SPONK/SONK | Subchondral Insufficiency Fracture | Medial Femoral Condyle
- SPONK is now understood as subchondral insufficiency fracture rather than primary avascular necrosis
- Sudden onset medial knee pain in elderly female without trauma is the classic presentation
- MRI is essential for early diagnosis and lesion size measurement
- Lesions involving less than 40 percent of condylar width often heal with conservative care
- Large lesions or collapse greater than 2 mm usually require surgical intervention
- “Differentiate from secondary osteonecrosis (steroids, alcohol, sickle cell)
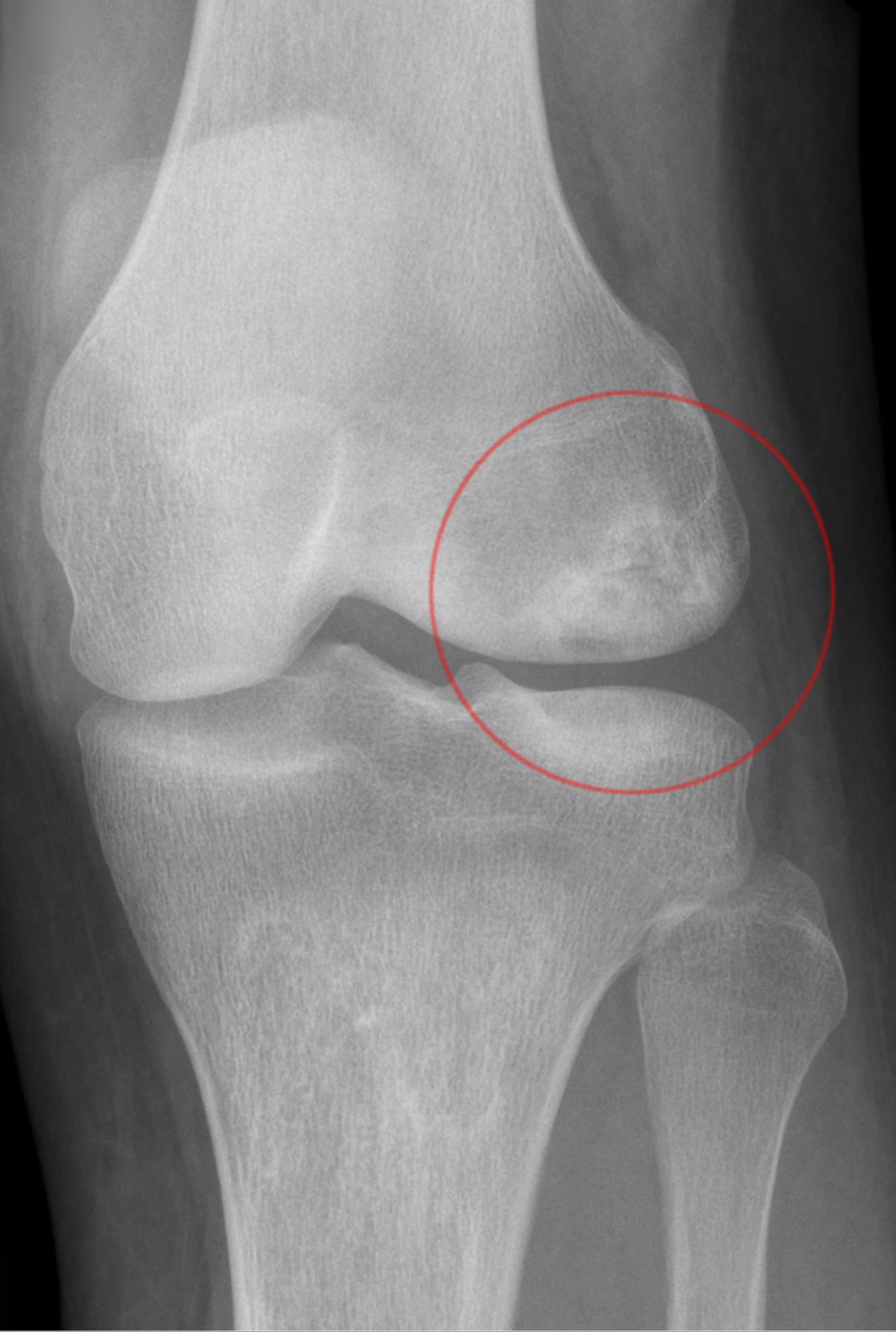
- “Weight-bearing AP and Rosenberg views show early flattening of medial condyle
- “Lesion size on MRI (area and percentage of condyle) determines prognosis
- “High tibial osteotomy unloads the medial compartment in younger active patients
Elderly female (greater than 60 years). Sudden onset severe medial knee pain without trauma. Night pain common. Differentiate from secondary ON which has risk factors (steroids, alcohol, haemoglobinopathy).
Medial femoral condyle in greater than 90 percent. Weight-bearing surface. Lateral condyle or tibial plateau involvement suggests alternative diagnosis or secondary ON.
Early diagnosis before X-ray changes. Quantify lesion size (area, percentage of condyle width, depth). Bone marrow oedema extent predicts healing potential.
Lesion size drives decision. Small lesions (less than 40 percent width, area less than 5 square centimetres) often heal conservatively. Large lesions or greater than 2 mm collapse require surgery.
- SPONK/SONK
- Elderly female, no risk factors
- Secondary ON
- Any age, steroid/alcohol/sickle history
- Key Discriminator
- History of systemic risk factors
- SPONK/SONK
- Sudden severe pain, no trauma
- Secondary ON
- Insidious or after risk exposure
- Key Discriminator
- Temporal relationship to steroids
- SPONK/SONK
- Medial femoral condyle only
- Secondary ON
- Multiple sites, bilateral possible
- Key Discriminator
- Single site medial condyle favours SPONK
- SPONK/SONK
- Focal subchondral fracture line
- Secondary ON
- Diffuse serpiginous lesions
- Key Discriminator
- Serpiginous pattern indicates secondary ON
SIZEMRI Lesion Size Criteria
Hook:Measure SIZE on MRI before deciding conservative versus operative treatment!
Overview and Epidemiology
Spontaneous osteonecrosis of the knee (SPONK/SONK) is the most common form of osteonecrosis around the knee and must be distinguished from secondary osteonecrosis which carries systemic risk factors and often multifocal disease. The current understanding is that SONK begins as a subchondral insufficiency fracture in osteopenic bone rather than primary vascular occlusion. Early recognition on MRI before radiographic collapse allows a trial of protected weight bearing that can prevent progression in small lesions. Larger lesions or established collapse require unloading osteotomy or arthroplasty, making accurate lesion sizing and staging essential for surgical planning.
- Peak age: 60-70 years, female predominance (2-3:1)
- Incidence: Underestimated, many cases labelled as OA or meniscus tear
- Location: Medial femoral condyle in greater than 90 percent of cases
- Bilateral: Less than 5 percent (unlike secondary ON)
- Sudden severe pain: Often mistaken for meniscus tear or flare of OA
- Night pain: Distinguishes from mechanical meniscus symptoms
- Rapid progression: Collapse can occur within weeks to months
- Functional loss: Antalgic gait, reduced walking distance, difficulty with stairs
Pathophysiology
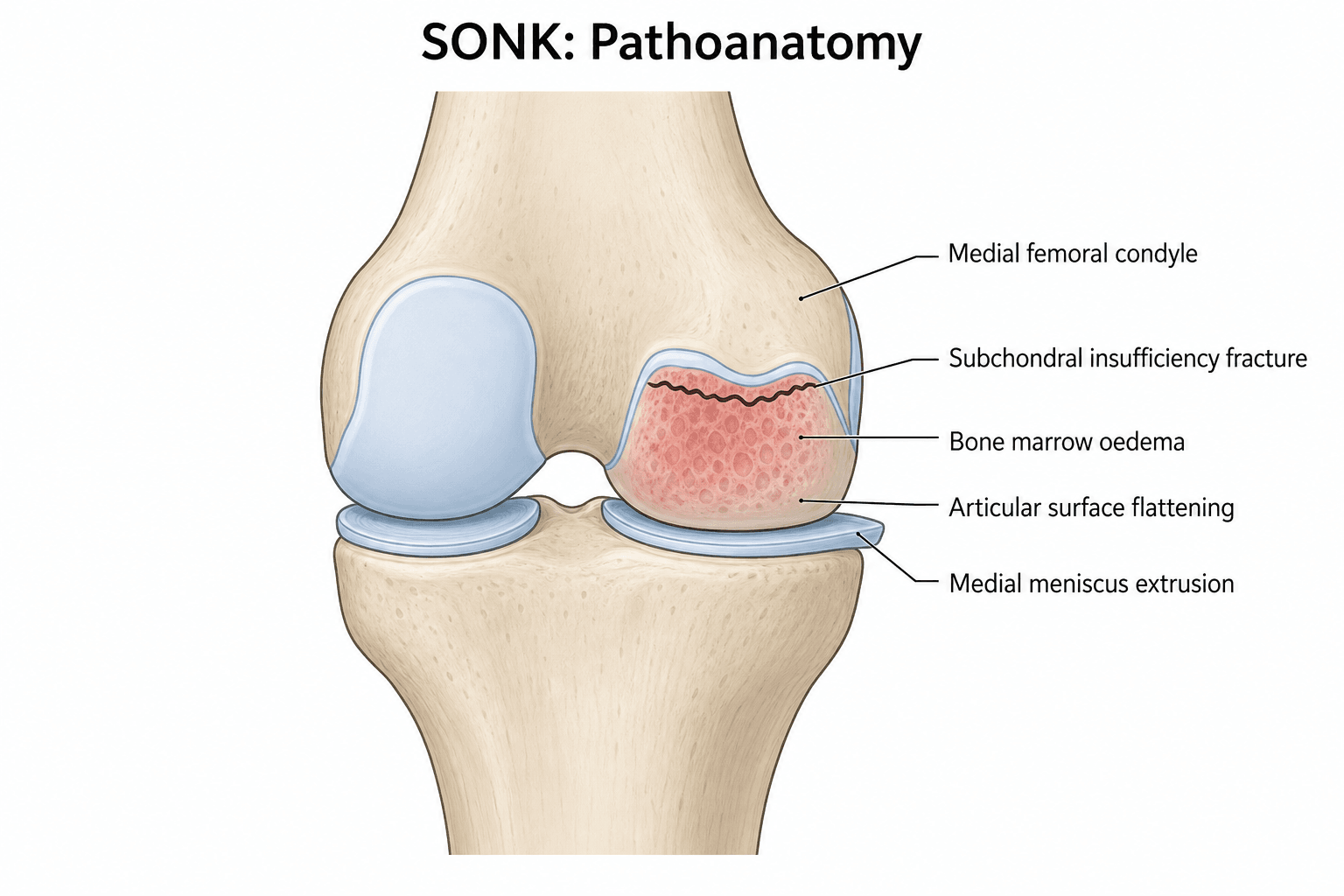
Current evidence supports that SONK is initiated by a subchondral insufficiency fracture in osteopenic bone rather than primary avascular necrosis. Repetitive loading on weakened subchondral trabeculae produces microfracture. The fracture disrupts local blood supply, leading to focal osteonecrosis and subsequent articular collapse. This explains the typical single-site medial condyle location in elderly patients without systemic risk factors. Secondary osteonecrosis, by contrast, involves true vascular occlusion from fat emboli, coagulopathy or steroid-induced adipocyte hypertrophy and is often multifocal.
- SPONK/SONK
- Subchondral insufficiency fracture
- Secondary ON
- Vascular occlusion (fat emboli, steroids)
- Clinical Relevance
- History of risk factors points to secondary ON
- SPONK/SONK
- Osteopenic elderly bone
- Secondary ON
- Normal bone with superimposed insult
- Clinical Relevance
- DEXA scan useful in SONK workup
- SPONK/SONK
- Single focus, medial condyle
- Secondary ON
- Multiple foci, often bilateral
- Clinical Relevance
- Screen hips and shoulders if secondary suspected
- SPONK/SONK
- Focal fracture line + oedema
- Secondary ON
- Serpiginous geographic lesions
- Clinical Relevance
- Pattern recognition avoids misdiagnosis
Osteopenic subchondral bone fails under physiologic load. Reduced trabecular thickness and connectivity in elderly patients lower the threshold for microfracture. Continued weight bearing propagates the fracture line, isolating a segment of subchondral bone from its blood supply.
Subchondral fracture leads to focal osteonecrosis. Loss of structural support causes flattening of the weight-bearing surface. Joint incongruity accelerates cartilage wear and secondary osteoarthritis. Varus malalignment develops, further increasing medial compartment load.
FRACTURESONK Pathophysiology Cascade
Hook:Subchondral insufficiency FRACTURE starts the SONK cascade - protect the bone early!
The Third Type: Post-Arthroscopic Osteonecrosis
Examiners classically divide osteonecrosis around the knee into three types - the sections above contrast the first two, but the third is equally testable.
- Typical patient
- Elderly woman, no risk factors
- Key features
- Single medial femoral condyle lesion, subchondral insufficiency fracture
- Typical patient
- Younger, systemic risk factors (steroids, alcohol, sickle cell, SLE)
- Key features
- Multifocal, often bilateral, serpiginous, metaphyseal/diaphyseal extension
- Typical patient
- Older patient weeks-to-months AFTER knee arthroscopy (often meniscectomy)
- Key features
- New osteonecrosis in the operated compartment, not present pre-operatively
- Post-arthroscopic osteonecrosis develops in a previously normal-imaging compartment after an arthroscopy - classically after partial medial meniscectomy. The leading explanation is again a subchondral insufficiency fracture in the now mechanically-altered (and often chondromalacic) compartment, rather than thermal/laser injury alone.
- The medicolegal trap: because it appears after surgery it can be mistaken for a surgical complication, so a pre-operative MRI documenting normal subchondral bone is invaluable.
- Management mirrors SONK (size- and collapse-based: protected weight bearing for small lesions, UKA or osteotomy for large or collapsed lesions).
Q: What are the three types of osteonecrosis around the knee? A: Spontaneous (SONK) - elderly woman, single medial condyle, subchondral insufficiency fracture; secondary - systemic risk factors, multifocal/bilateral, serpiginous; and post-arthroscopic (PAON) - new osteonecrosis in the operated compartment weeks to months after arthroscopy (classically post-meniscectomy), again thought to be a subchondral insufficiency fracture.
Classification and Staging
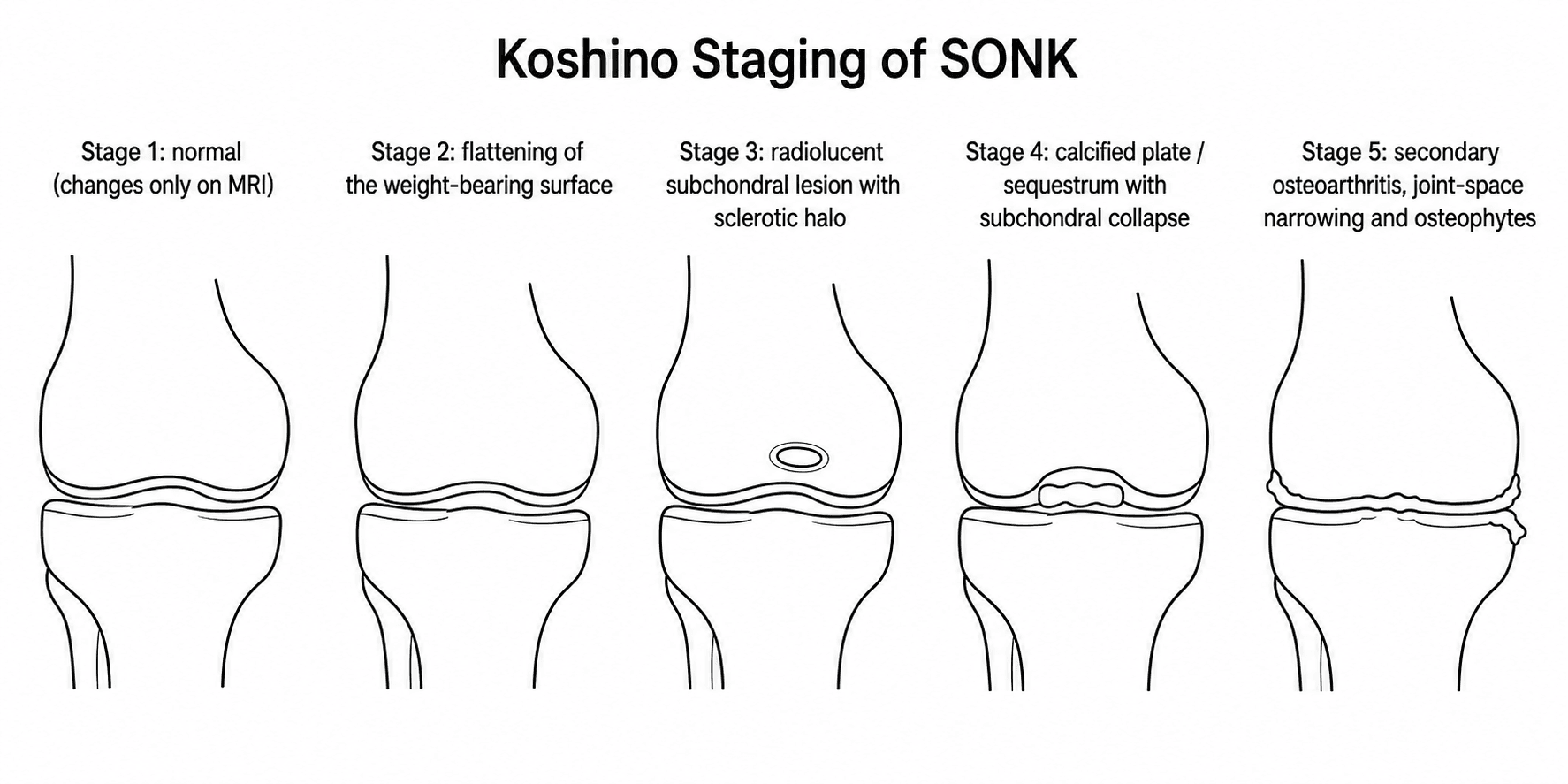
Modified Koshino MRI Staging for SONK
- Radiographic Findings
- Normal or subtle sclerosis
- MRI Findings
- Bone marrow oedema, possible linear fracture line
- Treatment Implications
- Protected weight bearing, high healing potential
- Radiographic Findings
- Subchondral radiolucency or flattening
- MRI Findings
- Oedema + subchondral fracture line visible
- Treatment Implications
- Bisphosphonate trial, close radiographic follow-up
- Radiographic Findings
- Crescent sign, subchondral collapse
- MRI Findings
- Fragmentation, fluid-filled cleft
- Treatment Implications
- Consider high tibial osteotomy or UKA
- Radiographic Findings
- Secondary OA, joint space loss
- MRI Findings
- Full-thickness cartilage loss, osteophytes
- Treatment Implications
- UKA or TKA based on compartment involvement
MRI staging is performed on coronal and sagittal T2-weighted and STIR sequences. The critical measurements are lesion width as percentage of condylar width, total lesion area, and depth of collapse.
Clinical Assessment
- Onset: Sudden severe medial knee pain, often after minor activity or at night
- No trauma: Patient frequently denies any injury
- Night pain: Wakes from sleep, distinguishes from mechanical symptoms
- Progression: Pain may improve slightly then worsen with collapse
- Risk factors: Ask specifically about steroids, alcohol, sickle cell, Gaucher disease
- Gait: Antalgic, varus thrust may be present if collapse advanced
- Swelling: Mild effusion, medial joint line tenderness
- ROM: Limited by pain, possible flexion contracture if chronic
- Stability: Usually stable unless secondary ligamentous laxity from collapse
- Alignment: Measure mechanical axis, varus deformity common in advanced cases
Key clinical discriminator: Sudden onset without trauma in an elderly patient with night pain should raise suspicion for SONK. Mechanical locking or catching suggests meniscus pathology. Gradual pain increase over months is more typical of primary osteoarthritis. Always obtain MRI in this demographic with unexplained medial knee pain.
- Onset
- Sudden, no trauma
- Night Pain
- Prominent
- Key Discriminating Feature
- MRI shows subchondral fracture line and oedema
- Onset
- Twisting or squatting
- Night Pain
- Rare
- Key Discriminating Feature
- MRI shows meniscal signal to articular surface
- Onset
- Gradual over weeks
- Night Pain
- Mild
- Key Discriminating Feature
- Joint space narrowing, osteophytes on X-ray
- Onset
- Sudden after minor fall
- Night Pain
- Moderate
- Key Discriminating Feature
- MRI shows linear fracture in proximal tibia
- Onset
- Variable, often insidious
- Night Pain
- Variable
- Key Discriminating Feature
- Risk factor history, multifocal lesions on MRI
Investigations
Imaging Protocol for Suspected SONK
Views: AP, Rosenberg (45-degree flexion PA), lateral, skyline
Look for: Subtle flattening of medial femoral condyle, subchondral sclerosis, early joint space narrowing. Normal X-ray does not exclude early SONK.
Clinical correlation: Compare with contralateral knee. Varus alignment greater than 5 degrees increases suspicion.
Sequences: Coronal and sagittal T1, T2, STIR, proton density
Key measurements: Lesion width (percentage of condyle), area in square centimetres, depth of collapse in millimetres, extent of bone marrow oedema.
Additional findings: Rule out meniscus tear, ligament injury, or secondary ON pattern (serpiginous lesions).
Indication: Planning high tibial osteotomy or UKA
Measurement: Mechanical axis deviation, medial proximal tibial angle, lateral distal femoral angle.
Decision impact: Determines whether corrective osteotomy can unload the lesion or whether arthroplasty is required.
Always measure lesion size on the coronal slice of maximum width. Calculate percentage of the medial condyle width. A lesion involving greater than 50 percent of the condyle width or with greater than 2 mm collapse has a high likelihood of progression and should be counselled toward surgical options early. Small lesions (less than 40 percent) with minimal oedema may be observed with protected weight bearing and repeat MRI at 8-12 weeks.

The Reversible Mimic: Transient Bone Marrow Oedema Syndrome
Not every painful older knee with bone marrow oedema is SONK. Transient bone marrow oedema syndrome (transient osteoporosis) of the knee is a self-limiting, reversible cause of pain and oedema that must not be over-treated as if it were a collapsing insufficiency fracture.
- MRI distinction: transient bone marrow oedema syndrome shows diffuse oedema without a discrete subchondral fracture line, without a focal subchondral low-signal collapse zone, and without articular flattening - whereas SONK has the focal subchondral fracture line and (later) collapse. A subchondral band of marked hypointensity adjacent to the endplate favours an insufficiency fracture (SONK), not transient oedema.
- Natural history: transient bone marrow oedema syndrome resolves spontaneously over weeks to months with protected weight bearing and analgesia; it does not progress to collapse. It can be regional or migratory (the hip is the classic site).
- Why it matters: misreading transient oedema as SONK risks unnecessary surgery; misreading SONK as transient oedema risks allowing a preventable collapse - so look specifically for the subchondral fracture line.
Q: An older patient has knee pain with diffuse bone marrow oedema on MRI but no subchondral fracture line or flattening - what is the likely diagnosis and its course? A: Transient bone marrow oedema syndrome (transient osteoporosis) of the knee - a self-limiting, reversible entity that resolves over weeks to months with protected weight bearing and does not collapse. The key discriminator from SONK is the absence of a focal subchondral fracture line; mistaking it for SONK risks unnecessary surgery.
Management Algorithm
Conservative Management (Small Lesions, Early Stage)
Indications: Lesion width less than 40 percent of condyle, collapse less than 2 mm, patient compliant with protected weight bearing.
Protected Weight Bearing Protocol
Touch weight bearing with crutches or walker. Avoid full weight bearing to prevent propagation of subchondral fracture.
Partial weight bearing (50 percent) with gradual increase if pain allows. Repeat radiographs or MRI to assess healing.
Full weight bearing as tolerated once pain subsides and imaging shows resolution of oedema or stabilisation of lesion.
Some centres use intravenous zoledronic acid or oral alendronate in early SONK to reduce bone turnover and support healing of the subchondral fracture. Evidence is limited to small series but the rationale is biologically plausible given the insufficiency fracture mechanism. Discuss with patient as off-label use.
STAGETreatment Selection by Stage
Hook:STAGE guides whether to protect, unload or replace the knee!
Complications
- Subchondral collapse of the weight-bearing condyle (the pivotal event converting a potentially reversible lesion into an irreversible one)
- Secondary osteoarthritis of the medial compartment, often rapid once collapse occurs
- Progressive varus malalignment increasing medial compartment load in a vicious cycle
- Chronic pain and functional decline with antalgic gait and reduced walking distance
- Association with meniscal (posterior root) tears, which both predispose to and accelerate the overload
- High tibial osteotomy: delayed/nonunion, loss of correction, over- or under-correction, intra-articular fracture, common peroneal nerve injury, hardware irritation
- Unicompartmental knee arthroplasty: aseptic loosening, polyethylene wear, bearing dislocation (mobile-bearing designs), progression of disease in the other compartments, persistent pain, periprosthetic fracture, conversion to TKA
- Bisphosphonate therapy (off-label adjunct): rare atypical femoral fracture and osteonecrosis of the jaw with prolonged use
- Prolonged protected weight bearing: deconditioning, falls and venous thromboembolism risk in the elderly
Subchondral collapse greater than 2 mm and a lesion involving more than ~50 percent of the condylar width are the key tipping points: beyond them, conservative care reliably fails and joint-preserving osteotomy outcomes become unpredictable. Counsel toward arthroplasty (or osteotomy in the young) before, not after, irreversible collapse and secondary osteoarthritis supervene.
Guidelines, Registries & Global Practice
- SONK incidence increasing with ageing population and greater MRI access worldwide
- Medial condyle predominance consistent across all ethnic groups and regions
- Female predominance 2-3:1 in every published series from Europe, Asia, North America
- Under-diagnosis common in low-resource settings where MRI is not readily available
- High-resource: Early MRI, lesion size quantification, bisphosphonate protocols, UKA or osteotomy in specialist centres
- Limited-resource: Diagnosis often delayed until radiographic collapse, protected weight bearing with crutches, TKA when advanced
- Universal principle: Lesion size and collapse depth remain the critical decision factors regardless of geography
- Surgery availability: UKA and osteotomy concentrated in high-volume arthroplasty centres globally
- Diagnosis Emphasis
- MRI for all unexplained medial knee pain in elderly
- Conservative Care
- Protected weight bearing 6-12 weeks, consider bisphosphonates
- Surgical Threshold
- Greater than 40 percent lesion or greater than 2 mm collapse
- Diagnosis Emphasis
- Clinical suspicion plus MRI staging
- Conservative Care
- Non-operative first line for small lesions
- Surgical Threshold
- Individualised, lesion size and patient factors
- Diagnosis Emphasis
- Differentiate SONK from secondary ON early
- Conservative Care
- Weight-bearing restriction, metabolic workup
- Surgical Threshold
- Osteotomy in younger, UKA/TKA in older
- Diagnosis Emphasis
- High incidence in elderly Asian females noted
- Conservative Care
- Similar conservative protocols
- Surgical Threshold
- UKA popular due to smaller stature and lower demand
There is no dedicated SONK registry. Data are derived from national joint registries (NJR, AJRR, AOANJRR) reporting outcomes of UKA and TKA performed for osteonecrosis, and from small prospective series on conservative care and osteotomy. The evidence base remains level 3-4. Key principle across all guidelines: measure lesion size accurately on MRI and base treatment on percentage of condyle involved and depth of collapse.
Controversies & Areas of Uncertainty
Small series suggest zoledronic acid or alendronate may accelerate healing of subchondral fractures in SONK, but no high-quality randomised trials exist. Use remains off-label and centre-dependent.
Six to twelve weeks is conventional, but exact duration and degree of unloading lack high-level evidence. Serial MRI at 8-12 weeks is increasingly used to guide progression.
Patients aged 60-70 with medium-sized lesions and mild collapse present a decision dilemma. Some surgeons favour joint preservation with osteotomy, others prefer the reliability of UKA. Shared decision-making with patient activity goals is essential.
Limited evidence supports core decompression or bone grafting for early SONK. Most centres reserve these for rare cases in very young patients or as part of research protocols.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old woman presents with sudden onset severe medial right knee pain for 3 weeks. No history of trauma or steroid use. Pain wakes her at night. Weight-bearing radiographs are normal. MRI shows a 2.8 square centimetre lesion of the medial femoral condyle with bone marrow oedema but no subchondral collapse. The lesion involves 32 percent of the condylar width. What is your diagnosis and initial management?”
“A 72-year-old active man presents with 4-month history of progressive medial knee pain. He recalls a minor twisting injury 5 months ago. Radiographs show 3 mm collapse of the medial femoral condyle with varus alignment of 7 degrees. MRI demonstrates a 6.2 square centimetre lesion involving 58 percent of the condylar width with a fluid-filled cleft. The lateral compartment and patellofemoral joint are preserved and he has an intact ACL. What surgical options would you discuss?”
Key Demographics and Presentation
- Elderly female (greater than 60 years), sudden medial knee pain without trauma
- Night pain is characteristic, distinguishes from meniscus tear or OA flare
- Greater than 90 percent involve the medial femoral condyle weight-bearing surface
- No systemic risk factors (steroids, alcohol, sickle) - these suggest secondary ON
MRI Staging and Sizing
- Stage 1: Normal X-ray, bone marrow oedema only - high healing potential
- Stage 2-3: Subchondral lucency or collapse - measure width percentage and depth
- Small lesion (less than 40 percent width, less than 3.5 cm2) - conservative trial
- Large lesion (greater than 50 percent) or greater than 2 mm collapse - surgical candidate
Differential Diagnosis
- Secondary ON: multifocal, serpiginous lesions, risk factor history
- Medial meniscus tear: mechanical symptoms, twisting injury, MRI meniscal signal
- Insufficiency fracture tibia: linear fracture line in proximal tibia on MRI
- Primary OA: gradual onset, joint space narrowing and osteophytes on X-ray
Treatment Thresholds
- Conservative: touch weight bearing 6-12 weeks, consider bisphosphonate
- High tibial osteotomy: younger active patient, correctable varus, preserved lateral compartment
- UKA: older patient, large lesion or collapse, intact ACL and lateral cartilage
- TKA: multicompartment disease, ligament deficiency, inflammatory arthritis
Prognosis and Follow-up
- Small lesions: greater than 80 percent heal with conservative care
- Large lesions with collapse: high progression risk, counsel early for surgery
- UKA survival in SONK: 90-93 percent at 10 years when selection criteria met
- Serial MRI at 8-12 weeks for conservatively managed patients to detect collapse
Evidence Base
Original description of spontaneous osteonecrosis of the knee
- Seminal paper that first described spontaneous osteonecrosis of the knee as a distinct entity affecting predominantly the medial femoral condyle in older patients
- Characterised the classic presentation of sudden-onset knee pain without preceding trauma
- Documented radiographic progression and used biopsy/radionuclide assessment in its evaluation
Subchondral insufficiency fracture as the cause of SONK
- Histological study of 14 resected femoral condyles with SONK showing subchondral fracture as the primary event
- No evidence of primary vascular occlusion in early lesions
- Fracture callus and granulation tissue consistent with reparative response to mechanical failure
- Supported the insufficiency fracture hypothesis over avascular necrosis theory
Unicompartmental knee arthroplasty for osteonecrosis (spontaneous and secondary)
- Retrospective review of 30 patients (31 knees) undergoing UKA for osteonecrosis - 21 spontaneous and 10 secondary; mean age 71, mean follow-up 7 years (range 3 to 16)
- Reliable pain relief and functional improvement (Knee Society scores) in 30 of 31 knees (96 percent)
- Appropriate lower-limb mechanical axis restored in 27 knees (88 percent)
- Kaplan-Meier survivorship 96.7 percent at 12 years
Subchondral insufficiency fracture of the knee: review of current concepts and radiological differential diagnoses
- MRI features distinguish SONK from other causes of bone marrow oedema
- Lesion size and collapse depth on MRI are the main prognostic factors guiding treatment