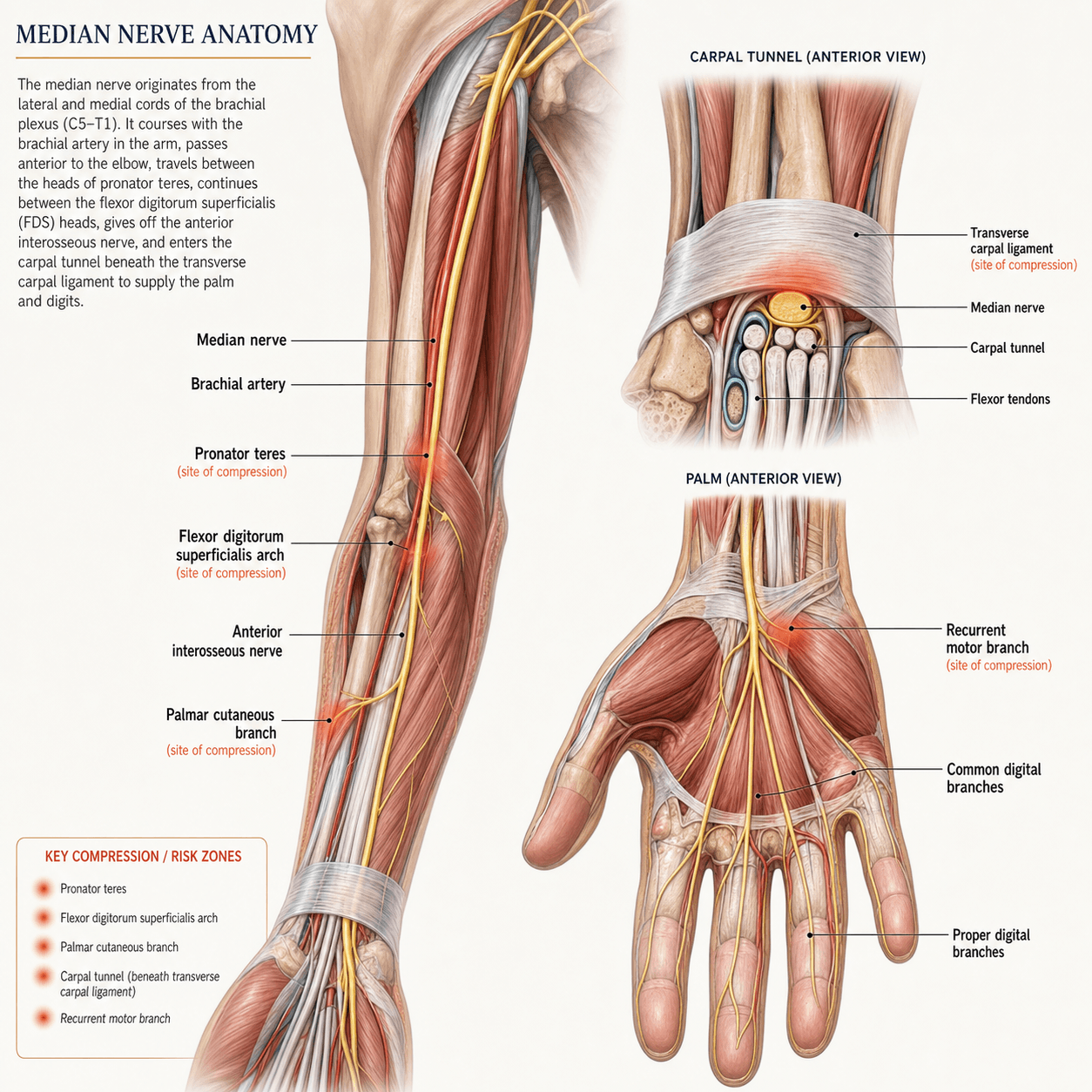
The Laborer's Nerve (Coarse Power and Sensation)
- Formed by Lateral (C5-7) and Medial (C8-T1) Cords
- Runs MEDIAL to Brachial Artery in Cubital Fossa (TAN: Tendon, Artery, Nerve)
- Supplies Flexor Compartment of Forearm (Except FCU + Ulnar 1/2 FDP)
- Supplies LOAF muscles in hand (Lumb 1/2, Opponens, APB, FPB-sup)
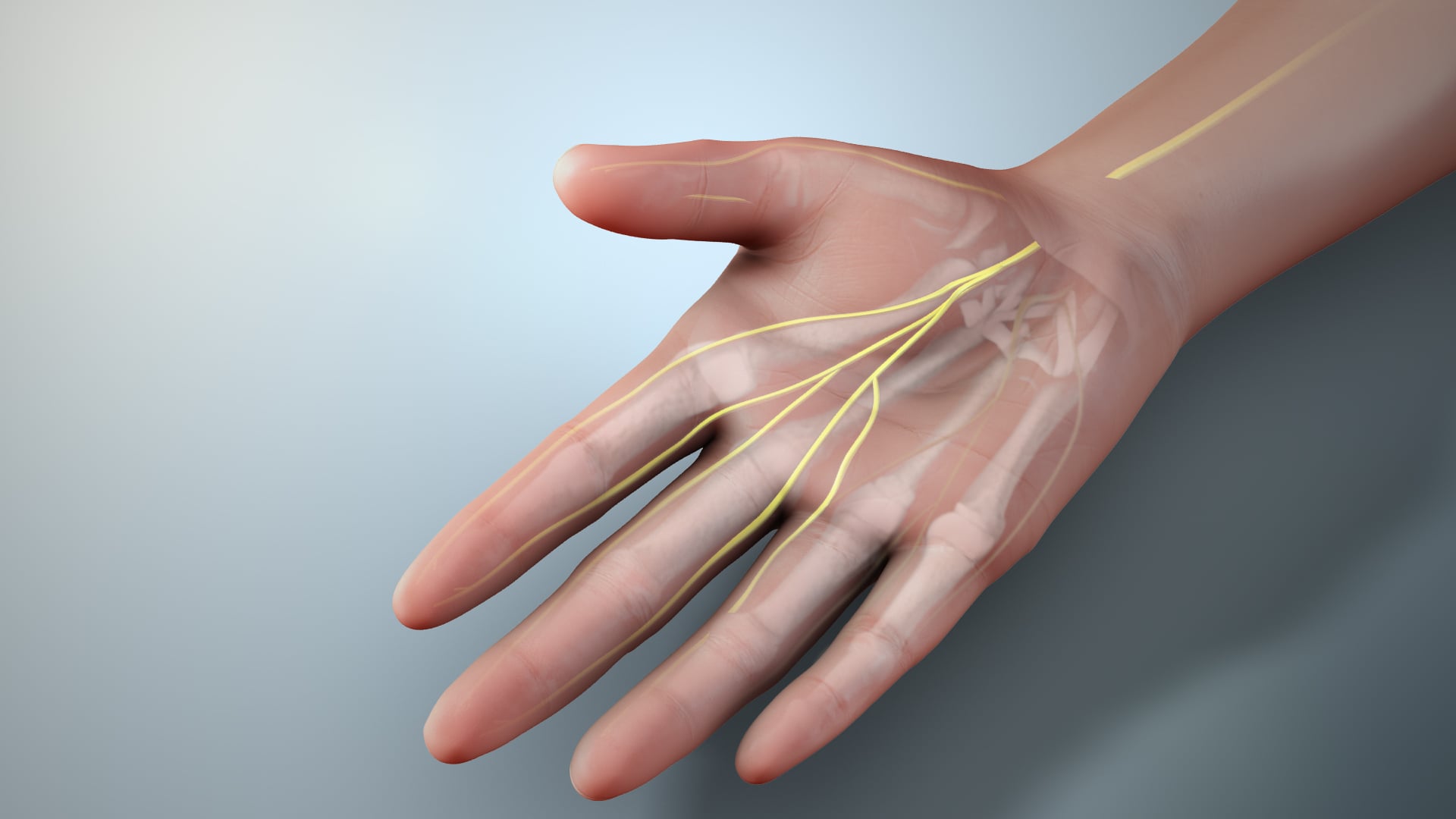
- Sensation to Radial 3.5 digits (Palmar)
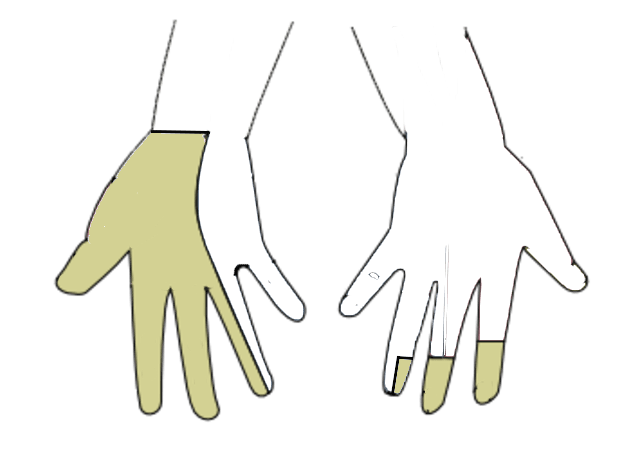
- “Hand of Benediction (High Median) is an ACTIVE sign (trying to fist)
- “Ulnar Claw (Low Ulnar) is a PASSIVE sign (at rest)
- “Palmar Cutaneous Branch is SPARED in Carpal Tunnel (arises proximal)
- “AIN is purely MOTOR (No sensory loss, just 'OK' sign fail)
High Median Palsy. Patient tries to make a fist.
- Index/Middle FDP + FDS paralyzed → Cannot flex.
- Ring/Little FDP intact (Ulnar) → Flex.
- Result: Index/Middle straight, others flexed. Active Sign.
Low Ulnar Palsy. Patient at rest.
- Intrinsics paralyzed (Lumb 3/4, Interossei).
- MCPs hyperextend (EDC), IPs flex (FDP).
- Result: Ring/Little clawed. Passive Sign.
- Motor Function
- Pronator, FCR, FDS, PL
- Sensory Area
- Palm + Digits
- Key Sign
- Benediction Hand
- Motor Function
- FPL, FDP (Idx/Mid), PQ
- Sensory Area
- None (Joint prop only)
- Key Sign
- Cannot make 'OK' sign
- Motor Function
- None
- Sensory Area
- Thenar Eminence / Palm
- Key Sign
- Spared in CTS
- Motor Function
- LOAF Muscles
- Sensory Area
- None
- Key Sign
- Thenar Wasting
PACSubtypes of Median Nerve Injury
Hook:PAC-Man eats the median nerve.
TANCubital Fossa Contents
Hook:TAN your arm from Lateral to Medial.
LOAFThenar Muscles (LOAF)
Hook:The loaf of bread in your hand.
Overview
The Median Nerve is the "Eye of the Hand" (sensory to thumb/index) and the "Laborer's Nerve" (power grip via FDS/FDP/Thenar).
Neurovascular
Axilla & Arm
- Formed effectively by the fusion of Lateral (C5-7) and Medial (C8-T1) cords.
- No branches in the arm.
- Runs with Brachial Artery. First lateral, then crosses to medial.
Elbow (Cubital Fossa)
- Passes under the Bicipital Aponeurosis (Lacertus Fibrosus).
- Compression site: Lacertus Syndrome.
- Lies Medial to the Brachial Artery ("TAN").
- Enters forearm between the two heads of Pronator Teres.
- Compression site: Pronator Syndrome.
The nerve is vulnerable at these multiple fibrous arches.
The Lacertus Fibrosus (Bicipital Aponeurosis) originates from the Biceps tendon and inserts into the ulna. It covers the median nerve and brachial artery. In bodybuilders or laborers, a thickened lacertus can compress the nerve, mimicking pronator syndrome.
Branching Order (Proximal to Distal)
- Level
- Arm
- Function
- None
- Clinical Relevance
- High palsy spares nothing below
- Level
- Elbow
- Function
- Pronation
- Clinical Relevance
- First motor branch
- Level
- Proxi Forearm
- Function
- Wrist Flexion
- Clinical Relevance
- Tendon transfer donor
- Level
- Proxi Forearm
- Function
- Fascia tensor
- Clinical Relevance
- Graft harvest
- Level
- Mid Forearm
- Function
- PIP Flexion
- Clinical Relevance
- Independent function
- Level
- Mid Forearm
- Function
- DIP/IP Flexion
- Clinical Relevance
- OK Sign / Pinch
- Level
- Distal Forearm
- Function
- Palm Sensation
- Clinical Relevance
- Spared in CTS
- Level
- Hand (Tunnel)
- Function
- Thenar Motor
- Clinical Relevance
- Million Dollar Nerve
- Level
- Hand
- Function
- Sensation 3.5
- Clinical Relevance
- Numbness in CTS
The carpal tunnel is an osseofibrous canal — the examiner expects its walls, not just its contents:
- Roof: the flexor retinaculum (transverse carpal ligament), spanning the carpal arch.
- Floor and sides: the concave arch of the carpal bones.
- Radial attachments of the retinaculum: the tubercle of the scaphoid and the ridge of the trapezium.
- Ulnar attachments: the pisiform and the hook of the hamate.
It transmits 10 structures: the median nerve plus 9 flexor tendons (4 FDS, 4 FDP, 1 FPL). Guyon's canal lies superficial and ulnar to the retinaculum and is a separate compartment, so the ulnar nerve is not in the carpal tunnel. Because the canal is a rigid box, anything that raises its volume (tenosynovitis, a mass, fluid in pregnancy) or reduces its capacity (a distal radius malunion) raises the pressure on the nerve.
Classification Systems
Carpal Tunnel Syndrome Severity (Neurophysiology)
- Sensory (SNAP)
- Slowed / Reduced Amp
- Motor (CMAP)
- Normal
- EMG
- Normal
- Sensory (SNAP)
- Absent / Severe Slowing
- Motor (CMAP)
- Delayed Latency
- EMG
- Normal / Mild changes
- Sensory (SNAP)
- Absent
- Motor (CMAP)
- Reduced Amp / Absent
- EMG
- Denervation (Fibs/Pos waves)
Clinical Assessment
- Wrist flexion for 60 seconds.
- Compresses nerve.
- Positive if paresthesia reproduced in digits.
- Reverse Phalen's: Wrist extension (increases pressure even more).
- Percussion over nerve.
- Wrist: CTS.
- Proximal Forearm/Elbow: Pronator Syndrome.
- Direct compression over carpal tunnel for 30s.
- Most sensitive test for CTS.
- Ask patient to make an 'O' with thumb and index.
- Normal: Tip-to-Tip pinch (FPL + FDP active).
- AIN Palsy: Pulp-to-Pulp pinch (Posterior pinch). FPL/FDP failed, Adductor/FDS compensate.
Differential Diagnosis Matrix
- Night Pain
- Yes (Classic)
- Sensory Loss
- Digits 1-3.5
- Motor Weakness
- APB (Thenar)
- Night Pain
- Rare (Activity related)
- Sensory Loss
- Palm + Digits
- Motor Weakness
- FPL/FDP/APB
- Night Pain
- Deep forearm ache
- Sensory Loss
- None
- Motor Weakness
- FPL/FDP (OK sign)
- Night Pain
- Neck pain
- Sensory Loss
- Thumb/Index (Dermatome)
- Motor Weakness
- Biceps/Wrist Ext
Examination Pearls
Motor Testing (Detailed)
- OK Sign (AIN): FPL/FDP. Look for "tear drop" (Pulp-to-Pulp).
- Abduction (APB): "Touch the ceiling". Palpate muscle belly to exclude trick movement (PL/EPL).
- Opposition (Opponens): "Touch pin to thumb".
- FDS Test: Hold other fingers in extension.
- FDP Test: Hold PIP in extension.
Sensory Maps
- Autonomous Zone: Tip of Index Finger.
- Splitting: Radial 1/2 of Ring Finger.
- Palm: Proximal to wrist crease (PCB).
Provocative Tests Sensitivity
- Sensitivity
- 89%
- Specificity
- 90%
- Notes
- Most accurate manual test
- Sensitivity
- 68%
- Specificity
- 73%
- Notes
- Less specific in elderly
- Sensitivity
- 50%
- Specificity
- 77%
- Notes
- Great for tracking axon regeneration
Investigations
Nerve Conduction Studies
- Indications: atypical symptoms, atrophy, revision, workers comp.
- Findings:
- Increased distal motor latency (greater than 4.2ms).
- Decreased sensory conduction velocity.
- Comparison: Compare to Ulnar/Radial (4th digit double innervation) to rule out polyneuropathy.
NCS is the gold standard for grading severity.
Management Strategy
Carpal Tunnel Syndrome
- Conservative:
- Night splints (neutral).
- Steroid injection (Diagnostic & Therapeutic).
- Ergonomics.
- Surgical:
- Indications: Failure of conservative, constant numbness, thenar wasting.
- Procedure: Carpal Tunnel Release (Open or Endoscopic).
Surgery is highly effective for night symptoms.
Management Algorithm
- First Line
- Splint / NSAIDs
- Second Line
- Steroid Injection
- Surgery Indication
- Failed conservative over 3m
- First Line
- Injection + Splint
- Second Line
- Consider early surgery
- Surgery Indication
- Patient preference / Failure
- First Line
- Surgery (Release)
- Second Line
- None
- Surgery Indication
- Relative Emergency (prevent permanent loss)
- First Line
- Reduction of fracture
- Second Line
- Release if persistent
- Surgery Indication
- Compartment Syndrome equivalent
Surgical Technique
Open Carpal Tunnel Release
Procedure Steps
Incision in line with ring finger axis. Distal to Kaplan's Cardinal Line. Avoid Palmer Cutaneous Branch (ulnar to PL tendon).
Incise Palmar Fascia. Identify distal edge of Transverse Carpal Ligament (TCL).
Divide TCL ulnarly to protect Recurrent Branch (radial). Visualize fat pad distally (Superficial Palmar Arch). Release proximally into forearm fascia.
The Recurrent Motor Branch has variable anatomy. In 50% it is Extraligamentous. In ~30% Subligamentous. In ~20% Transligamentous (goes THROUGH the ligament). Always cut the ligament on the ULNAR side.
Meticulous hemostasis is required to prevent hematoma and scarring.
Complications
- Cause
- Loss of arch support/ligament healing
- Management
- Time, padding (Resolves by 6m)
- Cause
- Flexor retinaculum intact proximally
- Management
- Revision
- Cause
- Radial side incision
- Management
- Repair / Tendon Transfer
- Cause
- Nerve injury / idiopathis
- Management
- Multimodal therapy
Rehabilitation
- Splinting: Generally NOT required for simple CTR.
- Motion: Immediate finger and wrist ROM.
- Strengthening: Grip strengthening at 4-6 weeks.
- Return to work: Desk (1-2 weeks), Light Manual (4 weeks), Heavy (6-8 weeks).
Early mobilization reduces complex regional pain syndrome risk.
Rehabilitation Protocol
- Timeframe
- 0-2 Weeks
- Goals
- Wound healing, Edema mgt
- Precautions
- Avoid heavy grip
- Timeframe
- 2-6 Weeks
- Goals
- Tendon gliding, Scar massage
- Precautions
- Desensitization
- Timeframe
- 6+ Weeks
- Goals
- Work hardening, Grip strength
- Precautions
- Return to sport
Specific Exercises
- Nerve Gliding: "Median Nerve Flossing".
- Position 1: Fist.
- Position 2: Extend fingers.
- Position 3: Extend wrist.
- Position 4: Supinate.
- Position 5: Stretch thumb.
- Tendon Gliding: Hook fist, Straight fist, Full fist.
Outcomes
- Success: 90% good/excellent results for CTS release.
- Night Pain: Resolves almost immediately ("Best sleep in years").
- Numbness: Variable recovery. Permanent if long-standing.
- Recurrence: Rare (less than 5%). Look for scarring, missed diagnosis, or double crush.
Guidelines, Registries & Global Practice
Global Epidemiology
- Carpal tunnel syndrome is the most common compressive neuropathy worldwide; population-based data (Atroshi et al., JAMA 1999) show clinically and electrophysiologically confirmed prevalence of about 2.7%, with median-distribution hand symptoms in roughly 14% of adults.
- Female predominance (approx 3:1 to 4:1), peak incidence in the 4th to 6th decades, and rising prevalence with obesity, diabetes, pregnancy, hypothyroidism and rheumatoid disease.
- Anterior interosseous nerve and pronator syndromes are rare by comparison and are frequently inflammatory (neuralgic amyotrophy) rather than purely compressive.
Side-by-Side Guideline Comparison
- Diagnosis
- Clinical criteria + provocative tests
- Electrodiagnostics
- Recommended before surgery if diagnosis uncertain
- Surgery
- Complete division of transverse carpal ligament; open or endoscopic equivalent
- Diagnosis
- Clinical, supported by validated questionnaires (e.g. CTS-6, Boston)
- Electrodiagnostics
- Not mandatory in classic cases; used when atypical or for medicolegal/work claims
- Surgery
- Decompression after failed/declined conservative care
- Diagnosis
- Clinical diagnosis; ultrasound increasingly used
- Electrodiagnostics
- Selective use
- Surgery
- Steroid injection then surgery; avoids routine NCS
- Diagnosis
- Clinical-first; imaging adjunctive
- Electrodiagnostics
- Confirmatory, not universally required
- Surgery
- Standardised release with recurrent-branch protection
Registry and Outcome Data
- Large administrative cohorts and hand-surgery registries consistently report carpal tunnel release as one of the highest-volume, highest-satisfaction elective hand procedures, with revision rates under 5%.
- There is no implant, so arthroplasty registries (NJR, AJRR, AOANJRR) do not apply; outcome surveillance relies on PROMs such as the Boston Carpal Tunnel Questionnaire and QuickDASH.
High- vs Limited-Resource Practice Variation
- Well-resourced settings: Liberal access to nerve conduction studies and high-resolution ultrasound; endoscopic release and wide-awake local-anaesthetic no-tourniquet (WALANT) open release are both common.
- Limited-resource settings: Diagnosis is predominantly clinical; open release under WALANT in an outpatient/minor-procedure room is the dominant cost-effective approach, reserving electrodiagnostics for atypical or revision cases.
Special Scenarios
Martin-Gruber Anastomosis
-
Median → Ulnar connection in forearm.
-
15% prevalence.
-
Can cause "Ulnar" muscles to be spared in a high Ulnar lesion (supplied by Median).
-
Ulnar → Median connection in hand (Deep branch to Recurrent).
-
Can cause Thenar sparing in CTS.
These anomalies can confuse NCS findings.
Two carpal-tunnel variants are high-yield because they raise CTS risk and are operative/ultrasound hazards:
- Bifid median nerve: the nerve divides into two (or more) fascicular bundles within or proximal to the tunnel (roughly 2 to 3 percent of wrists, higher on ultrasound series). The larger combined cross-sectional area predisposes to CTS, and at release both limbs must be decompressed and protected — a missed second limb is a cause of incomplete release.
- Persistent median artery: an embryological remnant that usually regresses but persists in a minority, frequently accompanying a bifid nerve and running with it into the palm. It can itself crowd the tunnel (and may thrombose, causing acute CTS) and is a bleeding/injury hazard, especially during endoscopic or ultrasound-guided release, where it must be identified before the retinaculum is divided.
- Practical point: pre-operative ultrasound readily shows both; their presence argues for caution (or open release) and for protecting the radial and ulnar limbs of the nerve.
Controversies & Areas of Uncertainty
- Routine electrodiagnostics: Whether nerve conduction studies are mandatory before carpal tunnel release in classic cases is debated. UK/European practice increasingly accepts a clinical diagnosis (with validated questionnaires) for typical presentations, whereas many US centres still obtain confirmatory studies, partly for medicolegal and work-related reasons.
- Endoscopic vs open release: Despite faster return to work with endoscopic release, the absence of any long-term advantage in symptom relief, plus a transiently higher rate of (usually reversible) nerve problems, keeps the choice surgeon- and patient-dependent rather than evidence-mandated.
- Existence of "pronator syndrome": Some authors question pronator syndrome as a discrete compressive entity, noting overlap with proximal median irritation, lacertus syndrome and neuralgic amyotrophy, and the historically inconsistent surgical results.
- AIN palsy aetiology: The pendulum has shifted from mechanical compression toward neuralgic amyotrophy with hourglass fascicular constrictions; this affects timing of surgery and the role of high-resolution ultrasound or MRI in selecting patients who will not recover spontaneously.
- Ultrasound as a stand-alone test: Cross-sectional area thresholds vary between studies and operators, so ultrasound is best viewed as complementary to, not a replacement for, electrodiagnosis.
MCQ Practice Points
Q: Which fibers cross in Martin-Gruber anastomosis? A: Motor fibers from Median to Ulnar. Usually AIN branch fibers crossing to Ulnar nerve in the forearm to supply intrinsics (First Dorsal Interosseous).
Q: Which lumbricals are Median innervated? A: 1 and 2 (Index and Middle). They are unipennate. 3 and 4 are Ulnar and bipennate.
Q: Which structure is most superficial in the Carpal Tunnel? A: FDS to Middle/Ring. The FDS tendons are stacked 2 over 2 (3/4 over 2/5). The FPL is radial/deep. The Nerve is superficial to the tendons.
Q: The Median nerve passes between which two heads? A: The superficial (humeral) and deep (ulnar) heads of Pronator Teres. The ulnar artery passes deep to the deep head (separating artery and nerve).
Q: Where does the Palmar Cutaneous Branch arise? A: ~5cm proximal to the wrist crease. It travels superficial to the Transverse Carpal Ligament. This is why it is spared in Carpal Tunnel Syndrome (compression is deep to ligament) but can be injured in the surgical incision if placed too radially.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 65-year-old lady presents with severe thenar wasting but no pain. She says her hands just feel 'clumsy'. Diagnosis?”
“A patient returns 3 months after Open CTR with WORSE pain and pillar tenderness. What is your differential?”
“A novice gymnast presents with inability to flex the IPJ of the thumb and DIPJ of the index finger. There is no sensory loss. What is the pathology?”
Anatomy High Yield
- Roots: C5-T1
- Cords: Medial + Lateral
- Tunel: 9 Tendons + 1 Nerve
- LOAF: Lumbricals 1/2, Opponens, APB, FPB
Clinical Signs
- Benediction: High Palsy (Active)
- OK Sign: AIN (Motor)
- Phalen's: CTS (Sensory)
- Durkan's: CTS (Compression)
Key Numbers
- 6mm: Normal 2-point discrimination
- Greater than 10mm²: US diagnosis of CTS
- Greater than 4.2ms: Motor Latency (abnormal)
- 5cm: PCB branching proximal to wrist
Surgical Steps
- Incision: Ring finger axis
- Kaplan's Line: Distal extent
- TCL: Cut on Ulnar side
- Protect: Recurrent Branch
Evidence Base
Splinting vs Surgery for CTS (Landmark RCT)
- 176 patients, open release vs nocturnal wrist splint, 18-month follow-up
- Success at 3 months: 80% surgery vs 54% splint (difference 26%)
- Success at 18 months: 90% surgery vs 75% splint (difference 15%)
- 41% of the splint group ultimately crossed over to surgery
Endoscopic vs Open CTR (Cochrane Review)
- 28 studies, 2586 hands; ECTR vs OCTR
- No difference in symptom relief or functional status at long-term follow-up
- Return to work ~8 days earlier with endoscopic release
- ECTR: more transient nerve problems but fewer wound complications
Corticosteroid Injection Efficacy (Cochrane Review)
- 12 studies, 671 participants
- Clinical improvement at 1 month vs placebo (RR 2.58)
- Benefit beyond 1 month not demonstrated vs placebo
- Local injection superior to oral corticosteroid up to 3 months
Ultrasound vs Electrodiagnosis for CTS
- Meta-analysis, 19 studies, 3131 wrists
- Ultrasound pooled sensitivity 77.6%, specificity 86.8%
- Wide variation across studies limits firm conclusions
Prevalence of CTS in a General Population
- Population survey of 2466 responders in southern Sweden
- Median-distribution symptoms in 14.4%
- Clinically certain CTS 3.8%; clinically AND electrophysiologically confirmed 2.7%
- Roughly 1 in 5 symptomatic subjects had confirmed CTS
AIN/PIN Palsy in Neuralgic Amyotrophy
- 51 cases of AIN/PIN involvement in neuralgic amyotrophy
- Pain was the presenting symptom in 52.9%, usually distal to the shoulder
- Neurolysis significantly improved Hand20 scores; conservative treatment did not
- Hourglass fascicular constrictions may explain failure to recover spontaneously