- Female sex (3x higher risk)
- Previous MTSS history
- Bone density (genetic component)
- Tibial anatomy (narrow diaphysis)
- Age (peak in young adults)
Postoperative Care and Rehabilitation
Following surgical fasciotomy for refractory MTSS, rehabilitation focuses on gradual return to loading while allowing fascial healing and addressing underlying biomechanical factors that contributed to the initial problem.
Goals:
- Wound healing
- Control swelling
- Maintain ankle ROM
- Prevent complications
Activities:
- Protected weight bearing with crutches
- Elevation when resting
- Ice therapy 3-4 times daily
- Ankle pumps and circles
- Gentle active ROM within pain limits
Precautions:
- No impact activities
- Monitor wound for infection
- Keep surgical site clean and dry
Focus on wound healing and swelling control.
Outcomes and Prognosis
With appropriate management, MTSS has an excellent prognosis:
- 85-90% resolve with conservative management
- Average recovery time: 6-8 weeks with activity modification
- Recurrence rate: 20-30% if underlying factors not addressed
- Progression to stress fracture: less than 10% with appropriate load management
- Surgical intervention needed: less than 5% of cases
- Early recognition and management
- Good compliance with activity modification
- Address of training errors
- Correction of biomechanical issues
- Adequate energy availability
- No previous stress fracture history
- Male gender
- Continued training through pain
- Multiple recurrences
- Underlying RED-S or low bone density
- Anterior tibial location (higher fracture risk)
- Failure to address biomechanics
- Poor training load management
- Concomitant stress fracture
- Conservative Management
- Activity modification 25-50%
- Expected Recovery
- 3-4 weeks
- Return to Sport
- 4-6 weeks
- Conservative Management
- Activity modification 50-75%
- Expected Recovery
- 6-8 weeks
- Return to Sport
- 8-10 weeks
- Conservative Management
- Significant load reduction
- Expected Recovery
- 8-12 weeks
- Return to Sport
- 12-16 weeks
- Conservative Management
- Complete rest from impact
- Expected Recovery
- 12-16+ weeks
- Return to Sport
- 16-20+ weeks
- Conservative Management
- Comprehensive management ± surgery
- Expected Recovery
- Variable, 3-6 months
- Return to Sport
- 6-9 months
Incidence and Risk Factors in Naval Recruits
- Prospective cohort of 124 naval recruits over a 10-week basic training period
- MTSS incidence 35% (40 of 124 recruits affected)
- Female recruits affected 53% versus 28% in males (relative risk 2.03)
- Pronated foot type associated with MTSS (relative risk 1.70)
- Identifying pronation pre-training may enable preventive intervention
Return to Sport Timeline
Guidelines, Registries & Global Practice
Global Epidemiology
MTSS is consistently the most common exercise-induced leg injury worldwide, but reported frequency varies with population and case definition.
- Reported figure
- 4-35%
- Source
- Moen 2009 critical review (PMID 19530750)
- Reported figure
- 35% overall incidence
- Source
- Yates & White 2004 (PMID 15090396)
- Reported figure
- 53% vs 28% (RR 2.03)
- Source
- Yates & White 2004 (PMID 15090396)
- Reported figure
- RR 1.70 for MTSS
- Source
- Yates & White 2004 (PMID 15090396)
According to PubMed, the female predominance and the role of foot pronation are reproducible across prospective military cohorts (Yates & White 2004, PMID 15090396, DOI; Moen 2009, PMID 19530750, DOI).
Guideline & Consensus Positions
There is no single dedicated AAOS/NICE/BOA clinical practice guideline for MTSS; practice is shaped by sports-medicine consensus statements and systematic reviews. The table below summarises authoritative positions and their evidence strength.
- Position on MTSS
- No active treatment proven; ESWT most promising; manage load/risk factors
- Evidence basis
- Level I review of Level 3-4 trials
- Position on MTSS
- Rest equals other interventions; orthoses may prevent; clinical diagnosis primary
- Evidence basis
- Level II review
- Position on MTSS
- Screen recurrent bone stress injury for the Female Athlete Triad / low energy availability
- Evidence basis
- Expert position stand (Level V)
- Position on MTSS
- Clinical algorithm; positive hop test plus focal tenderness signals stress fracture; image only if no response to rest
- Evidence basis
- Prospective validation cohort
Registry & Prospective-Cohort Evidence
MTSS is not captured by joint-replacement registries (AOANJRR/NJR/AJRR); the equivalent population-level evidence comes from military training cohorts, which provide the most robust incidence and prevention data.
Gait Retraining Reduces MTSS Incidence (RCT)
- RCT in 166 at-risk British Army recruits during 26-week basic training
- Supervised gait retraining plus neuromuscular exercise versus usual training
- Adjusted hazard ratio for MTSS 0.25 (95% CI 0.05-0.53)
- Number needed to treat 14 to prevent one additional injured recruit at 20 weeks
Clinical Differentiation of Stress Fracture from MTSS (IDF Protocol)
- Prospective validation of the Israel Defense Forces medial tibial stress fracture protocol in 429 elite infantry recruits
- A positive hop test with focal tibial tenderness strongly predicted stress fracture (odds ratio 52.0)
- Stress fracture occurred when the band of tenderness was 10cm or less; diffuse tenderness favoured MTSS
- A clinical, imaging-free initial rest protocol resolved more than two-thirds of suspected cases
Practice Variation Across Health Systems
- Common international practice
- Clinical across all systems; imaging reserved for atypical or non-responding cases
- Common international practice
- MRI preferred globally where accessible; bone scan still used where MRI access is limited
- Common international practice
- Load modification and risk-factor correction universal; ESWT used in better-resourced settings for refractory cases
- Common international practice
- A leading driver of training time-loss and medical downgrading in military recruits; UK, Israeli and Australian programmes use gait retraining and graduated loading to reduce incidence
Essential Mnemonics
STRESS
Pathophysiology of MTSS
Hook:The STRESS on your shins - what causes shin splints!
SPLINTS
History for Shin Pain
Hook:SPLINTS history - shin pain is not always shin splints!
MODIFY
MTSS Treatment Approach
Hook:MODIFY the approach - don't just rest!
PREVENT
MTSS Prevention
Hook:PREVENT shin splints before they happen!
SHINS
MTSS Quick Diagnosis
Hook:Sore SHINS - the classic shin splints features!
FRACTURE
Stress Fracture Red Flags
Hook:FRACTURE - the red flags that distinguish stress fracture from MTSS!
MCQ Practice Points
Q: What is the characteristic clinical finding that distinguishes MTSS from tibial stress fracture? A: Diffuse tenderness over greater than 5cm of the posteromedial tibial border. Point tenderness less than 5cm suggests stress fracture.
Q: What is the gold standard imaging modality for suspected MTSS? A: MRI - demonstrates periosteal edema on T2/STIR sequences. X-rays are usually normal in MTSS.
Q: What is the underlying mechanism of MTSS? A: Traction periostitis from soleus, FDL, and tibialis posterior muscles combined with repetitive tibial bending loads causing periosteal reaction at the posteromedial border.
Q: What is the key management principle for MTSS? A: Activity modification (not complete rest) with pain-guided return to activity. The 10% rule limits weekly training increase.
Q: What is the most common modifiable risk factor for MTSS? A: Training errors (sudden increase in volume, intensity, or change in running surface). Female sex increases risk 3-fold but is non-modifiable.
- MTSS is a clinical diagnosis - imaging not required
- Diffuse tenderness over greater than 5cm posteromedial tibial border
- Pain improves with warm-up (vs stress fracture worsens)
- Distal 2/3 of tibia most commonly affected
- Single-leg hop test provocative
- Must exclude stress fracture if focal tenderness
- Traction periostitis from soleus, FDL, tibialis posterior
- Bone stress continuum with stress fractures
- Repetitive tibial bending loads
- Periosteal reaction on histology
- NOT purely muscular origin
- Same risk factors as stress fractures
- MRI is gold standard for imaging
- Periosteal edema on T2/STIR sequences
- X-ray usually normal in MTSS
- Bone scan: sensitive but NOT specific
- Fredericson classification grades severity
- CT has limited role in MTSS
- Female sex increases risk 3-fold
- Training errors most common modifiable factor
- Previous MTSS history
- Overpronation of foot
- Low BMI and RED-S
- Hard running surfaces
- Activity MODIFICATION not complete rest
- Pain-guided return to activity
- 10% rule for weekly training increase
- Address biomechanics and footwear
- Screen for RED-S in recurrent cases
- Surgery rarely indicated (under 5%)
- 85-90% resolve conservatively
- Average recovery 6-8 weeks
- Recurrence 20-30% if factors not addressed
- Progression to fracture under 10%
- Excellent long-term prognosis
- Return to pre-injury level in 87%
Common MCQ Scenarios
- Most Likely Diagnosis
- MTSS
- Next Best Investigation
- None - clinical diagnosis
- Definitive Management
- Activity modification 50%, biomechanics
- Most Likely Diagnosis
- Tibial stress fracture
- Next Best Investigation
- MRI tibia
- Definitive Management
- Complete rest from impact, protected WB
- Most Likely Diagnosis
- MTSS with RED-S
- Next Best Investigation
- DEXA scan, vitamin D, menstrual workup
- Definitive Management
- Increase energy availability, MDT approach
- Most Likely Diagnosis
- Refractory MTSS
- Next Best Investigation
- MRI to exclude stress fracture
- Definitive Management
- Consider ESWT or surgical fasciotomy
- Most Likely Diagnosis
- Fredericson Grade 1
- Next Best Investigation
- None - confirms MTSS
- Definitive Management
- Activity modification 2-3 weeks
Key Numbers for MCQs
At a Glance Table
- MTSS
- Diffuse (greater than 5cm)
- Tibial Stress Fracture
- Focal (less than 5cm)
- MTSS
- Posteromedial tibial border
- Tibial Stress Fracture
- Any cortex (anterior higher risk)
- MTSS
- Typically improves
- Tibial Stress Fracture
- Worsens with activity
- MTSS
- Uncommon
- Tibial Stress Fracture
- Common
- MTSS
- Periosteal reaction
- Tibial Stress Fracture
- Cortical stress reaction/fracture
- MTSS
- Usually normal
- Tibial Stress Fracture
- May show fracture line/periosteal reaction
- MTSS
- Periosteal edema only
- Tibial Stress Fracture
- Marrow edema + cortical involvement
- MTSS
- 6-8 weeks
- Tibial Stress Fracture
- 12-16+ weeks (depends on grade)
- MTSS
- Activity modification
- Tibial Stress Fracture
- Complete rest from impact
- MTSS
- Progression to stress fracture
- Tibial Stress Fracture
- Complete fracture
- Most common overuse leg injury
- 13-17% of running injuries
- Up to 35% prevalence in athletes
- Female runners 3x higher risk
- Peak incidence: 18-25 years
- Training errors - sudden increase in load
- Female gender (lower bone density)
- Overpronation of foot
- Low BMI and relative energy deficiency
- Previous MTSS history
- Diffuse tenderness posteromedial tibial border
- Pain length typically exceeds 5cm (vs stress fracture)
- Pain improves with warm-up initially
- Clinical diagnosis - imaging not always needed
- Rule out compartment syndrome if atypical
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old female runner presents with 4 weeks of bilateral leg pain. Examination shows diffuse tenderness along the posteromedial tibial borders. She's training for a marathon and recently increased her weekly mileage. How do you approach this case?”
“A 19-year-old male soldier presents with right leg pain worsening over 3 weeks of infantry training. Examination shows focal tenderness over a 2cm area of the mid-tibial shaft. What is your approach?”
“A 17-year-old female cross-country runner has recurrent bilateral shin pain despite two previous periods of rest. She has irregular periods and is underweight. How do you manage this complex case?”
Key Numbers
- **35%** - Athletes affected at some point
- **5cm** - Tenderness length distinction (MTSS greater than 5cm, stress fracture less than 5cm)
- **3x** - Female sex increases risk
- **6-8 weeks** - Typical MTSS recovery
- **12+ weeks** - Stress fracture (Grade 4) recovery
- **10%** - Maximum weekly training increase (prevention)
- **50%** - Load reduction recommended in acute MTSS
Clinical Diagnosis
- Diffuse posteromedial tibial tenderness (greater than 5cm)
- Distal 2/3 of tibia most commonly affected
- Pain IMPROVES with warm-up (vs stress fracture worsens)
- No focal point tenderness (that's stress fracture)
- Positive single-leg hop test
- Clinical diagnosis - imaging NOT required for typical cases
Fredericson MRI Classification
- **Grade 1**: Periosteal edema only - 2-3 week recovery
- **Grade 2**: Periosteal + marrow edema (T2) - 4-6 weeks
- **Grade 3**: Marrow edema T1 AND T2 - 6-9 weeks
- **Grade 4a**: Focal cortical abnormalities - 9-12 weeks
- **Grade 4b**: Linear fracture line - 12-16+ weeks
Critical Differentials
- **Tibial stress fracture** - focal tenderness, worsening pain
- **CECS** - compartment fullness, pressure testing diagnostic
- **Popliteal artery entrapment** - claudication, vascular testing
- **Lumbar radiculopathy** - dermatomal symptoms
- **DVT** - swelling, warmth
Management Principles
- Activity MODIFICATION not complete rest
- Pain-guided return (no pain during, after, or next morning)
- Address training errors (10% weekly increase maximum)
- Footwear/orthoses for overpronation
- Cross-train to maintain fitness
- Screen for RED-S in recurrent cases
Viva Buzzwords
- 'Bone stress continuum'
- 'Traction periostitis'
- 'Pain-guided return to activity'
- 'Relative energy deficiency in sport (RED-S)'
- 'Fredericson classification'
- 'Activity modification preferred over complete rest'
Evidence Base
Fredericson MRI Grading System (Landmark)
- Defined a progression of tibial stress injury: periosteal oedema then marrow involvement then cortical stress fracture
- Introduced the MRI grading system that correlated with technetium bone-scan grading and symptoms
- MRI more accurately localised and graded injury than bone scan, without ionising radiation
- Recommended MRI over bone scan for grading tibial stress lesions in runners
MTSS Pathophysiology and Risk Factors (Critical Review)
- Reported incidence of MTSS between 4% and 35% in military personnel and athletes
- Histology does not support traction periostitis - MTSS reflects bony resorption outpacing formation in the tibial cortex
- Excessive standing foot pronation and female sex are intrinsic risk factors across multiple prospective studies
- Previous history of MTSS is an established risk factor
- In randomised studies rest was equal to other interventions; neoprene or semi-rigid orthoses may aid prevention
Treatment of MTSS - Systematic Review
- Eleven trials reviewed; all RCTs carried a high risk of bias (Level 3 evidence) and non-randomised trials were poor quality (Level 4)
- No single treatment is sufficiently free of methodological bias to be recommended
- Lower-leg braces and iontophoresis showed no significant benefit on pooled analysis
- Extracorporeal shockwave therapy (ESWT) appeared to have the most promise of the interventions examined
- Low-level laser, stretching/strengthening, compression stockings and pulsed electromagnetic fields were not proven effective
Shockwave Therapy for Chronic Recalcitrant MTSS
- Case-control cohort: 47 patients had radial low-energy shockwave therapy plus home training versus 47 controls with home training alone
- Success rate at 15 months 76% (ESWT) versus 37% (control), p less than 0.001
- Mean numeric rating scale at 15 months 2.7 (ESWT) versus 5.3 (control)
- 40 of 47 ESWT patients returned to preferred sport at pre-injury level versus 22 of 47 controls
Female Athlete Triad - ACSM Position Stand
- Defines the Triad as the interrelationship of energy availability, menstrual function and bone mineral density
- Low energy availability (below ~30 kcal/kg fat-free mass/day) is the central driver impairing reproductive and skeletal health
- Athletes should be screened at pre-participation and annual exams and whenever a Triad condition appears
- First aim of treatment is to increase energy availability via intake and/or reduced expenditure, with a multidisciplinary team