The Silent Meniscectomy
LaPrade Classification
Critical Must-Knows
- A root tear is biomechanically equivalent to a total meniscectomy.
- Hoop stress is lost, leading to peak contact pressure increase.
- Medial root tears are more common (degenerative/deep flexion).
- Lateral root tears are associated with ACL tears.
- The 'Ghost Sign' on Sagittal MRI is pathognomonic.
Clinical Pearls
- "Always look for the root tear in patients with a 'pop' during deep squatting.
- "Extrusion greater than 3mm indicates incompetence of the meniscus.
- "Spontaneous Osteonecrosis of the Knee (SONK) is often secondary to a missed root tear.
Clinical Imaging
Imaging Gallery




High Yield Concept
The Biomechanical Disaster
Loss of Hoop Stress. The meniscus functions to convert axial load into hoop stress. When the root tears, this mechanism fails completely. The femur articulates directly with the tibia (bone-on-bone forces).
Association
Lateral vs Medial.
- Medial: Degenerative, Middle-aged, Deep Flexion (Squatting/Gardening).
- Lateral: Acute, Young, ACL Tear association (10-15%).
| Feature | Medial Root | Lateral Root |
|---|---|---|
| Mechanism | Deep Flexion/Degenerative | Acute Trauma (ACL) |
| Patient Age | 50-60s | 20-30s |
| Arthritis Risk | High (Rapid Progression) | High (Lateral OA) |
| Repair Urgency | Semi-urgent (Prevent OA) | Acute (With ACL) |
ROOTSIndications for Repair
| R | Rotational Control rotational stability |
| O | OA Mild OA (Kellgren-Lawrence less than 3) |
| O | Outer Outerbridge 1-2 only |
| T | Timing Acute/Subacute preferred |
| S | Stable Stable knee/alignment (Correct varus first) |
| R | Rotational Control rotational stability | T | Timing Acute/Subacute preferred |
| O | OA Mild OA (Kellgren-Lawrence less than 3) | S | Stable Stable knee/alignment (Correct varus first) |
| O | Outer Outerbridge 1-2 only |
Hook:Plant the ROOTS to save the tree (knee).
GHOSTMRI Signs
| G | Ghost Ghost Sign (Empty Sagittal view) |
| H | High High signal at root |
| O | Out Extrusion (Out of joint, greater than 3mm) |
| S | Subchondral Subchondral edema (SONK-like) |
| T | Truncated Truncated meniscus sign |
| G | Ghost Ghost Sign (Empty Sagittal view) | S | Subchondral Subchondral edema (SONK-like) |
| H | High High signal at root | T | Truncated Truncated meniscus sign |
| O | Out Extrusion (Out of joint, greater than 3mm) |
Hook:The meniscus is a GHOST.
BAD KNEEContraindications
| B | BMI greater than 35 (Relative) |
| A | Arthritis Severe OA (KL 3-4) |
| D | Dealignment Severe Malalignment (uncorrected) |
| KNEE | Knee Unstable knee (e.g. chronic ACL deficiency) |
| B | BMI greater than 35 (Relative) | D | Dealignment Severe Malalignment (uncorrected) |
| A | Arthritis Severe OA (KL 3-4) | KNEE | Knee Unstable knee (e.g. chronic ACL deficiency) |
Hook:Don't fix a BAD KNEE.
Overview
The Silent Epidemic
Meniscal root tears are often missed in primary care. Patients present with posterior knee pain after a minor event (squatting). X-rays are often normal or show mild OA. Without MRI, the diagnosis is missed, leading to rapid joint destruction (SONK).
A meniscal root tear is defined as an avulsion of the meniscal attachment (or tear within 1cm of the attachment). It results in the complete loss of the ability of the meniscus to withstand circumferential hoop tension, rendering the meniscus functionally incompetent.
This injury was historically under-recognized and often treated as a simple meniscal tear. However, modern biomechanical understanding has redefined it as a major structural failure requiring urgent attention. It represents a "silent" cause of rapid joint destruction.
Anatomy and Biomechanics
Insertion Sites
- Medial Root:
- Posterior to the medial tibial spine.
- 1cm posterior to the ACL connection.
- Located on the downslope of the retro-eminence.
- Approximately 9.6mm posterior and 0.7mm lateral to the apex of the medial tibial eminence.
- Close proximity to the PCL insertion.
- Lateral Root:
- Adjacent to the ACL footprints.
- Often torn with ACL avulsion.
The medial root is most vulnerable to shear in deep flexion.
Pathophysiology
Mechanism of Injury
Traumatic root tears:
- Deep flexion during squat or kneeling activities
- Pivot mechanism with axial loading
- Posterior horn trapped between femoral condyle and tibial plateau
- More common in young active patients
Degenerative root tears:
- Chronic degeneration of root attachment
- Often associated with existing osteoarthritis
- Common in patients over 50 years
- May occur with minimal trauma ("pop while getting up from chair")
Loss of Hoop Stress - The Critical Concept
The meniscal root anchors circumferential collagen fibers that convert axial load into circumferential (hoop) stress. When the root is torn:
- Circumferential fibers lose their anchor point
- Axial load cannot be converted to hoop stress
- Meniscus extrudes radially
- Functionally equivalent to total meniscectomy
- 25% immediate loss of tibiofemoral contact area
- Rapid progression to medial compartment osteoarthritis
Natural History Without Treatment
Untreated medial meniscal root tears progress predictably:
- Meniscal extrusion of greater than 3mm within months
- Progressive cartilage degeneration
- Development of medial compartment OA within 2-5 years
- Eventual need for knee arthroplasty
Classification Systems
LaPrade Classification (Morphology)
- Type 1: Partial stable root tear.
- Type 2: Complete radial tear within 9mm of root. (Most common operative type).
- Type 3: Bucket-handle tear extending into root.
- Type 4: Complex oblique tear into root.
- Type 5: Avulsion fracture of the root attachment.
Type 2 and 4 are the classic "Root Tears" requiring repair.
Type 5 is essentially an avulsion fracture.
History
Patient History
- Mechanism: Usually non-contact. "Pop" felt while squatting, kneeling, or descending stairs.
- Pain: Posterior knee pain. Constant.
- Locking: Mechanical locking is UNCOMMON (unlike bucket handle tears).
The absence of locking often delays presentation.
Examination
Physical Exam
- Effusion: Mild to moderate.
- Joint Line Tenderness: Posterior medial joint line (highly sensitive).
- Seated McMurray: Pain with external rotation/varus.
- Deep Squat: Pain at maximum flexion.
A high index of suspicion is required to avoid missing this diagnosis.
Clinical Presentation
The Classic Presentation
A middle-aged patient (typically a woman in her 50s-60s) with a sudden "pop" or "tearing" sensation in the back of the knee during a low-energy deep-flexion activity (squatting, kneeling, rising from a low chair), followed by persistent posteromedial pain and an effusion, with normal or near-normal plain radiographs.
Symptom Pattern
- Onset: Often a discrete, low-energy event. Up to half of degenerative medial root tears occur with trivial trauma; many patients cannot recall a single event.
- Pain: Deep, posteromedial knee pain that is constant rather than purely mechanical. Pain is reproducibly worse with deep flexion and weight-bearing rotation.
- Mechanical symptoms: True locking is UNCOMMON (contrast with displaced bucket-handle tears). Patients may report giving way or a vague "instability" from quadriceps inhibition rather than ligamentous laxity.
- Functional impact: Difficulty with stairs (especially descending), squatting, and rising from low seating. Night pain is common when an associated subchondral insufficiency fracture is present.
Two Distinct Clinical Phenotypes
| Feature | Medial Root (Degenerative) | Lateral Root (Traumatic) |
|---|---|---|
| Typical patient | Woman, 50-60s, raised BMI | Young athlete, often male |
| Mechanism | Deep flexion / minor trauma | High-energy pivot, ACL rupture |
| Key association | SONK / subchondral insufficiency fracture | ACL tear (8-15% of ACL ruptures) |
| Dominant symptom | Posteromedial pain, slow onset | Acute haemarthrosis with instability |
Examination Synthesis
A focused examination integrates the findings above into a coherent picture rather than relying on any single test:
- Inspection/palpation: Small-to-moderate effusion; posteromedial joint-line tenderness is the most sensitive single sign for a medial root tear.
- Provocative tests: Pain on a seated McMurray (external rotation, varus) and at terminal deep squat. No single physical test is specific, so MRI is mandatory for confirmation.
- Alignment and the rest of the limb: Always assess standing alignment (varus loads the medial compartment), ligamentous stability (rule out concurrent ACL injury, especially with lateral root tears), and contralateral knee for comparison.
Imaging: MRI
The Ghost Sign
Sagittal View is Key. On sagittal sequences, the posterior horn normally appears as a black triangle ("Bow tie"). In a root tear, this triangle is absent or replaced by fluid signal. This is the "Ghost Sign".
MRI Signs
- Ghost Sign: Absence of meniscus on sagittal cut.
- Cleft Sign: Fluid signal (vertical line) at the root on T2 Coronal.
- Radial Extrusion: Greater than 3mm extrusion of the medial meniscus body relative to the tibial plateau (Coronal view).
- Giraffe Neck Sign: Distortion of the meniscus.
Look for edema in the subchondral bone adjacent to the root.

Management Algorithm
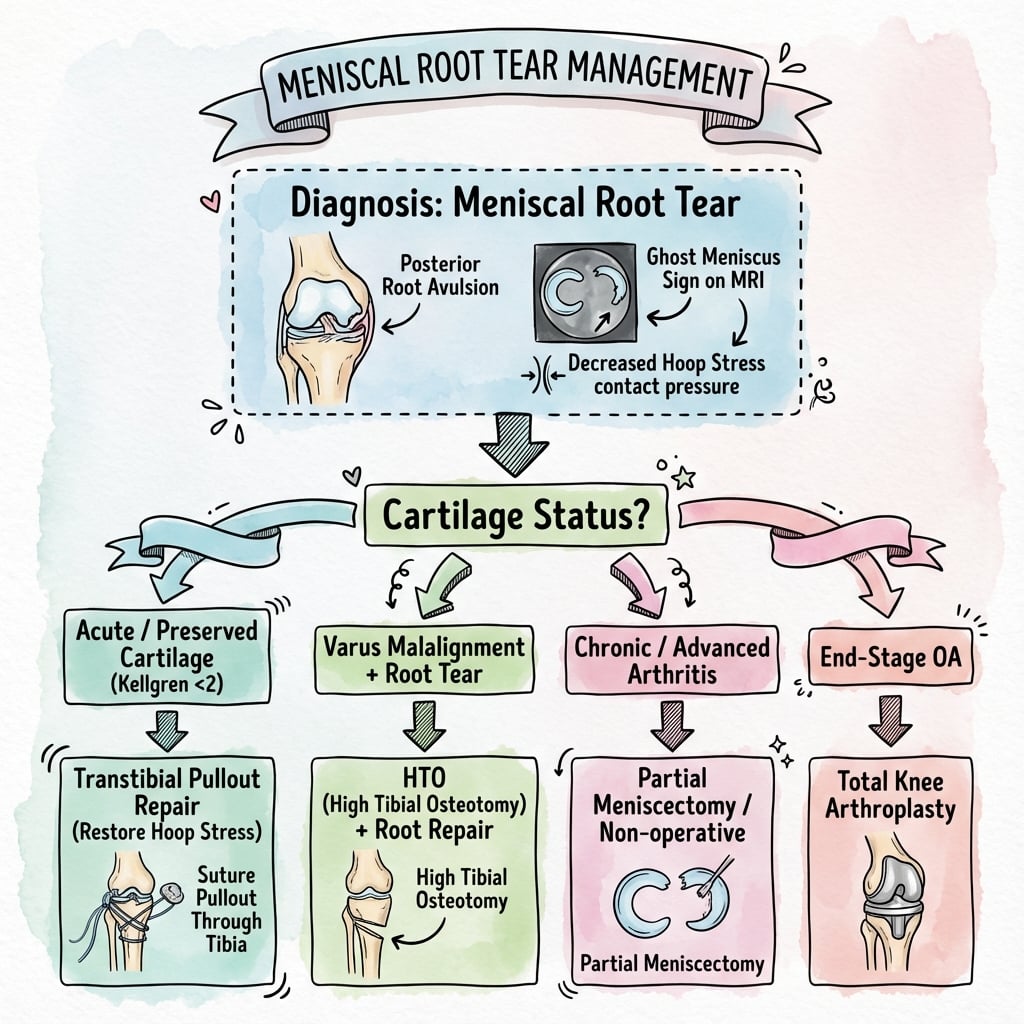
Decision Making
- Group A (Ideal): Age less than 65, BMI less than 35, KL Grade 0-2, Normal alignment. ACTION: REPAIR.
- Group B (Borderline): Mild varus, Age greater than 65 but active. ACTION: Consider HTO + Repair.
- Group C (Poor): Severe OA (KL 3-4), Fixed flexion deformity. ACTION: Non-operative / Total Knee.
Partial meniscectomy is reserved for failed repairs or symptomatic relief in poor candidates, but it accelerates OA.
Surgical Considerations
Transtibial Pull-out Repair
- Concept: Sutures passed through the root, pulled down a tibial tunnel, and fixed on the anterior tibia (Button).
- Pros: Strong restoration of footprint.
- Cons: "Bungee cord" effect (suture elongation), technically demanding.
- Steps:
- Debride root footprint to bleeding bone.
- Pass sutures (Luggagetag/Cinch) through meniscus.
- Drill tibial tunnel using ACL guide (aiming at footprint).
- Pass sutures down tunnel.
- Fix over button on anterior tibia.
Ensure the tunnel exit point doesn't compromise the PES attachment.
Complications
- Failure of Repair: Suture breakage or pull-through (10-15%).
- Progression of OA: Despite repair, some arthritis may progress.
- Arthrofibrosis: Stiffness due to immobilization.
- Posterior Neurovascular Injury: Risk during drilling or anchor placement (Popliteal vessels are directly posterior).
- Saphenous Nerve Injury: During tibial tunnel drilling/button placement.
- Meniscal Cyst Formation: Can occur at the repair site or due to fluid leak.
- Iatrogenic Cartilage Injury: During instrumentation in the tight posterior compartment.
Rehabilitation
-
Phase 1 (0-6 weeks):
- Non-weight bearing (or toe-touch) in brace in extension.
- Passive ROM 0-90 degrees.
- Avoid deep flexion (greater than 90) to protect repair.
-
Phase 2 (6-12 weeks):
- Progress to full weight bearing.
- Full ROM.
- Closed chain strengthening.
-
Phase 3 (3-6 months):
- Return to running.
-
Phase 4 (greater than 6 months):
- Return to sport/squatting.
Note: Protocol is surprisingly slow compared to meniscectomy because root healing takes time.
Return to Sport Criteria
- Full pain-free range of motion.
- No effusion.
- Quadriceps strength greater than 90% of contralateral side.
- Hamstring strength greater than 90% of contralateral side.
- Successful completion of functional hop tests.
- Timeframe: Usually 6-9 months post-operatively.
Early return leads to failure of the repair construct.
Prognosis
Outcomes by Treatment
- Repair Survival: 5-year survival approximately 85% in ideal candidates.
- Extrusion Response: Rarely improves fully, but progression is halted with repair.
- OA Progression: Significantly slower than meniscectomy, but faster than normal knee.
- Meniscectomy: Rapid OA progression within 2-3 years in most patients.
Prognostic Factors
| Factor | Favorable | Unfavorable |
|---|---|---|
| Age | Less than 50 years | Greater than 65 years |
| BMI | Less than 30 | Greater than 35 |
| Cartilage | Outerbridge 0-2 | Outerbridge 3-4 |
| Alignment | Neutral | Varus greater than 5 degrees |
| Timing | Acute (less than 6 weeks) | Chronic (greater than 3 months) |
Long-Term Considerations
- Conversion to TKA: 30% at 5 years in non-operative management vs 10-15% with repair.
- Functional Outcomes: Significant improvement in IKDC and Lysholm scores with repair.
- Activity Level: Most patients return to recreational activities but may need to modify high-impact sports.
Evidence Base
Root Tear Is Biomechanically a Total Meniscectomy
- Nine fresh-frozen cadaver knees loaded to 1000 N at 0, 30, 60 and 90 degrees of flexion
- Medial root tear raised medial-compartment peak contact pressure by 25% versus intact (p less than 0.001)
- No detectable difference between root tear and total medial meniscectomy
- Root repair restored peak contact pressure and corrected the abnormal external rotation and lateral translation
Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: The Pop in the Garden
"A 55-year-old female presents with acute posterior knee pain after squatting in the garden. She felt a pop. X-rays show mild OA. What is your differential?"
Scenario 2: The ACL Associated Tear
"You are performing an ACL reconstruction. You inspect the lateral meniscus posterior horn. It looks mobile. How do you assess for root tear?"
Scenario 3: The Failed Repair
"A patient 6 months post-root repair returns with pain. MRI shows pull-through of sutures. She has Grade 3 OA. Management?"
MCQ Practice Points
Biomechanics
Q: A meniscal root tear increases contact pressure equivalent to: A: Total Meniscectomy.
Imaging Sign
Q: The 'Ghost Sign' is seen on which MRI sequence? A: Sagittal T2.
Management
Q: Which factor is a relative contraindication to root repair? A: Kellgren-Lawrence Grade 3-4 OA.
Extrusion
Q: Significant meniscal extrusion is defined as: A: Greater than 3mm.
SONK Association
Q: What is the relationship between SONK and meniscal root tears? A: 80% of SONK patients have associated medial root tears - SONK is likely secondary subchondral insufficiency fracture from root-tear overload.
Surgical Technique
Q: What is the most common surgical technique for meniscal root repair? A: Transtibial pull-out repair - sutures through root, passed down tibial tunnel, fixed over button.
Controversies and Areas of Uncertainty
What the Evidence Does Not Yet Settle
Meniscal root repair is biomechanically compelling but the high-level clinical evidence base remains immature. Be ready to discuss these unresolved questions in a viva.
- Repair versus structured non-operative care: No adequately powered randomised controlled trial directly compares anatomic root repair with optimised non-operative management. Recommendations rest on cadaveric biomechanics, cohort studies and meta-analyses of mostly Level IV data.
- Persistent extrusion: Even successful repairs frequently fail to reverse meniscal extrusion, and the long-term chondroprotective benefit therefore remains debated. "Healed on second-look MRI" does not guarantee restored hoop-stress mechanics.
- Transtibial pull-out versus suture-anchor fixation: Both restore the footprint; the clinical superiority of one over the other (and the significance of the suture "bungee/creep" effect) is unproven.
- Centralisation techniques: Adjunctive meniscal centralisation (anchoring the mid-body to the tibial rim to limit extrusion) is an area of active investigation without mature outcome data.
- Degenerative tear in older patients: The boundary between a repairable root tear and an early-arthritic knee best served by non-operative care or arthroplasty is judgement-based; age alone is a weak discriminator if alignment, cartilage status and BMI are favourable.
- Role of biologics: Marrow venting, platelet-rich plasma and other augments are used variably without convincing comparative evidence.
Guidelines, Registries and Global Practice
Global Epidemiology
- Medial posterior root tears are predominantly degenerative, peaking in the 5th-7th decades, with a female predominance and an association with raised BMI and varus alignment.
- Lateral posterior root tears are predominantly traumatic and are reported in roughly 8-15% of ACL ruptures, typically in younger, more active patients.
- Root tears account for a meaningful minority of all meniscal tears and were historically under-recognised; MRI awareness has substantially increased detection over the last two decades.
Side-by-Side Guidance
| Body / Source | Emphasis on root tears |
|---|---|
| AAOS (US) | Degenerative meniscal/OA guidance cautions against routine arthroscopic partial meniscectomy in osteoarthritic knees; favours structured non-operative care first in arthritic compartments |
| ESSKA (Europe) | Consensus on degenerative meniscus lesions supports exhausting non-operative care for degenerative tears, while recognising root tears as a distinct, repair-amenable entity in suitable knees |
| ISAKOS / sports-medicine consensus | Recognises root tears as biomechanically equivalent to meniscectomy and recommends repair in young/active patients and acute lateral root tears with ACL reconstruction |
| AO Foundation | Stresses anatomic footprint restoration and protection of the posterior neurovascular structures during transtibial tunnel or anchor fixation |
The common thread across societies: do not treat a root tear as a routine degenerative tear; either repair it in a biomechanically salvageable knee or manage the arthritic knee on its own merits, but avoid simple partial meniscectomy that accelerates arthritis.
Registry Perspective
- General arthroplasty registries (NJR, AJRR, AOANJRR, Swedish/Norwegian) do not track meniscal root repair as a discrete procedure, so survivorship data come from institutional cohorts and meta-analyses rather than registries.
- Registry data are nonetheless relevant downstream: untreated root tears feed the cohort progressing to unicompartmental or total knee arthroplasty, where registries show that younger arthroplasty recipients carry higher lifetime revision burden, reinforcing the value of joint-preserving repair when feasible.
High- versus Limited-Resource Practice
- High-resource settings: Routine MRI, arthroscopic transtibial pull-out or suture-anchor repair, and concomitant high tibial osteotomy for malalignment are widely available.
- Limited-resource settings: MRI access and arthroscopic root-repair capability may be constrained; management leans toward activity modification, unloader bracing, weight optimisation and, where indicated, arthroplasty. The diagnostic priority everywhere is to recognise the lesion clinically and on plain films/MRI so that it is not mislabelled as simple osteoarthritis.
Clinical summary
Diagnosis
- •Mechanism: Squatting 'pop'
- •Sign: Joint line tenderness
- •MRI: Ghost Sign
- •MRI: Cleft Sign
- •MRI: Extrusion over 3mm
Decision Making
- •Ideal: Young, No OA, Normal alignment
- •Contraindication: Severe OA (KL 3-4)
- •Contraindication: BMI over 35
- •Contraindication: Malalignment (unless corrected)
Surgical Steps
- •Assessment: Probe root
- •Debridement: Bleeding bone
- •Suture: Cinch/Locking
- •Tunnel: ACL guide aiming at footprint
- •Fixation: Button on tibia